
Abstract
Ongoing payment reform in dialysis necessitates better patient outcomes and lower costs. Suggested improvements to processes of care for maintenance dialysis patients are abundant; however, their impact on patient-important outcomes is unclear. This systematic review included comparative randomized controlled trials or observational studies with no restriction on language, published from 2000 to 2014, involving at least 5 adult dialysis patients who received a minimum of 6 months of follow-up. The effect size was pooled and stratified by intervention strategy (multidisciplinary care [MDC], home dialysis, alternate dialysis settings, and electronic health record implementation). Heterogeneity (I2) was used to assess the variability in study effects related to study differences rather than chance. Of the 1988 articles screened, 25 international studies with 74,833 maintenance dialysis patients were included. Interventions with MDC or home dialysis were associated with a lower mortality (hazard ratio [HR] = 0.72, 95% confidence interval [CI] 0.61, 0.84, I2 = 41.6%; HR = 0.57, 95% CI 0.41, 0.81, I2 = 89.0%; respectively) and hospitalizations (incidence rate ratio [IRR] = 0.68, 95% CI 0.51, 0.91, I2 = NA; IRR = 0.88, 95% CI 0.64, 1.20, I2 = 79.6%; respectively). Alternate dialysis settings also were associated with a reduction in hospitalizations (IRR = 0.41, 95% CI 0.25, 0.69, I2 = 0.0%). This systematic review underscores the importance of multidisciplinary care, and also the value of telemedicine as a means to increase access to providers and enhance outcomes for those dialyzing at home or in alternate settings, including those with limited access to nephrology expertise because of travel distance.
Introduction
S
These modifications to reimbursement were partly motivated by large-scale epidemiologic research showing variability in the cost of care, mortality, and other outcomes across facilities and countries. 1,2 These studies suggest that variations in outcomes may not always be explained by disease severity, and may instead be related to differences in the processes of care. 1 Thousands of life-years could be gained by better adherence to best practices. 2
The Medicare ESRD Managed Care Demonstration Operations carried out by large health systems demonstrated improved outcomes and costs based on the implementation of multiple layers of interventions targeting high-risk patients. 3 However, there is insufficient methodological detail to determine which interventions add the most value in terms of patient outcomes without being prohibitively expensive. Similar concerns have been raised about other Medicare-funded quality initiatives. 4
As dialysis facilities seek to enhance care delivery, meet quality standards and manage reimbursement, information on effective models of dialysis care is necessary to improve value-based care. This systematic review and meta-analysis aims to summarize the literature on models of care, targeting critical patient-important outcomes for maintenance dialysis patients: hospitalizations and mortality.
Methods
This systematic review followed an a priori established protocol and is reported according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 5 The study was approved by the Mayo Clinic Institutional Review Board as a minimal risk study.
Study eligibility
Eligible studies met the following criteria: (1) original comparative studies identified as a randomized controlled trial (RCT) or an observational study published between January 2000 and October 2014; (2) studies that evaluated at least 5 maintenance dialysis patients aged >18 years; (3) studies including at least 6 months of follow-up. Exclusion criteria: (1) published case reports, letters, comments, and reviews; (2) study design including only in vivo and/or in vitro studies; (3) studies limited to high-risk patients such as patients with HIV, in the intensive care unit, or cancer patients; (4) studies limited to patients with chronic kidney disease progressing to ESRD; (5) studies reporting only on palliative care for ESRD.
Literature search
Controlled keywords, such as ESRD, mortality, and hospitalizations, were used to search Ovid MEDLINE, Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus databases. There were no restrictions on language or country of origination. The literature search was designed and conducted by an experienced librarian with input from the investigators (see online Supplementary Fig. S1; Supplementary Data are available online at
Study selection
Study selection was completed over 2 levels of screening (Fig. 1). During the first level of screening, 2 reviewers, working independently, screened titles and abstracts. Disagreements were resolved by reviewer consensus. If a study was believed relevant, the full-text version was independently reviewed by 2 reviewers for further assessment. Studies were selected for inclusion upon reviewer agreement, with discrepancies resolved by reviewer consensus.
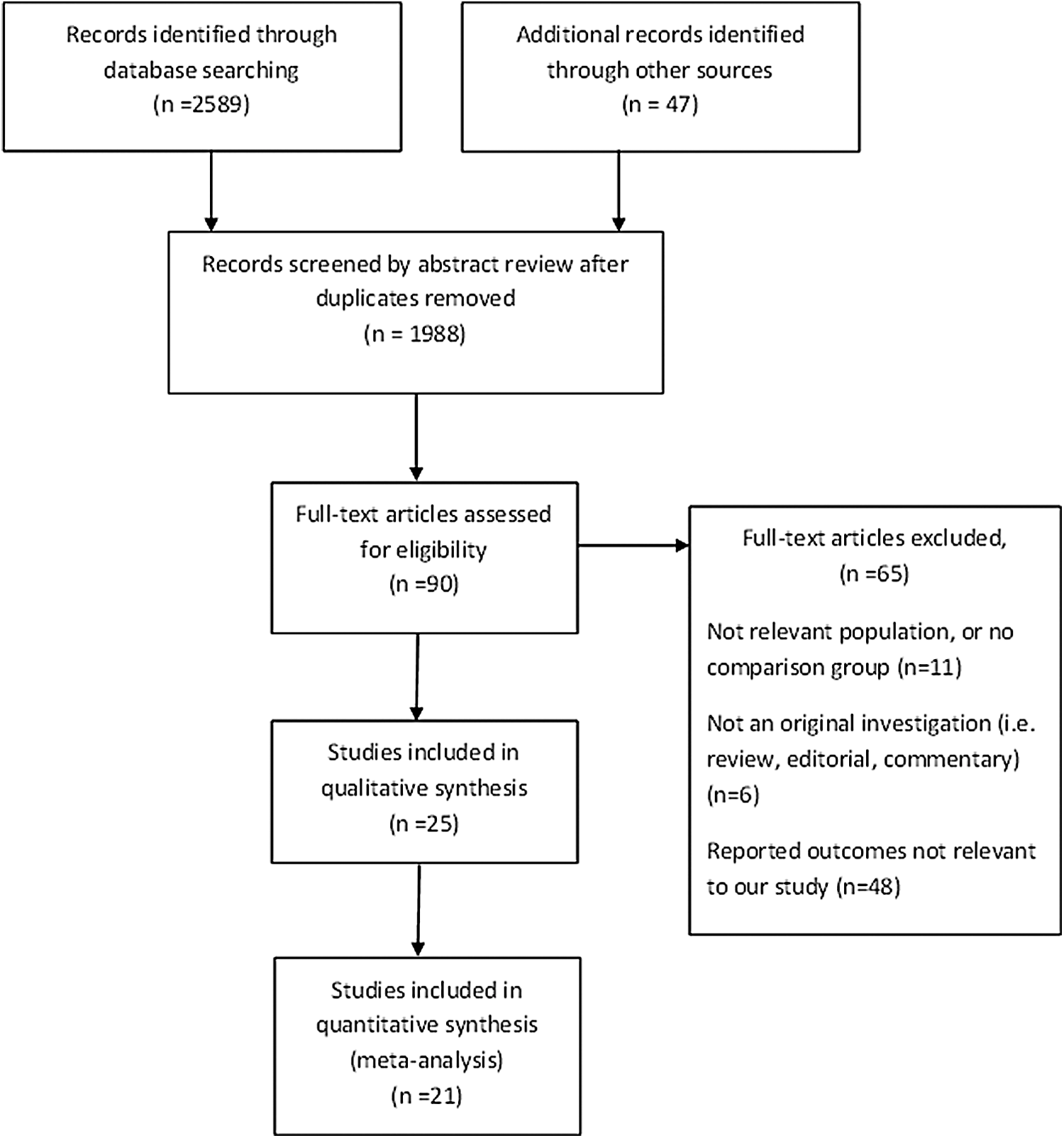
PRISMA flow diagram of study selection.
Data abstraction
Standardized forms for abstraction were developed and piloted. Two reviewers independently abstracted information on the care setting, including country; single versus multiple site; home, primary, or specialty care; study design; intervention (described change to model of dialysis care, not including medication or nutrition changes); patient characteristics; dialysis modality for the intervention group and comparison group; and outcome measures. When differences in collected data were identified, the authors discussed and resolved discrepancies by consensus.
Statistical analysis
A meta-analysis was conducted to evaluate the effect of interventions on mortality and hospitalizations. Based on data reporting methods, the study team extracted or calculated a relative effect measure from each study (hazard ratio [HR], which is the relative likelihood of the outcome in the intervention group compared to the control group over time; incidence rate ratio [IRR], which is the ratio of the proportion at risk in the intervention group who have the outcome within the time at risk to the proportion at risk in the control group who have the outcome within the time at risk control; relative risk [RR], which is the ratio of the probability of having the outcome in the intervention group to the probability of having the outcome in the control group.
The effect size was pooled across studies and stratified by intervention strategy (multidisciplinary care [MDC], home dialysis, alternate dialysis settings, and electronic health record [EHR] implementation) using Der-Simonian and Laird random-effects models. 6 The study team tested whether the effect size differed between HR and RR. Studies were grouped as MDC if terms such as multidisciplinary or team-based care were used to describe the intervention. Studies describing dialysis administration in a nonclinical setting, such as home or a remote or satellite location, were grouped as home hemodialysis and alternate dialysis settings, respectively. One study described the implementation of an EHR whereby all clinical, administrative, and financial information was immediately accessible; this study was evaluated separately.
The team examined variability in evaluated intervention effects across included studies by calculating heterogeneity and assessing methodological quality as will be described. Heterogeneity, or the proportion of variation in intervention effects among included studies that is related to differences between studies rather than chance, was measured with reported I2, in which I2 greater than 50% suggests substantial heterogeneity. 7 All analyses were conducted using STATA version 13 (StataCorp LP, College Station, TX).
Methodological quality (risk of bias)
Risk of bias was assessed for each included study to understand the influence of differences in study methodology on variability in results. The Cochrane risk of bias tool was used for RCTs to evaluate bias within the domains of selection, performance, detection, attrition, and reporting by assessing allocation concealment, blinding of participants or personnel, blinding of outcome assessment, attrition, incomplete outcome data, incomplete data, and selective outcome reporting. 8 The Newcastle-Ottawa Scale, a tool designed to assess the quality of nonrandomized studies based on selection and comparability of the study groups as well as the ascertainment of either the exposure or outcome of interest, was used for observational case-control and cohort studies. 9 Both are well-known and validated tools to assess risk of bias. The methodological quality of the studies was assessed by 2 reviewers independently, with disparities resolved by consensus.
Results
The search strategy revealed 1988 references after removing 648 duplicates. An additional 47 references were identified by a secondary manual search. The abstract review resulted in 90 articles screened with a full-text review (Fig. 2). Studies were excluded if the study population was not relevant, there was no comparison group, the study was not an original investigation, or if the study did not report relevant outcomes. Overall, 25 studies with 74,833 (range 12 to 26,366) maintenance dialysis patients in a variety of settings were included (Table 1). Most included studies (71%) were conducted in the United States; the remaining studies (29%) were conducted in Canada, Europe, China, Australia, and New Zealand.
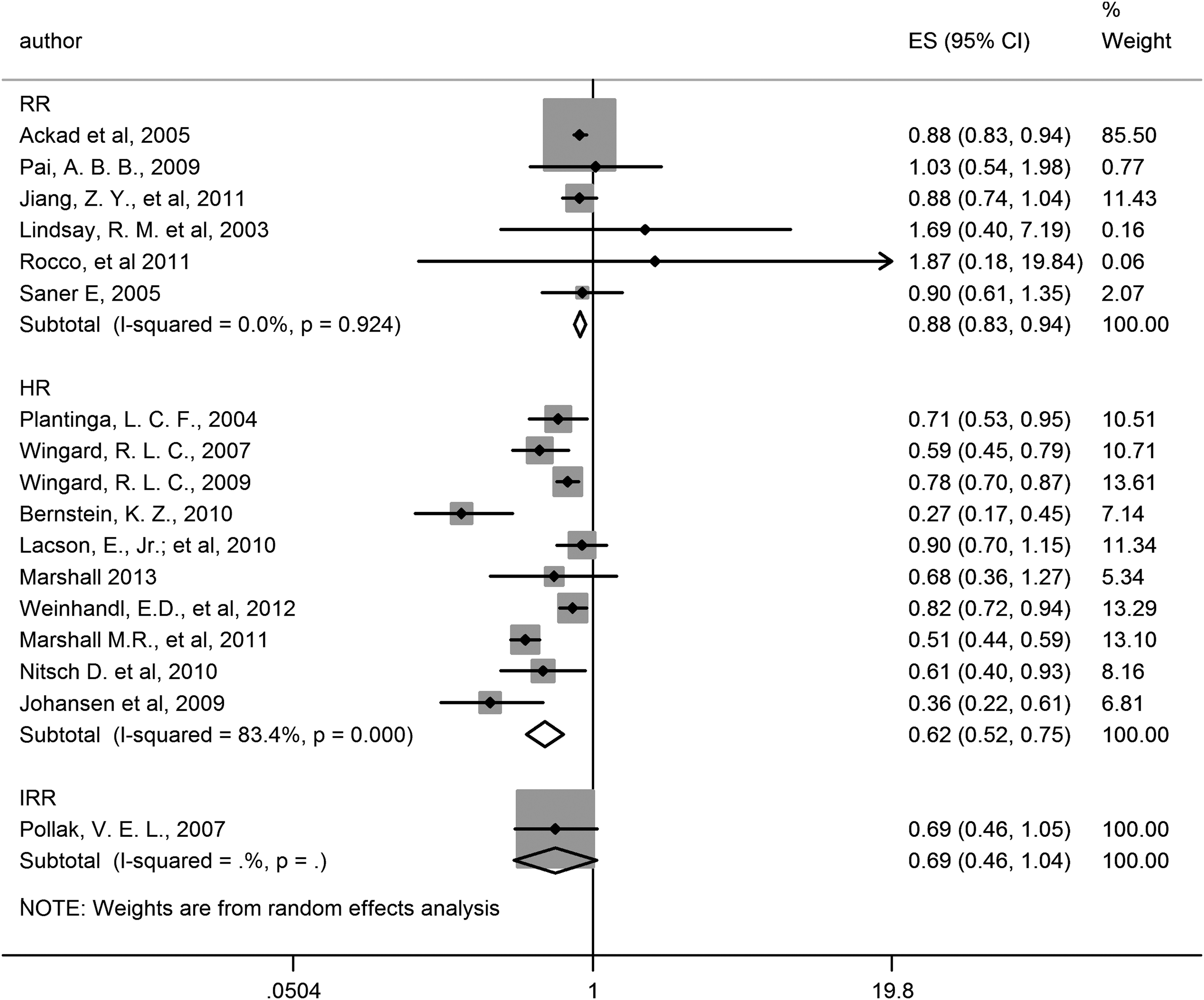
Meta-analysis of mortality associated with dialysis care interventions. Vertical line indicates no effect, squares and horizontal lines indicate HR and associated 95% CIs for each study. Diamond indicates pooled effect. CI, confidence interval; ES, estimate; HR, hazard ratio; IRR, incidence rate ratio, RR, relative risk.
% per 10,000 py.
avg, average; CI, confidence interval; EHR, electronic health record; FHD, facility dialysis; HD, hemodialysis; HHD, home hemodialysis; HR, hazard ratio; IRR, incidence rate ratio; PC, prospective cohort, PD, peritoneal dialysis; ppy, per patient year; py, patient years; RC, retrospective cohort; RCT, randomized clinical trial; RR, risk ratio; SD, standard deviation; USRDS, US Renal Data System; yr, year.
Outcomes
The pooled MDC, home hemodialysis, alternate dialysis settings, and implementation of EHR intervention strategies showed a reduction in mortality (HR = 0.62, 95% confidence interval [CI] 0.52, 0.75, I2 = 77.7%) and hospitalizations (IRR = 0.88, 95% CI 0.63, 1.10, I2 = 81.3%), shown in Figures 3 and 4. The subgroup analysis is reported in Table 2, showing the MDC studies to be associated with a significant reduction in mortality (HR = 0.72, 95% CI 0.61, 0.84, I2 = 41.6%).
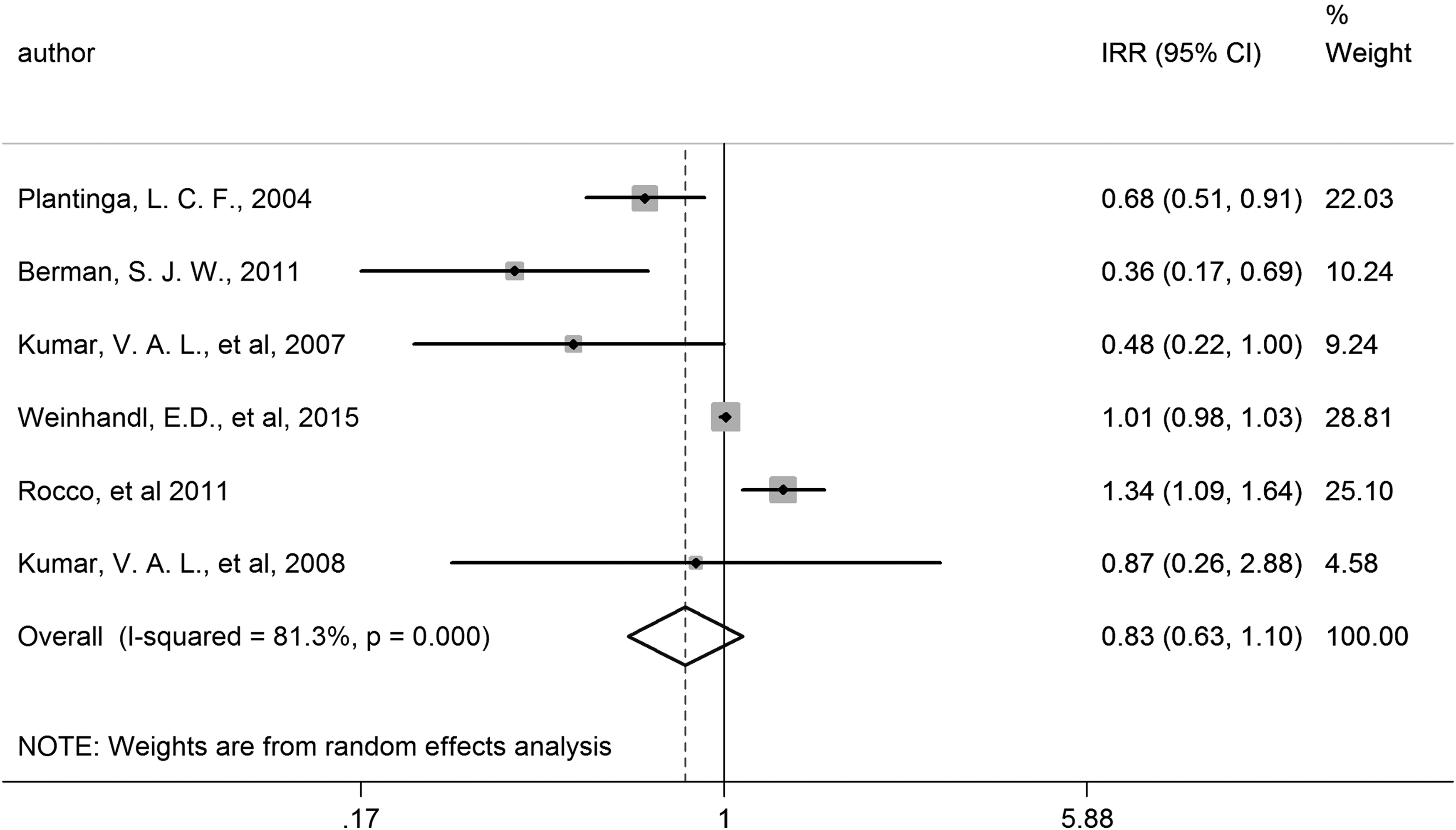
Meta-analysis of hospitalizations associated with dialysis care interventions. Vertical line indicates no effect, squares and horizontal lines indicate HR and associated 95% CIs for each study. Diamond indicates pooled effect. CI, confidence interval; HR, hazard ratio; IRR, incidence rate ratio.
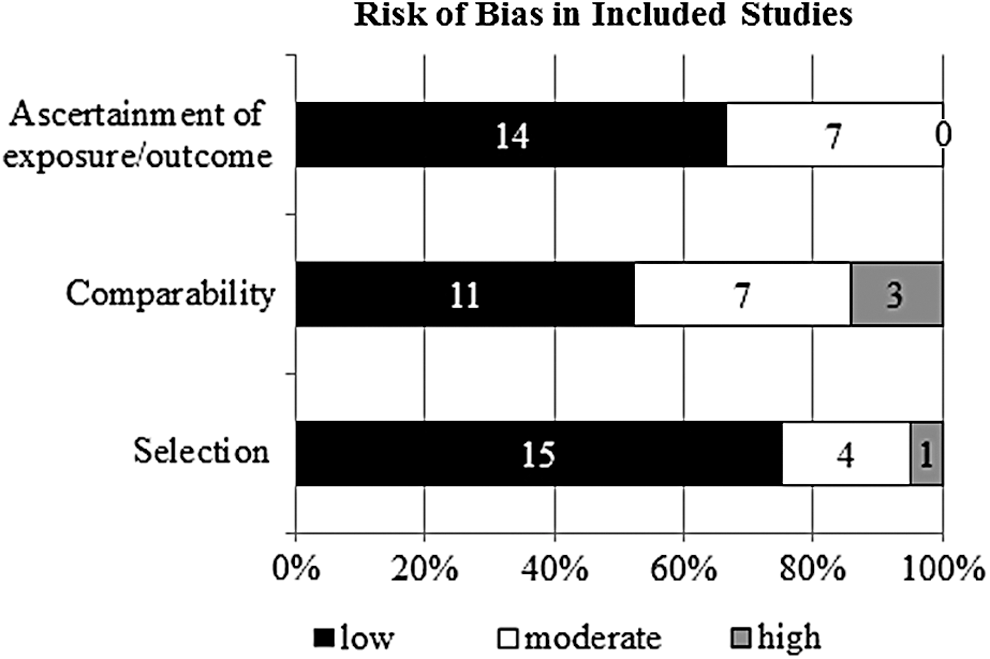
Risk of bias in observational studies. Number of studies with low risk, moderate risk, and high risk is shown within bars.
CI, confidence interval; EHR, electronic health record; HR, hazard ratio; I 2, heterogeneity; IRR, incidence rate ratio; MDC, multidisciplinary care; RR, relative risk.
The pooled estimates of home hemodialysis, alternate dialysis settings, and the outcome measure for EHR implementation also favored the intervention, although these were not statistically significant (Table 2). One study of MDC showed a reduction in hospitalizations (IRR = 0.68, 95% CI 0.51, 0.91), as did the pooled estimate of 5 home hemodialysis studies (IRR = 0.88, 95% CI 0.64, 1.20, I2 = 79.6%; Table 2).
Methodological quality (risk of bias)
Of the 25 studies included, 4 were RCTs and 21 were cohort studies. Follow-up ranged from 9 to 240 months. The distribution of methodological quality indicators in the included studies is illustrated in Figure 4.
RCTs
Among the 4 RCTs included, 2 had adequate concealment and a defined method of randomization. 10,11 The other 2 studies reported randomization, although their methods were not clearly defined. 12,13 Two trials described blinding of study personnel and/or outcome assessors. None of the trials had apparent selective outcome reporting and all had less than a 9% attrition rate.
Cohort studies
Six retrospective cohort studies 14 –19 and 15 prospective cohort studies 16,20 –33 were included. The majority of these studies were representative of maintenance dialysis patients in the community. Four studies that focused on home hemodialysis included a select cohort of patients. 15,18,22,23 Most studies had a comparison group from the same community as the exposed cohort and ascertained the exposure by secure records (clinical or registry). One study used matched comparison cohorts from a national database. 15 Comparability was adequate, with most studies accounting for important factors including recovery, transplant, and change of dialysis modality; 6 studies did not account for these. Mortality and hospitalizations were assessed by record linkage in all studies and estimates were adjusted for important confounders such as demographics, mode of dialysis, cause of ESRD, and comorbidities.
Intervention strategies
Four primary intervention strategies were examined and are described in Table 1. These include (1) MDC, (2) home hemodialysis, (3) alternate dialysis settings, and (4) EHR implementation.
MDC
Seven international studies with an MDC intervention were reviewed. These multidisciplinary teams included staff nurses or dietitian case managers integrated with an MDC team 30,32,33 ; scheduled monthly sit-down meetings of the MDC team to review medical records and discuss long- and short-term care plans 29 ; a bimonthly, in-depth drug review with a pharmacist who consulted with the MDC team 10 ; and a monthly vascular access blood flow monitoring. 20,27 The studies involved nephrologists, nurses, and often social workers and dietitians. The studies reported positive effects on mortality and hospitalization, and stressed the importance of MDC team-based care to optimize patient outcomes.
Home hemodialysis
The 13 home hemodialysis studies showed better outcomes compared to center hemodialysis, peritoneal dialysis, and satellite centers. 18,19,25,28,31,34 Many of these also incorporated nocturnal hemodialysis, which has long been shown to have better outcomes regardless of location 11,15,16,24,35,36 Two home hemodialysis studies included telemedicine, or remote monitoring, and reported dramatic improvements in outcomes. 12,13
Berman et al found that the addition of a nurse-clinician to remotely monitor the health status of high-risk home hemodialysis patients reduced the number of hospitalizations by more than half compared to high-risk home hemodialysis patients who did not have nurse-clinician oversight of their care. 12 They also noted a decrease in frequency of patient and nurse contacts for clinical issues over time, suggesting patient empowerment and stronger self-management resulting from remote therapy, combined with clinical oversight and ongoing communication with the nurse-clinician. Similarly, Gallar et al reported that home hemodialysis patients with telemedicine visits had a hospitalization rate that was half that of home hemodialysis patients without telemedicine visits. 13 They also described the additional benefit of added surveillance, error avoidance, and an increase in focused attention from nurses with teleconsultation–difficult to achieve in a busy multiple-bed hospital setting.
Alternate dialysis settings
As already described, Lacson et al showed the benefit of long duration nocturnal hemodialysis, which reported fewer hospitalizations compared to conventional hemodialysis. 16 The effect on mortality was not as pronounced. Marshall et al found that a community house for hemodialysis as a submodality to home hemodialysis resulted in lower costs and mortality compared to home hemodialysis, facility hemodialysis, or even peritoneal dialysis. 26
The remaining 2 studies investigated satellite clinics to extend care to patients unable to receive home hemodialysis or living in more remote/rural areas without access to similar health care resources as patients in more urban settings. 14,21 Jiang and colleagues found that a satellite option offered convenience and added comfort for patients living remotely–with standardized staff training to provide care similar to the provincial centers–significantly improved rates of mortality. 21 An important component of these alternate settings is access to MDC, including thorough remote monitoring, as suggested by Bernstein et al who reported a greater positive effect on mortality than the other studies. 14
EHR implementation
Pollak and Lorch compared outcomes of 1790 patients on chronic maintenance hemodialysis in 3 dialysis units (A, B, C) managed by the same institute, but which differed in the number and type of providers at each site. 17 The first site (A) was staffed with 8 full-time salaried nephrologists, who also care for general nephrology and transplant patients, participate in medical education teaching, and clinical research; and 2 nurse practitioners. The second site (B) was staffed with 1–2 salaried nephrologists, 2–5 private practice nephrologists, and 1 nurse practitioner. The third site (C) was staffed with 3 private practice nephrologists. The authors noted overall and unit-specific decreases in mortality and hospitalizations over time, which was even more substantial over time when compared to mortality data for patients with similar characteristics from a national ESRD data set. The authors suggested the availability of complete, accurate, timely information, which facilitated clinical decision making, benefited survival outcomes.
Quality of the evidence (certainty in the estimates)
Using the Grading of Recommendations, Assessment, Development, and Evaluation approach, the quality of evidence supporting the effect of models of dialysis care on mortality and hospitalization is low because of the nonrandomized nature of most of the studies. 37
Discussion
Despite a comprehensive review of the literature, only a small number of studies were found that evaluated the impact of different models of dialysis care on patient-important outcomes. No comparative effectiveness studies were found that evaluate models of dialysis care delivery in terms of quality, safety, and cost. Although a vast amount of research on dialysis care exists, most of these studies evaluate specific medications and techniques, or are quality initiatives targeting process measures or short-term surrogate outcomes such as biochemical or physiological markers, access duration, and fluid and volume management. The studies included in this systematic review comprised multiple intervention strategies and provider types, making summative statements and quantitative pooling of outcomes challenging.
Despite this, the study team found that MDC, whether involving home, alternative, or inpatient dialysis settings, is important in improving patient-important outcomes. Prior studies have described the positive impact of MDC on patients with chronic kidney disease. 38 Surprisingly, using the present study's criteria for inclusion, a limited number of studies were found that measured the impact of MDC once a patient has progressed to ESRD. The majority of MDC studies included in this review provided evidence of effectiveness with a variety of provider types, roles, and settings; however, the multifaceted and variable nature of these interventions made it difficult to highlight the most beneficial components.
Interventions that support patient self-care at home or in an alternate dialysis setting with telemedicine also are associated with improved outcomes. Patient empowerment through self-care tools has been recognized as a strategy to improve outcomes in chronic disease. 39,40 These tools use enhanced technology to improve communication between patients and providers, thereby increasing efficiency by tracking health status and access to care.
Patients and providers in the Gallar et al study reported that telemedicine successfully replaced clinic consultation more than 90% of the time, resulting in significantly lower hospitalization rates. 13 Similarly, Whitten and Buis reported that telemedicine increased access to health care with successful maintenance of the patient-provider relationship. 41 Other reviews reporting the effects of telemonitoring for chronic disease requiring close management have reported similar results. 42,43
Such tools are invaluable in promoting health behavior change and self-management skills for maintenance dialysis patients who require consistent and just-in-time access to care, particularly for patients who reside further away from clinics, which has been correlated with poor outcomes. 44 Although only 1 study focused on the impact of the EHR, it found benefit in improved outcomes across settings and providers, suggesting the benefit of a common EHR allows the sharing of information between practice sites and providers.
There are several limitations to this systematic review. First, the study team chose to focus on hospitalizations and mortality as the patient-important outcomes of interest. The team was not able to assess other valid patient-important outcomes such as infection and emergency department visits because of the limited scope of the included studies. The team found several interventions that were effective in improving mortality and hospitalizations; however, this evidence needs to be interpreted with caution. High heterogeneity is expected when pooling observational studies with varying populations, settings, and study designs. Although the study team was able to group articles by intervention strategy, they were not able to fully explore heterogeneity because of wide variation in populations, treatment settings, providers, mode of dialysis, and intervention strategies.
Also, the possibility of publication bias favoring positive studies is a common threat to the validity of meta-analysis of observational studies. The study team was unable to conduct quantitative tests (ie, funnel plots) for publication bias because of the small number of included studies per analysis and the variation in intervention strategies. Similarly, the team acknowledges the possibility of reviewer bias, which was mitigated through a pilot phase of abstraction forms, independent abstraction, and resolution of differences in abstraction through consensus. Finally, some interventions contained features that may not be easily replicated in other settings (ie, because of staffing or technological resources).
Strengths of this review include the a priori design, the comprehensive search of several databases, and the duplicate process of study selection and appraisal with good interrater reliability for data collection and synthesis.
To the study team's knowledge, this is the first systematic review to summarize models of dialysis care targeting patient-important outcomes. There is a paucity of high-quality evidence to guide dialysis practice reform to meet the challenges of new reimbursement standards. This systematic review underscores the importance of MDC, and also the value of telemedicine as a means to increase access to providers and enhance outcomes for those dialyzing at home or in alternate settings, including those with limited access to nephrology expertise because of travel distance. The consideration of treatment burden, the importance of a patient and caregiver perspective, and improved coordination of clinical knowledge and care will inform policy and practice that is patient-centered and that enhances the value of care by improving outcomes and decreasing costs. 45
The proposed Medicare Telehealth Parity Act supports expanding the use of telemedicine services for home dialysis patients, and broadens the reach for services seemingly limited by face-to-face contact. 45 These findings support this decision. Similarly, connection through an EHR enables the timely flow of information and increases the provider's relationship with patients. Future work to improve the effectiveness of care delivered to ESRD patients also may benefit from consideration of the demands that complex chronic disease and associated health care interventions place on patients and their caregivers. The knowledge gained by the ongoing discoveries made during the creation of the alternative payment models, specifically ESCOs, will better inform changes to improve the care of those with ESRD, focusing on patient-centered outcomes while decreasing the overall cost of care.
Footnotes
Author Disclosure Statement
Drs. Ahmed, Wang, Suarez, Hickson, Williams, Shah, Murad, and Thorsteinsdottir, and Ms. Ramar, Mr. Chawla, and Ms. Farrell declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The corresponding author acknowledges that this manuscript represents an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained. The authors received the following financial support: This research was made possible by the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.