
Abstract
In recent years, neonatal abstinence syndrome (NAS) rates have increased rapidly across the United States, rising from 1.2 (2000) to 5.8 (2012) per 1000 hospital births annually. Because most NAS infants are treated in an intensive care setting, associated hospital charges are high and continue to escalate, rising on average from $39,400 in 2000 to $66,700 in 2012. An innovative NAS treatment program, which includes early-initiated methadone therapy, rooming-in, and combined inpatient/outpatient weaning in a low-acuity nursery, has been in place since 2003 at a large Southeastern hospital. The program has proven safe, effective and low cost for treating infants of ≥35 weeks gestational age whose mothers used long-acting opioids. Given that 81% of NAS cases in the United States are funded by Medicaid programs and that the cost burden is rising rapidly, researchers considered the potential saved charges associated with implementing the same program in other hospitals state- and nationwide. Researchers used regression models to project state and national NAS birth rates from 2015–2025 and to predict future NAS charges under current treatment protocols. Three scenarios were developed to compare the potential saved charges of implementing the innovative NAS treatment program across the state and nation with assumptions related to the percent of NAS infants eligible for the program, percent funded by Medicaid, and fluctuations in average length of stay. The potential saved charges are substantial, creating a compelling case for policy makers and hospitals in the pursuit of safe, effective, and cost-conscious NAS care.
Introduction
N
The NAS epidemic is a significant public health problem both because of the severity of the neonate's medical withdrawal experience and because the majority of NAS cases are covered by Medicaid, a publicly provided state health insurance program. 2 –8 Because many infants are managed in neonatal intensive care unit (NICU) environments, hospital charges for NAS care are increasing nationally. Patrick et al estimated that the mean US hospital charges per infant discharged with NAS rose from $39,400 in the year 2000 to $66,700 in 2012. 2,3 In addition, 2012 data show that pharmacologically-treated NAS infants had mean hospital charges totaling $93,400 and a mean length of stay of 23 days. 3 With an estimated 23,000 NAS infants born annually, charges would total $1.5 billion on average.
Medicaid was the primary payer for 81% of cases. 3 Medicaid typically reimburses approximately 50% of hospital charges. Data comparing reimbursement rates for NAS between states was not available, and national literature reporting the financial impact of NAS care is framed in terms of charges, so the figures presented in this paper will be in hospital charges for consistency. With the expansion of Medicaid in some states and the addition of the Children's Health Insurance Program (CHIP) across all states, the vast majority of infants born in the United States are covered by some health insurance policy at birth. 9,10 Federal law allows for considerable flexibility in how individual states manage Medicaid reimbursement. According to the Medicaid and CHIP Payment and Access Commission, there are 3 broad categories of Medicaid reimbursement approaches: per diem, cost reimbursement, and flat rate payment based on diagnosis-related groups (DRGs). 11 In 2004, there was advisement from the Centers for Medicaid & Medicare Services (CMS) that states implement more up-to-date payment methods or develop their own. 12 As such, many states now use a range of algorithms that reimburse hospitals based on DRGs. The move toward reimbursement based on DRGs is argued to be an important step in providing more efficient and cost-effective care. 13,14 Currently in South Carolina, Medicaid reimbursement is per diem for pediatrics but uses a CMS-DRG algorithm for other hospital stays. 12 Given the ongoing evaluation of Medicaid reimbursement and policy pressures to improve effectiveness while stabilizing or reducing costs, it is likely that South Carolina and other states will move to a DRG model for pediatric care in the future.
Geographic variation in incidence across the nation also has been documented. The state of South Carolina falls into one of the country's geographic regions with the highest NAS incidence rates. 3 In South Carolina, the NAS rate was 6 per 1000 newborns in 2013 compared to 3 per 1000 in 2010. 15 Average hospital charges for an NAS newborn in the state were $39,110 in 2013 with an average length of stay of 12.4 days compared to an average of 3.7 days for all state newborns. 15
As states evaluate the allocation of Medicaid funds, the substantial cost burden associated with existing NAS care provides opportunities for states to consider innovative treatment methods. Concerns over rising health care costs, particularly those financed by public payers, provide an impetus to examine the potential cost savings of new treatment programs. Few studies have examined the potential effectiveness of hospital-level interventions related to NAS treatment; however, examples of 2 interventions that have been developed and tested separately include rooming-in care with mothers and combined inpatient/outpatient weaning programs. 16 –21
Considering the number of population health challenges associated with increasing opioid use, new treatment programs that combine improved patient outcomes with cost-effective care must be explored. The Managing Abstinence in Newborns (MAiN) program, an innovative method of NAS treatment, has been developed at Greenville Memorial Hospital (GMH), a large, regional Southeastern hospital. For otherwise healthy newborns at high risk for opioid withdrawal, the treatment program includes early-initiated methadone treatment (within 24 hours of birth), rooming-in with mothers in a low-acuity care setting, and a combined inpatient/outpatient methadone wean. 22 Using state and national data related to NAS cases, the researchers propose different scenarios of potential future saved charges through use of this innovative NAS treatment program. This research has relevance for hospitals, Medicaid, and other payers as well as public policy makers.
Methods
Early treatment program description
The MAiN program was developed in 2003 at GMH-a large (710 beds), regional hospital that is part of a public, not-for-profit academic health care delivery system. GMH experienced an average annual volume of 5221 births from 2006–2014, with approximately 88% of newborns admitted to the mother/baby unit. The MAiN treatment program is based on the theory that neonates who are chronically exposed to long-acting opioids in late gestation are born dependent, because research has demonstrated significant transfer of opioids across the placenta. 23 When started within 24 hours of birth, low-dose methadone may be considered a continuation of long-acting opioid therapy and therefore prevent severe opioid withdrawal and its complications.
To be eligible for the MAiN treatment model, a neonate must be born to a mother who has been taking at least 20 mg of methadone or at least 9 mg of buprenorphine for at least 2 weeks immediately prior to delivery. In addition, the neonate must be at least 35 weeks gestational age and have no other conditions at birth that would require intensive care. Between 2006 and 2014, 472 NAS-diagnosed infants were born at GMH, and approximately 30% of these infants met the MAiN eligibility criteria. The other 70% were excluded as follows. Ninety-three infants (20%) were admitted to neonatal intensive care immediately after delivery for gestational age <35 weeks and/or ill appearing at birth. Methadone was never administered to 201 of the infants (43%) who were exposed in utero to unknown or non-opioid substances. Methadone was initiated after 48 hours of birth in 35 of the infants (7%) because of parent opposition to early treatment or physicians assessed risk of withdrawal as low but symptoms later became severe enough to warrant treatment. A total of 143 patients (30%) were eligible for MAiN, but 26 patients (5%) had to later be transferred to neonatal intensive care for medical illness or complication. Hence, 117 infants (25%) completed the MAiN treatment model.
In the MAiN model, neonates admitted to the low-acuity mother/baby unit whose mothers are taking chronic long-acting opioids are offered early pharmacologic treatment, breastfeeding support (unless contraindicated), and extended maternal stay for the duration of the birth hospitalization. All neonates are managed by a pediatrician and receive low-stimulation supportive care. Within 24 hours of birth, infants exposed to maternal methadone doses of 60 mg or higher are started on 0.1 mg/kg/dose of methadone every 6 hours; those exposed to less methadone or to buprenorphine are started on 0.05 mg/kg/dose every 6 hours. Urine and meconium drug screening and prescription monitoring database queries are performed routinely. Continuous monitoring for apnea and bradycardia is provided in the mother's room, and modified Finnegan scoring is performed every 4 hours by trained mother/baby nursing staff. A social work evaluation is completed for all families. Any feeding supplementation, whether by maternal choice or physician order, is initiated with expressed breast milk or standard 20 kcal/oz. formula.
Once an infant meets criteria for discharge, a weaning calendar is developed by a pediatric pharmacist, and methadone is dispensed in pre-filled oral syringes from the hospital outpatient pharmacy at an average out-of-pocket cost to the family of $13 per 1-month supply. Medicaid does not cover the cost of the infant's prescription in South Carolina. Caregivers are required to fill the prescription prior to discharge, and unit staff reconcile that all necessary syringes have been dispensed and that caregivers understand how to administer medication per program instructions.
During the outpatient weaning period, dosage reductions of approximately 15% (of the discharge dose) occur every Sunday and Wednesday for approximately 4 weeks. Office visits occur weekly at an outpatient pediatric medical home during weaning to evaluate the effect of medication reduction. Outpatient physicians assess for signs or symptoms of poor NAS control and have the option to slow the weaning process if necessary. During the outpatient methadone wean, each infant generates an additional $655 in outpatient charges beyond a normal infant. Hospital inpatient social workers collaborate with social workers in the pediatric medical home to ensure that transportation needs are met and follow-up is ensured for weaning visits. Outpatient social workers closely track visit compliance and address cases of concern. One or 2 postpartum newborn home visits are routinely provided by South Carolina Department of Health and Environmental Control for all families with Medicaid through a local health department. Families with a weaning infant receive targeted education and evaluation during these encounters. No new costs are generated by utilizing the home visiting program. Once completely off medication, infants are followed according to the recommended Early and Periodic Screening, Diagnostic, and Treatment schedule. All newborns are referred for formal developmental assessment at 3–4 months of age as well as to phone-based parenting support and developmental screening services (Help Me Grow®) that are available until the child reaches age 8.
Initial evidence for the MAiN treatment program reveals that it is safe, effective, and results in substantial cost savings compared to national expenditures for NAS infants. 15 A retrospective study was conducted to evaluate the MAiN program. From 2006–2014, 143 patients were enrolled in MAiN at GMH. Because of medical illness or complication, 26 patients (18%) were transferred to the NICU after enrollment, and 117 patients (82%) completed the inpatient component of the MAiN treatment program. Infants in the MAiN program from 2006–2014 experienced a median peak weight loss of 7% (range: 1% −14%) and median peak modified Finnegan score of 10 (range: 3–21). The overall breastfeeding rate among the cohort was 42%. Five newborns (4%) experienced oversedation. There were no medication errors, seizures, or deaths. Outpatient records were available for 115 patients. Of these, 14% visited an emergency department within 30 days of discharge; 7% were readmitted, none with a primary diagnosis of withdrawal. This may represent a significant improvement over standard treatment for NAS, during which infants often are treated in a NICU environment. In addition to improved patient outcomes, widespread implementation of the MAiN program may result in significant savings in hospital charges.
Data
Data collection for infants treated with MAiN at GMH was performed through data extraction from electronic medical records and direct chart review. All data were abstracted by a trained research assistant. Additional data on South Carolina NAS infants were acquired from all-payer inpatient hospitalization and emergency department encounter data, linking with state birth certificate and Medicaid claims data. This study population included all infants born in South Carolina hospitals between 2006 and 2014. NAS infants were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes of 779.5 and/or 760.72. The ICD-9-CM code 779.5 describes “drug withdrawal syndrome in newborn,” and the ICD-9-CM code 760.72 identifies “narcotics affecting fetus or newborn via placenta or breast milk.” Statistical analyses were performed using Stata 14 (StataCorp LP, College Station, TX, US).
Economic impact analysis description
A multistep approach was utilized to develop a cost analysis of the potential state and national saved charges that might result from widespread implementation of the MAiN treatment model. Researchers first identified the number of NAS cases in South Carolina for each year from 2006–2014 and the number of total births for the state over the same period. These data were then used to develop an annual NAS case rate per 1000 births. A linear regression model with case rate as the dependent variable and year as the independent variable was generated to predict the NAS case rate per 1000 births for South Carolina from 2015–2025. The NAS case rate per 1000 births for the years 2015–2025 was multiplied by the projected number of births per year in each of those years to obtain the projected number of NAS cases per year. State projected births for 2015–2025 were acquired from the South Carolina Revenue and Fiscal Affairs Office - Health and Demographics Section.
From 2006–2014, 25% of NAS infants at GMH were treated by the MAiN model. The researchers maintain this assumption that 25% of NAS infants will meet eligibility criteria for the MAiN model to obtain the projected number of MAiN-eligible infants for South Carolina. Recent Tennessee data confirmed that more than 50% of NAS cases were from supervised maternal opioid treatment therapy. 25 The present study's 25% estimate is conservative, given the data from Tennessee.
Using retrospective charge data for the MAiN program and the state, additional linear regression models were generated to predict NAS-related charges from 2015–2025. Several model estimations were tested for best fit and significance. After exploring these other model options, linear regression proved to be the best model fit across the scenarios. Data met the assumptions for linear regression. A time series model was not appropriate because of data limitations. Length of stay (LOS) was determined to be the key predictor of NAS charges. The final model included annual mean LOS as the independent variable and annual mean hospital charges as the dependent variable.
Scenario narratives
Three scenarios were developed to estimate the potential fiscal impact of widespread implementation of the MAiN program based on assumptions related to LOS as well as state and national MAiN and Medicaid eligibility.
Scenario 1 assumes that all future charges are based on the same average LOS demonstrated over the time period 2006–2014. It further assumes that 25% of NAS cases will be eligible for the MAiN program and that 80% of infants are covered by Medicaid, which is comparable with national literature. 2,3
Scenario 2 takes into account variability in LOS because of the strong relationship between LOS and total charges. LOS for state NAS cases showed a mean annual increase from 2006–2014 of 4.94% and was highly variable from year to year, with a total inflation-adjusted change over the time period of 13%. The mean annual change in LOS for the MAiN program was 1%, which was relatively stable over the time period. Given the variability in state LOS and the short time series, the researchers assume a conservative 2% annual increase in LOS for the state and a 1% increase in LOS for the MAiN program. The predicted mean LOS over the 11-year period 2015–2025 is used to estimate future charges for statewide cases and for those managed with the MAiN program. This assumption presumes the current per diem reimbursement model for Medicaid infants. If South Carolina were to shift to a DRG reimbursement model, LOS would not be relevant for this analysis. This model retains the assumption that 25% of NAS infants are MAiN eligible and 80% of infants are consistently funded by Medicaid.
Scenario 3 proposes that the MAiN program is implemented on a national scale. Assuming current national growth trends in NAS rates, a linear regression model was used to estimate future NAS rates per 1000 births. Using national projections of US birth rates and estimated NAS rates, future NAS births were projected. 24 An equation to predict national NAS charges was developed with LOS as the independent variable. This analysis retains the assumption that 25% of NAS infants are MAiN eligible and 80% of infants are consistently funded by Medicaid. With these metrics in place, the researchers assess the potential savings in hospital charges if the MAiN program were implemented on a national scale. These estimates do not account for approximate Medicaid reimbursement rates and as such must be considered an upper bound of potential savings.
Results
Patient data were collected on 117 infants receiving the MAiN treatment model at GMH from 2006–2014. Figure 1 illustrates the mean hospital charges per NAS case for infants treated with the MAiN program as well as mean hospital charges for all NAS cases in the state and nation. All charges were adjusted to 2014 USD (US dollars). Using analysis of variance to test difference in means, results reveal a statistically significant difference in charges between the MAiN population and the state and national populations (P < 0.0001). From 2006–2014, average charges for NAS infants in the MAiN program at GMH were $10,946.96 (2014 USD) compared to an average of $44,544.17 (2014 USD) for NAS infants statewide and $59,641.35 (2014 USD) for NAS infants nationwide.
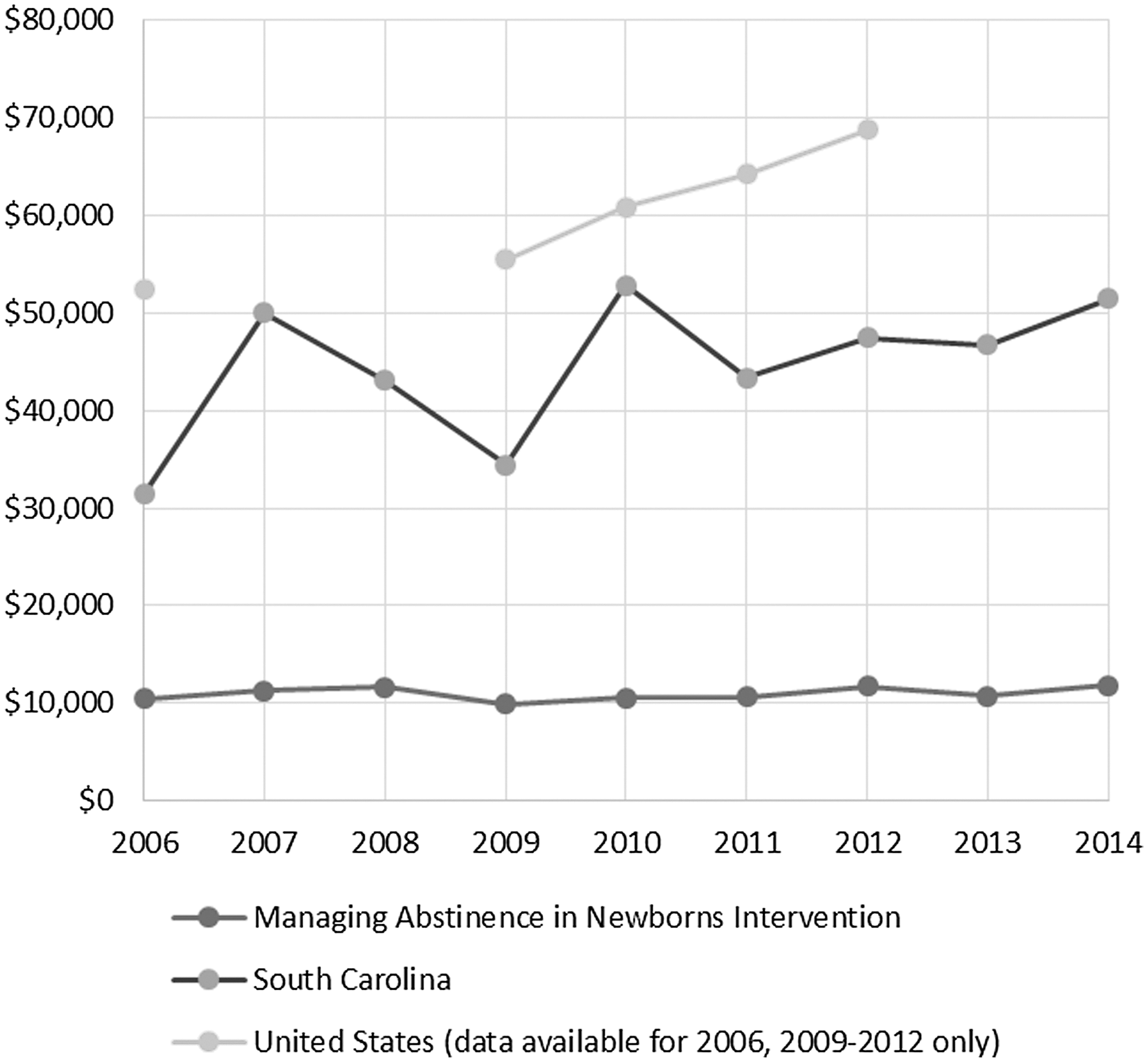
Average inpatient charges for NAS infants, 2006–2014. NAS, neonatal abstinence syndrome.
From 2006–2014, mean hospital charges for NAS infants treated in the MAiN program were relatively stable, with a mean annual change of 1.9% per year. Mean annual state charges for NAS diagnosed infants increased approximately 7.24% per year. From 2006 to 2014, total inflation-adjusted charges increased 12.17% for NAS infants treated with MAiN and 63.7% for NAS infants statewide. From 2000–2012, the total inflation-adjusted change in NAS-related charges nationally was 26.97% with an annual average increase of 4.5% over the 13-year study period.
County and state NAS birth projections
A linear regression model was used to test for model significance and prediction of future NAS cases in South Carolina. The dependent variable was NAS rate per year (2006–2014), and the independent variable was year. The model has an R2 of 0.93, with 93% of model variation predicted by this model. Table 1 contains the projected number of NAS births and MAiN treated infants in South Carolina in 2015, 2020, and 2025.
Prediction equation: y = 0.7299x−1462.4.
MAiN, Managing Abstinence in Newborns; NAS, neonatal abstinence syndrome.
These results confirm the potential for a substantial increase in the number of NAS diagnosed infants from 2015 through 2025. For South Carolina, the researchers predict a 6% increase in total births and a 99% increase in NAS cases if current trends hold. If the MAiN program continues to apply to approximately 25% of NAS diagnosed infants, substantially more state infants could be treated with this intervention.
County, state and national NAS charges projections
The following models were estimated to predict annual mean hospital charges for the MAiN program and the state. These prediction models use a fixed annual mean LOS, calculated as the mean of the annual average LOS over the time period.
Using predictions of NAS births and estimated charges, the following 3 scenarios explore potential saved hospital charges for state Medicaid programs and state and national taxpayers that support these safety net programs.
Scenario 1
Table 2 presents results of the 3 scenarios. Scenario 1 uses equations (1) and (2) and assumes a fixed annual mean LOS of 8.27 days for MAiN and 12.85 for the state (ie, the same average LOS from 2006–2014). The results of this scenario show that over the 11-year time period 2015–2025, the saved charges are estimated to exceed $56,000,000.
MAiN, Managing Abstinence in Newborns.
Scenario 2
Scenario 2 uses equations (1) and (2) and assumes a mean annual LOS of 9.32 days for MAiN and 14.67 days for the state based on the 1% and 2% projected annual increase in LOS, respectively. Based on these equations, predicted charges for MAiN are $11,802.82 per case, and predicted charges for the state are $57,072.92 per case.
Scenario 2 results reveal average state charges for these 11 years of $89,607,241 with no intervention (Table 2). From 2015–2025, a statewide MAiN program expansion could reduce charges to state Medicaid by more than $71,000,000.
Scenario 3
Scenario 3 estimates potential nationwide saved charges if the MAiN program were to be implemented on a national scale. The average NAS rate per 1000 births from 2000–2012 was 3.39 births per 1000. Using the following linear regression model (3) to estimate the future NAS case rate for the United States and applying that rate to the number of births projected by the US Census,
17,24
the number of future neonates with NAS is estimated to be 25,746 in 2015, 34,727 in 2020, and 43,474 in 2025.
Over the 11-year period from 2015–2025, 381,358 infants could be diagnosed with NAS. By 2025, applying the 25% treatment eligibility assumption, almost 11,000 infants per year across the United States could be eligible for the MAiN treatment program, with an approximate total of 95,000 infants eligible for MAiN across the US from 2015–2025.
National data reveal an average LOS of 16.3 days from 2000–2012, with average national charges of $59,641.35 per NAS case (2014 USD). The regression model used to predict national charges (adjusted to 2014 USD) is given by (4):
Using current treatment protocols and assuming a fixed 16.3-day LOS, total charges are estimated to be more than $4.5 billion for approximately 76,000 infants treated across the nation from 2015–2025.
Equation (1) was used to estimate national charges if MAiN were expanded across the United States. Assumptions included that 25% of NAS infants would be eligible for MAiN, 80% of MAiN-eligible infants would be covered by Medicaid, and the LOS would be fixed at 8.27 days. Results show that if MAiN were expanded, the average savings is projected to be more than $337 million annually in Medicaid charges, with a total potential reduction in Medicaid charges of approximately $3.7 billion from 2015–2025.
Discussion
Currently, a national standard treatment protocol for NAS infants does not exist in the United States. Although some innovative treatments are described in the literature, 16 –21 NAS-diagnosed infants are largely treated in NICUs across the country. As health care systems transition away from fee for service to population-based reimbursement for care, there is incentive for hospitals to consider lower cost, effective treatment models. In this case, hospitals that have implemented low-cost solutions for NAS care will save money as well. Thus, from a clinical perspective, there is impetus to explore innovative treatments, and as these treatments are proven safe and efficacious, understanding the cost-effectiveness of these models is critical.
This analysis illustrates that there are strong cost incentives related to implementing the MAiN program across the state and nation. Each of the described scenarios makes conservative assumptions about current trends that may or may not occur; however, if current trends continue with little change to the current NAS treatment protocol, the cost burden to Medicaid and hospitals will increase and may increase substantially. Further, LOS assumptions inherent in this analysis would be of little importance if the state, and others, shift to a DRG reimbursement model for pediatric care.
It is important to note that this analysis does not take into account the costs of implementing a new treatment model; however, based on information from the reference hospital, these costs are not necessarily substantive and in many cases would not require hiring additional staff. Much of the implementation requires training existing staff to regularly, appropriately monitor NAS infants, providing consultation and education for families, establishing partnerships with supportive community resources, and potentially hiring a case manager depending on the caseload of NAS infants.
Additional limitations of this study include that the MAiN model is a program for NAS infants at high risk for withdrawal related to long-acting opioid exposure, whereas the state and national cohorts are composed of all NAS infants. Infants coded for NAS in these cohorts may have been affected by a variety of medications or illicit drugs used by a mother as prescribed or illegally. Others may have been coded for NAS because of withdrawal from medications administered to the neonate during prolonged critical illness. Recent research from the state of Tennessee provides evidence that more than half of all 2015 NAS cases were associated with supervised opioid replacement therapy. 25 The initial study population led to the conservative assumption that 25% of NAS infants in the state and national cohorts would be eligible for MAiN; however, recent research may indicate MAiN may have wider application.
The analyses in this study were limited to using hospital charges to estimate saved charges to Medicaid, because state and national cost data were not available. Charges do not account for Medicaid reimbursement rates, which in South Carolina range from 40% to 50% for NAS infants depending on whether infants receive treatment in a NICU or non-NICU setting. As such, these estimated saved charges should be considered as a first step in examining the potential economic magnitude of an innovative treatment model such as MAiN.
The challenge of NAS continues to be discussed and evaluated on a national scale. Although opportunities for more effective treatment should be considered across the nation, there are outpatient methadone policy differences from state to state and even within states that may prove to be barriers to replication of innovative treatments. 26 –28 Although states are obligated to meet national regulatory standards, states and localities may exceed federal minimum standards. For example, some states do not allow patients to be discharged on drugs such as morphine or methadone, an important component of the MAiN intervention. Other dosing requirements vary across states, and some states may automatically withdraw a pregnant patient from methadone treatment. All of these variations in policy make a standard national treatment protocol difficult to implement in the near term. 26,28
As NAS research continues, a more robust time series of data is an important area for future research consideration. The MAiN program treated 117 infants from 2006–2014, and small sample sizes in some years could have impacted overall model results. Further, as researchers continue to examine this issue, better understanding of the socioeconomic patterns of mothers and NAS infants, the geographic distribution (eg, urban vs. rural) of NAS, along with policy impacts across states are all important areas of future research.
Footnotes
Author Disclosure Statement
Drs. Dickes, Summey, Mayo, Hudson, Sherrill, and Chen declare no conflict of interest with respect to the research, authorship, and/or publication of this article. The authors received the following financial support: All phases of this study were supported by the South Carolina Department of Health and Human Services. Dr. Hudson also is supported by the Greenville Health System Children's Hospital.