
Abstract
Innovations in chronic disease management are growing rapidly as advancements in technology broaden the scope of tools. Older adults are less likely to be willing or able to use patient portals or smartphone apps for health-related tasks. The authors conducted a cross-sectional survey of older adults (ages ≥50) with hypertension or diabetes to examine relationships between portal usage, interest in health-tracking tools, and eHealth literacy, and to solicit practical solutions to encourage technology adoption. Among 247 patients surveyed in a large integrated delivery health system between August 2015 and January 2016, eHealth literacy was positively associated with portal usage (OR [95% CI]: 1.3 [1.2–1.5]) and interest in health-tracking tools (1.2 [1.1–1.3]). Portal users compared to nonusers (N = 137 vs.110) had higher rates of interest in using websites/smartphone apps to track blood pressure (55% vs. 36%), weight (53% vs. 35%), exercise (53% vs. 32%), or medication (46% vs 33%, all P < 0.05). Portal users noted cumbersome processes for accessing portals and variations in provider availability for online scheduling and response times to messages. Portal nonusers expressed concerns about data security, lack of personalization, and limited perceived value of using portals. Both groups noted the importance of computer literacy and technical support. Patient stakeholders recommended marketing initiatives that capture patient stories demonstrating real-life applications of what patients can do with digital technology, how to use it, and why it may be useful. Health systems also must screen for eHealth literacy, provide training, promote proxy users, and institute quality assurance that ensures patients' experiences will not vary across the system.
Introduction
T
However, recent studies suggest that older adults are less likely to use, and therefore less likely to benefit from, expansions in digital technology to manage health. Per the Pew Research Center's Internet & American Life Project, the rate of accessing the Internet increased from 52% to 84% among all US adults between 2000–2015. 2 Rates among adults ages 50–64 years increased 46% to 81% while rates among adults ages 65 years and older increased from 14% to 58%. In a 2012 national survey, only 59% of US adults looked online for health information within the past year, with younger adults being more likely than older adults to have reported doing so (ages 18–29 years [72%] vs. 30–49 years [67%] vs. 50–64 years [54%] vs. ≥65 years [30%]). 3
An analysis of 10 years of data from the Health Information National Trends Survey (HINTS) confirmed increasing rates of Internet use among US adults and further highlighted that age, sex, race/ethnicity, and education predict differences in access to the Internet and online health activities. 4 The 10-year trend in HINTS data also suggests that although the overall differences attributed to sex and race/ethnicity have declined, age and education remain important predictors. 5 For example, Gordon and Hornbrook demonstrated within a large health plan that, compared to adults ages 65–69 years, adults ages 70 years and older are less likely to register to use patient portals or to use key features such as secure messaging even when registered. 6 In addition, adults ages 75 years and older are less likely to own digital devices, use the Internet, or to be able or willing to use digital technology to perform health-related tasks.
Differences in computer self-efficacy likely distinguish users of online health information from nonusers. 7 Choi and Dinitto demonstrated that eHealth (electronic health) literacy, defined as “the ability to seek, find, understand and appraise health information from electronic sources and apply the knowledge gained to addressing or solving problems,” 8 is negatively associated with age and positively associated with Internet use. 9 Even if older adult Internet users are receptive to patient portals, the supportive needs and approaches to engaging older adults in patient portal use may differ from those used to engage younger adults. 10 Awareness of “digital disengagement” among older adults is imperative. 11
Health system promotion of patient portals and eHealth technology for delivery of care can potentially widen the digital divide for patients who are least likely to use it. Prior studies have shown that patient choice to use portals is influenced by attitudes/preferences for using technology, perceived usability, provider endorsement, care received prior to accessing patient portals, demand for different types of health services, patient preferences for how to access services, and multiple demographic factors (age, race, ethnicity, degree of comorbidity, education level, health literacy). 12 –14 Age, socioeconomic factors and trust in health care professional information also influence willingness to use mobile devices to exchange health information electronically. 15 Health systems are challenged with finding effective solutions for surmounting these barriers.
The study team formally engaged patient stakeholders in generating solutions for reducing the digital divide and disengagement among older patients with chronic conditions. In 2015, Ochsner Health System, Louisiana's largest integrated delivery health system, launched chronic disease management programs for hypertension and diabetes that incorporate disease registries, bulk orders for care gaps, nurse care coordination, and patient portal outreach communication (eg, reminders). Simultaneously, a portal-based hypertension digital medicine program for remote monitoring of blood pressure was piloted. 16
Given these emerging strategies, Ochsner's Center for Applied Health Services Research conducted this study to better understand how to engage older adult patients with hypertension and/or diabetes in using portal technology for self-care. This study examined the relationship between eHealth literacy, portal use status, and interest in using websites or smartphone applications for tracking health information, and engaged older adult patients with hypertension and/or diabetes in identifying specific facilitators and barriers to using the portal. Finally, this study provided system administrators with patient-generated recommendations for tailoring portal implementation to encourage use among older adults served in the community.
Methods
Study setting and population
This study was conducted at Ochsner Health System, southeast Louisiana's largest nonprofit, academic, multispecialty health care delivery system. Ochsner owns, manages, or is affiliated with 30 hospitals and 60 health centers, and employs more than 1000 physicians in 90 specialties. Ochsner serves approximately 600,000 unique patients annually. In 2012, Ochsner implemented Epic Systems (Epic Systems Corporation, Verona, WI), which includes the MyChart patient portal. To date, approximately 333,000 patients have activated their MyOchsner patient portal accounts.
Study design
The study team conducted a cross-sectional survey of adults ages 50 years and older who saw their primary care provider at least twice between July 2012 and December 2014 within Ochsner Health System. Baby boomers were included in the study because this population is predicted to rapidly increase the size of the elderly population. Given Ochsner's initial focus on population health management strategies for patients with hypertension or diabetes, 101,019 primary care patients who had at least 1 of these chronic conditions were sampled. Details of the sampling design will be described. Subsequently, a survey was conducted to compare Internet use among portal users and nonusers, self-efficacy in using the Internet, interest in tracking health using website/smartphone applications, experience with using or perceived usefulness of patient portal features, and recommendations to encourage patient use of the portal. Survey data were collected and managed using REDCap electronic data capture tools hosted by the Ochsner Clinic Foundation. 17 This study was approved by the Ochsner Health System Institutional Review Board.
Survey
Questionnaire
To gauge Internet use, the study team assessed use in the prior 3 months (1 item) and incorporated the 10-item eHealth Literacy Scale (e-HEALS). 18 Findings from a study of older adults demonstrated that eHEALS has internal consistency (α = .94), test-retest reliability, and construct validity. 19 Refer to Table 1 for content of e-HEALS items. To gauge interest in tracking health using website/smartphone apps, the team included adaptations of 2 items from the national Consumers and Health Information Technology Survey. 20 Also included was an item that listed the following health-related activities patients can track using websites/smartphone apps: accessing online health information; tracking exercise/fitness/pedometer readings; or recording heart rate, diet/food/calorie count, weight, blood pressure, blood sugar, medication alerts, mood (stress levels), and hours of sleep.
P < 0.05.
e-HEALS, eHealth Literacy Scale; SILS, Single Item Literacy Scale.
The survey assessed whether patients had ever used MyOchsner and, if so, whether they had used it in the past 12 months. Patients who indicated use of MyOchsner were then asked questions from the Clinician and Group-Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) HIT scale to assess their experiences. 21 The CG-CAHPS HIT items have a scale reliability of 0.7. 22 Two items assessed experiences with making an appointment (Did you use [MyOchsner] to make an appointment for this provider's office? How often did you get an appointment as soon as you needed?). Three items assessed experiences with sending a medical question (Did you send a medical question through [MyOchsner] to this provider's office? How often did you get an answer to your medical question as soon as you needed? How often were all of the questions answered?). Four items assessed experiences with looking at lab/test results (Does this provider office put your laboratory or other test results on [MyOchsner] for you to see? Did you look for your lab or other test results on [MyOchsner]? How often was it easy to find these lab or other test results on [MyOchsner]? How often were these lab or other test results put on [MyOchner] as soon as you needed them?) Patients who indicated nonuse of MyOchsner were administered questions about access to technology needed to use MyOchsner (Internet, computer, cell phone, e-mail) and reasons for not using MyOchsner (privacy concerns, preference for using computers or communicating by phone, necessity of MyOchsner for managing health, perception of time consumption).
Both MyOchsner users and nonusers were asked about perceived usefulness of patient portal features using 1 item adapted from the national Consumers and Health Information Technology Survey. 20 MyOchsner users were asked to provide feedback on how to improve the patient experience. Nonusers were asked how likely they were to use MyOchsner in the future and to provide feedback on what the health system could do to encourage patient portal use.
The survey concluded with the Single Item Literacy Scale (SILS) 23 and items to assess demographics (age, sex, race/ethnicity, education, chronic conditions, self-rated health, and insurance). The SILS is a 1-item question that asks, “How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?” Responses range from 1 (never) to 5 (always). Scores greater than 2 indicate some difficulty with reading printed health-related material (sensitivity 54%; specificity 83%; receiver operating curve 0.73). 23
Sampling design and survey administration
Stratified random sampling was used to generate a list of patients randomized to phone or e-mail surveys. The study hypothesis was that eHealth literacy would be associated with self-identified portal use status. The study team estimated a sample size of 164 respondents to detect a 20% difference between portal users and nonusers in agreeing with knowing what health resources are available on the Internet and confidence in using the Internet to make health decisions (e-HEALS items #3 and #10). The team generated a list of patients (N = 1541) whose phone numbers or e-mail addresses were verified as functional (eg, not entered as “place holders” in required fields). Randomization categories for recruitment included activated portal account via phone (n = 391) or e-mail (n = 390), and nonactivated account via phone (n = 400) or e-mail (n = 360).
Portal account activation status was the easiest method to preliminarily identify users and nonusers. The study team recognizes that account activation does not equate with actual use. Randomized patients were similar to the aforementioned 101,019 primary care patients with hypertension and diabetes with regard to sex, race, and portal activation status but were slightly younger (mean age, [SD]: 62 [7.5] years vs 66 [10.5] years, P < 0.05).
Waves of survey invitations were sent to reach the target sample size. Both survey modes offered alternative survey formats if desired. Patients were informed that participation was voluntary and would not impact their care at Ochsner if they declined, and that the results of this research would be shared with Ochsner leadership overseeing implementation of HIT to inform efforts to improve their experience. Each e-mail survey invitation contained a unique hyperlink to the survey to facilitate patient self-entry of responses, which were then stored directly in the research database. Trained telephone interviewers entered patient responses directly into REDCap. A total of 3 invitations were sent to nonresponders via e-mail or phone. The survey was administered from August 2015 to January 2016.
Patient engagement in survey design
The research team worked closely with the Ochsner Patient Research Advisory Board (O-PRAB) on the design of the survey. All O-PRAB members reflect the target age group of the survey and represented both MyOchsner users and nonusers. The original draft of the survey was piloted by e-mail and phone with the O-PRAB to determine the length of time required to complete the survey and to assess the relevance/necessity of the items included. The survey was subsequently shortened and took an average of 12 minutes to administer.
Data analysis
To calculate the response rate for each of the 4 categories of survey invitations, the study team eliminated patients with nonworking or incorrect contact information (eg, bounced e-mails, business phone number, fax numbers, nursing home numbers, wrong person) (n = 39); patients who were ineligible or who had unknown eligibility (deceased, mental or physical impairment, no longer an Ochsner patient, never answered, n = 141); and those randomized patients whom the team never attempted to call (n = 144). The team then defined study groups based on patient self-identification as a MyOchsner user or nonuser (never used it). Self-identification was chosen because account activation does not equate to usage.
Baseline characteristics of portal users were compared to nonusers using Student t test for continuous variables and chi-square analysis for categorical variables. The main study outcomes were total e-HEALS scores (range 8 to 40; higher score indicates greater perceived eHealth literacy), self-identified use of MyOchsner (yes/no), and interest in websites or smartphone applications for tracking one's health (yes/no). The multivariate analyses examined the strength and direction of the relationship between patient characteristics and these outcomes. Covariates of interest included: self-reported age, sex, race (black vs white), number of chronic conditions, education (less than high school vs high school or greater), and general health literacy (SILS–inadequate health literacy; yes/no).
The study team examined patient comments regarding how to improve MyOchsner and strategies to encourage use of the portal. The team used the Technology Acceptance Model and the Unified Theory of Acceptance and Use of Technology Model as frameworks for developing a thematic coding scheme. 24 Key concept domains within these models include: behavioral intention (motivation or willingness), attitude (evaluative judgment of technology use), perceived ease of use, perceived usefulness, social influence, and perceived behavioral control (self-efficacy, facilitating conditions, controllability).
Two members of the research team (EPH, JHB) each independently coded patient comments using these concept domains and then met to reach consensus regarding differences of opinion about specific comments. The agreement rate between the 2 coders was 95%. The researchers shared study results with the O-PRAB to solicit meaningful interpretation of facilitators and barriers to using MyOchsner and recommendations to health system administrators to encourage patient use of and improve patient experience with the portal.
Results
Patient characteristics
Refer to Figure 1 for details on survey recruitment. Response rates varied by the survey recruitment category (activated portal account: 43% phone, 15% e-mail; nonactivated account: 33% phone, 7% e-mail). Survey respondents were slightly older than nonresponders (mean age [SD]: 63.7 [7.2] vs. 62.1 [8.0], P < 0.01); however, there were no significant differences by sex (female vs. male: 62.5% vs. 55.8%) or race (white, non-Hispanic vs. black non-Hispanic: 77.8% vs 71.8%; all P < 0.05).
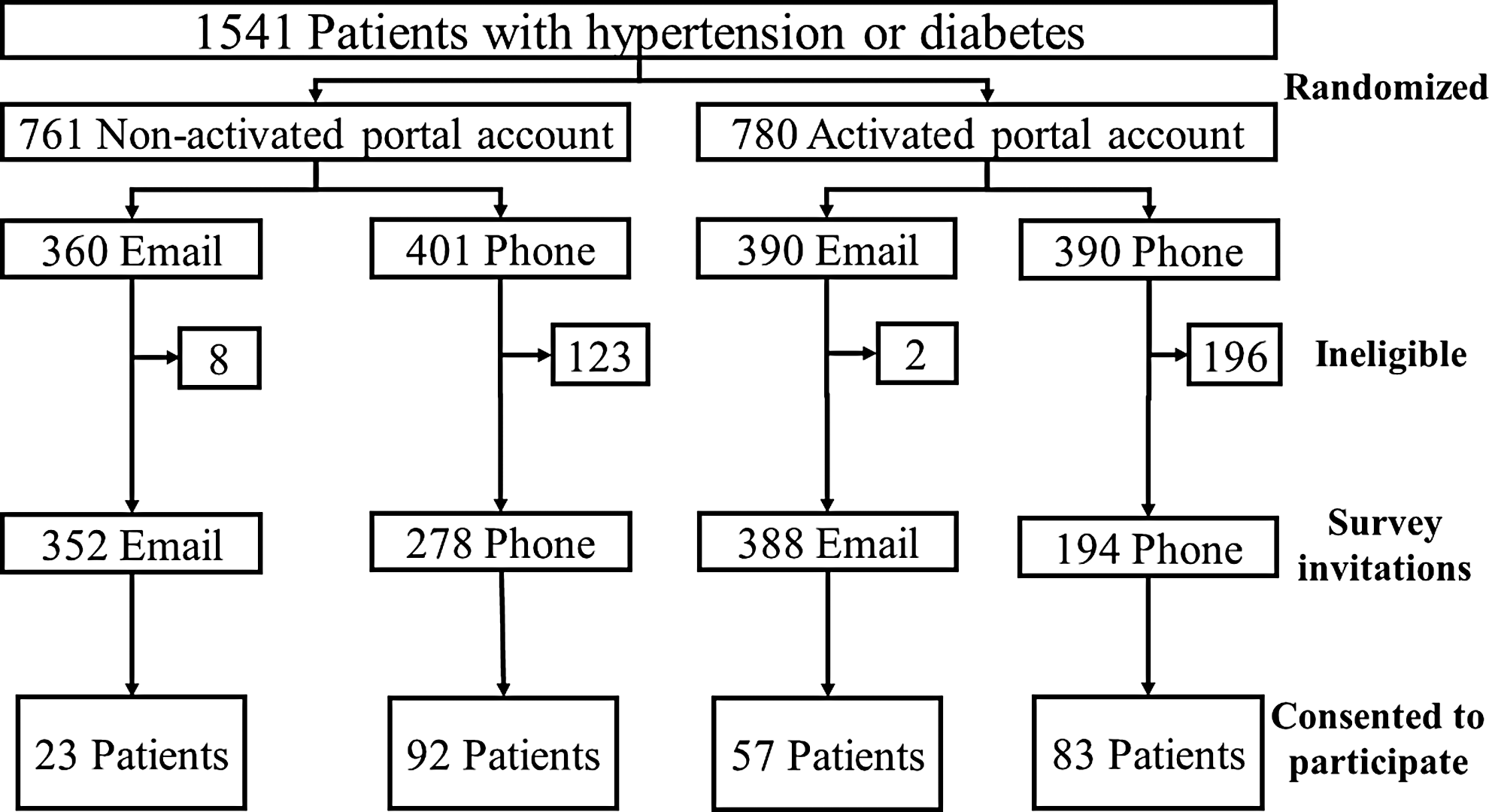
Survey sampling strategy.
The analysis was limited to 247 patients who completed the survey. Approximately 20% of respondents whose accounts were listed as activated reported that they had never used the patient portal. Compared to nonusers, self-identified portal users had higher levels of education, lower rates of inadequate health literacy, higher rates of using the Internet and having an interest in websites or smartphone apps for tracking health, and higher total e-HEALS scores (Table 1). Portal users had higher rates of agreeing with e-HEALS survey items reflecting level of confidence in their ability to navigate and use the Internet for health information. Despite high rates of having access to computers, cell phones, and Internet connection (>70%), portal nonusers most frequently cited preference for phone communication as the most common reason for not using the portal (75%).
Perceptions of usefulness of portal features
Compared to portal nonusers, a significantly higher proportion of users rated viewing lab results (user vs. nonuser: 94% vs. 60%), checking health records for accuracy (79% vs. 65%), and receiving test reminders (78% vs. 64%; all P < 0.05) as useful (data not shown in tables). Although a higher proportion of portal users also rated looking at doctors notes (73% vs. 62%), sending medical questions to the doctor's office (67% vs. 60%), making an appointment online (51% vs. 46%), and renewing medication prescriptions (55% vs 53%) as useful, these differences were not significant. Fewer respondents rated viewing or paying bills online (44% vs. 49%) or sharing medical information with family or friends as useful features (32% vs. 33%).
Interest in websites or smartphone tools for tracking health
Compared to nonusers (data not shown in tables), portal users had a significantly higher rate of reporting interest in using websites or smartphone applications to access health information (68% vs. 40%), record blood pressure (55% vs. 36%), track their weight (53% vs. 35%), record exercise (53% vs. 32%), track medication (46% vs 33%), or monitor heart rate (44% vs 30%). Less than a third of all respondents were interested in tracking their blood sugar, sleep, or mood using websites or smartphone applications.
Associations between eHealth literacy, portal use, and interest in applications for tracking health
In the multivariate analysis (Table 2), e-HEALS scores were positively associated with higher education and negatively associated with age. The odds of portal usage increased with total e-HEALS score and decreased among black patients. The odds of being interested in using websites/smartphone apps increased with total e-HEALS score. All other covariates of interest were not significantly associated with eHealth literacy, portal use, and interest in applications for tracking health in the study population.
P < 0.05.
CI, confidence interval; e-HEALS, eHealth Literacy Scale; HS, high school; OR, odds ratio; SE, standard error; SILS, Single Item Literacy Scale.
Portal nonuser recommendations for encouraging use
Among portal nonusers who shared feedback for encouraging use (n = 87), most comments reflected patient willingness or motivation to use portal technology (32%) and highlighted personal- and system-level factors that impede or facilitate using the portal (36%). Portal nonusers mostly expressed concerns about online security of their information, lack of personalization in using technology, lack of resources, desire for skills or technical support to navigate computers and/or the Internet, and simply not seeing the need for or value of using the portal to manage their health. Refer to Table 3 for examples of specific comments shared.
Portal user recommendations for improving the patient experience
Among portal users who shared feedback for improving the portal (n = 95), respondents suggested addressing perceived ease of use (33%), personal- and system-level factors that impede or facilitate using the portal (37%), patient attitudes about the portal (26%), and perceived usefulness of portal technology (19%). Most comments highlighted concerns about computer literacy, the cumbersome nature of logging into portal accounts (eg, remembering passwords, multiple accounts for patients in the same household), lack of technical support, and variations in provider availability for online appointment scheduling and response times to medical messages. Refer to Table 4 for examples of specific comments shared.
O-PRAB recommendations to system administrators
O-PRAB members reviewed study results, reflected on personal experiences with using or not using the portal, and offered several recommendations to system administrators to better address the feedback provided by survey respondents. The O-PRAB identified a lack of clear tangible incentives for using the portal for managing one's health as a supplement to the traditional provider-patient relationship to be a major area of concern for portal nonusers. O-PRAB members therefore suggested that advertisement about the portal (marketing posters and mailings) should not only highlight what patients can do in the portal but also emphasize how to use it and why patients might find select features useful. Messaging about the benefits of using the portal should focus on capturing stories from real patients and demonstrate real-life applications of using the portal. To address portal nonusers' self-efficacy in using technology, the board noted that someone other than the busy clinical team should be responsible for introducing patients to the portal and showing them how to use it (including navigating the Internet). Moreover, screening patients for computer literacy and comfort levels with using technology is imperative. Promotion of the proxy user might further alleviate patient concerns about self-efficacy in using the portal. Finally, the board recommended that the health system prioritize efforts to institute quality assurance processes to guarantee that patient portal users have consistent experiences (eg, message response times, availability of online appointment scheduling and lab results) that do not vary between providers or clinical settings.
Discussion
Compared to nonusers, portal users had higher levels of education, higher rates of using the Internet and having an interest in websites or smartphone apps for tracking health, and higher total e-HEALS scores. The e-HEALS scores were associated with age, education level, portal usage, and interest in using websites/smartphone apps to track health. Using a theoretical model of accepting technology, this study observed insightful similarities and differences among portal users and nonusers in the relative importance of addressing patient attitudes about the portal, self-efficacy to use the portal, patient- and system-level factors that impede or facilitate using the portal, perceived ease of use, and perceived usefulness of portal technology. Although many of these findings confirm previous studies, to the study team's knowledge, this is the first study to formally involve patients in identifying practical solutions for surmounting challenges to HIT adoption and engagement among older adults.
This study highlights the salience of incorporating eHealth literacy interventions into the design and implementation of portal and e-Health/m-Health (mobile health) technology. eHealth literacy entails a complex interplay of 6 core competencies, including 8 : traditional literacy (ability to read written text), health literacy (skills required to interact with a health system), information literacy (knowing what resources to use to find information on a specific topic), scientific literacy (understanding how science is done), media literacy (ability to critically appraise media content and place information within a sociopolitical context), and computer literacy (ability to use computers). All skill sets are required to engage electronic health resources effectively.
Screening for eHealth literacy provides a way to detect knowledge and skills deficits that patients otherwise may not readily reveal. Tieu et al. illustrated how patients with limited health literacy experience a number of computer barriers (eg, how to use a search bar, website navigation), take longer to complete tasks, and have problems interpreting medical results. 25 Wolff et al demonstrated that although patients' caregivers are more likely to have adequate health literacy and perform health management activities through online portals, shared access via patient portal proxy users is an underutilized strategy. 26 The O-PRAB insightfully recommended that health systems not only screen for computer literacy and provide training in how to use portals but also heavily promote the value of having a proxy user to optimize use of technology.
Screening patients for eHealth literacy also could help identify patients who may hesitate to adopt other digital tools for chronic disease self-management. In this study, patients with lower perceived eHealth literacy were less likely to express interest in using websites or smartphone applications to track their health despite having access to computers, cell phones, and the Internet. Lack of motivation to use technology–no matter how well designed–will undoubtedly lead to low adoption rates.
Nonetheless, lack of interest also may be a proxy for patient perceptions of limited self-efficacy for using digital tools. Mackert et al demonstrated that general health literacy is associated with greater perceived ease of use and perceived usefulness of fitness/nutrition/activity trackers and patient portals. 27 Most older adults, regardless of whether they own a smartphone or tablet computer, report that they would need assistance using a new device or digital service. 28 Assessing mobile device proficiency and training older adults to use them is imperative. Older adults with multiple chronic conditions may experience difficulties not only because of unfamiliarity with technology but also because of cognitive or physical impairments that make using technology difficult. 28,29 Therefore, caregivers should be engaged in managing m-health technology as an alternative option. These considerations are especially important for reducing disparities in access to technology-based disease management programs from which older patients may benefit.
Health systems must attend to basic customer service issues that facilitate or hinder using online portals. Health systems have limited control over portal technology design, especially when implementing electronic medical record tethered portals. Nonetheless, real-time technical assistance provides a human touch that can alleviate frustrations portal users may experience with using the technology. An even more salient issue is the need to incorporate quality assurance with regard to appointment availability and response times to portal messages. Accessing services through different means for different providers can become too cumbersome. Variability in quality of these online services further discourages use.
The O-PRAB recognized the importance of transparency in addressing patient concerns about technology creating barriers to the provider-patient relationship. Previous literature supports the notion that patients prefer to maintain existing face-to-face communication and to use the portal to enhance the provider-patient relationship between visits. 30,31 Crafting patient-centered messaging that incorporates real patient stories demonstrating the utility of technology for enhancing the provider-patient relationship while supporting self-management may increase the value of using it among older adults who place greater value on interpersonal or social interactions.
This study has several limitations. It was conducted within a single institution; therefore, the findings have limited external generalizability to other health systems, electronic medical record vendors, or regions of the country. In addition, only patients with hypertension or diabetes were sampled, given the limited scope of programs within the study health system that currently utilize self-management digital technology. Therefore, conclusions cannot be drawn about portal engagement for other chronic diseases.
Given the response rates, the study findings are subject to survey response bias. The study team acknowledges that respondents may have been driven to participate either because of strong opinions about the patient portal or strong interest in contributing to the health system's quality improvement efforts in general. Even so, the survey response rates are similar to a number of national studies that included questions on similar topics (technology adoption). The HINTS study reported response rates ranging from 21% to 40%, depending on the mode of administration. 32 The Pew Research Center reported a decline in survey response rates from 39% in 1997 to 9% in 2012. 33 The Pew Research Center also reported no difference in the quality of survey responses obtained from their standard survey approach compared to a more intense approach that included an extended field period, monetary incentives, and deployment of their most successful interviewers. Notably, this study was powered to detect differences between self-identified portal users and nonusers based on the underlying hypothesis that eHealth literacy would explain differences between study groups. The target sample size of responders was exceeded.
Notwithstanding these limitations, the findings largely confirm previous literature examining facilitators and barriers to adoption of portal technology among older adult patients. As health systems increasingly promote the use of HIT, systematic screening of patients' use of and interest in health-related technology for medical care and chronic disease self-management is imperative. The e-HEALS may be a useful tool to identify patients who are most likely to adopt use of and benefit from engaging in self-care through patient portals, wearable devices, or smartphone applications for tracking their health. Screening for eHealth literacy also can identify patients who are least likely to adopt such technology and require additional support. Finally, active engagement of patients in reviewing their experiences with health self-management technology can generate practical solutions to improve interest, self-efficacy, and sustained use of technology.
The paucity of evidence-based strategies to effectively manage patients with limited eHealth literacy remains a formidable challenge for health systems. Future research must examine the comparative effectiveness of eHealth literacy interventions for older adults, the instructional content and delivery methods that work best to improve eHealth literacy, the effectiveness of these interventions in clinical versus community settings, and whether these interventions are associated with increased use of self-management technology and, ultimately, improvements in health outcomes.
Footnotes
Acknowledgments
The authors would like to thank the Ochsner Patient Research Advisory Board for their collaboration on this project; and Richard Milani, MD (Chief Clinical Transformation Officer) and Todd Burstain, MD (Chief Medical Information Officer) for their leadership roles in optimizing health information technology within the Ochsner Health System.
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.