
Abstract
Health and health care in the United States are being jeopardized by top-end spending whose share of the gross domestic product continues to increase even as aggregate health outcomes remain mediocre. This paper focuses on a new approach for improving stakeholder role performance in the marketplace, value-driven population health (VDPHSM). Devoted to maximizing the value of every dollar spent on population health, VDPH holds much promise for ameliorating this dilemma and exerting a constructive influence on the reshaping of the Affordable Care Act. This paper introduces VDPH and differentiates the science underlying it from the management that serves to make good on its potential. To highlight what VDPH brings to the table, comparisons are made with 3 like-minded approaches to health reform. Next, 2 areas are highlighted, workplace wellness and the quality and cost of health care, where without necessarily being recognized as such, VDPH has gained real traction among 2 groups: leading employers and, more recently, leading providers. Key findings with respect to workplace wellness are assessed in terms of psychometric performance to evaluate workplace wellness and to point out how VDPH can help direct future employer initiatives toward firmer scientific footing. Then, insights gleaned from the employer experience are applied to illustrate how VDPH can help guide future provider efforts to build on the model developed. This paper concludes with a framework for the use of VDPH by each of 5 stakeholder groups. The discussion centers on how VDPH transcends and differentiates these groups. Implications for health reform in the recently altered political landscape are explored.
Introduction
T
Tackling this dilemma
Former President Obama recently assessed progress in improving health outcomes while reducing health costs. 4 ACA-sponsored reforms have contributed to promising gains (eg, sharp declines in hospital-acquired infections 5 and readmission rates from 2010–2014 6 ), even as major insurers have withdrawn from government exchanges because of smaller market sizes and higher-than-expected risk profiles. 7
Yet, his assessment all but omitted key elements of the major progress achieved in the private sector that are likely to figure prominently as the Trump Administration endeavors to change course. Specifically, 2 major themes have led to an array of evidence-based marketplace innovations: (1) better value–improved outcomes at reduced costs–can be achieved in health care delivery and payment 8 and (2) needed improvements in population health (PH)–the distribution of health outcomes in a population and the health determinants that influence this distribution–can be achieved via policies and interventions targeting these determinants. 9
With value rooted in health economics and PH in public health, these 2 ideas have remained largely distinct in their development. Yet, better value is increasingly providing a compass for guiding PH management efforts toward sustainability. 10,11 Conversely, PH and new avenues for advancing it (eg, stakeholder collaboration) are being embraced as the larger context in which value improvement should be targeted. 12,13
It is thus not uncommon to hear of value as “baked into” PH (or vice versa). Yet, this reflects a merging of the 2 themes that to date has been at most informal and unsystematic. The time is now ripe to strive for a more explicit embrace of their integration. An explicit embrace could bring the underlying science and its management into more cohesive, mutually reinforcing alignment and spark innovation. The net effect could propel the considerable gains that value and PH have each made. In addition, such a fusion could help to sustain continuing health reform in the recently sharply altered political landscape. Appropriately configured, it could support prior progress under the ACA and serve to support the emerging priorities of other more marketplace-oriented approaches. 14
We seek to advance this integration by introducing value-driven population health (VDPHSM). VDPH as a science analyzes outcomes relative to investment to determine priorities among policies and programs. These priorities seek to differentiate the greatest and broadest gains in PH and to improve outcome-to-cost ratios to maximize the value of every dollar spent on health, well-being, and functional status (performance/productivity). VDPH management operationalizes this science.
VDPH in context
Several premises guiding the evolution of VDPH both differentiate between and transcend stakeholder groups. First, how each stakeholder group performs its role impacts the system's outcome/cost dilemma. Measurable progress that each group makes in becoming better performers vis-à-vis VDPH's role criteria, in turn, helps to ameliorate this dilemma.
Second, the path toward better role performance for each stakeholder group lies in evidence-based management rooted in wise investments prioritized by the science of VDPH. The metrics being used to gather the evidence to inform and shape the management of this science can be appraised by guideposts reflecting validity and reliability. Progress vis-à-vis these guideposts speaks to predictions that flow from tenets for VDPH that afford the opportunity to advance its scientific underpinnings.
Third, VDPH transcends stakeholder groups with the value equation expressed in PH terms whose form–health outcomes achieved relative to costs incurred–is generalizable across groups but whose parameters vary by stakeholder group. The form of the PH-framed value equation thus functions as a crosswalk across stakeholder groups. This crosswalk means that the successes of one group in improving its PH-framed value equation can serve to fuel norms within the same group and across other groups to improve role performance.
What follows
This article builds on these premises by first distinguishing VDPH from other similar-minded approaches that have been put forward for health reform. It addresses the question, what is unique about VDPH?
This article next singles out workplace wellness, where without necessarily being recognized as such, VDPH has gained real traction among 1 group: employers. Key findings are evaluated in terms of psychometric performance to assess the progress workplace wellness has made at the level of VDPH and to illustrate how a more explicit embrace could help guide future employer initiatives toward firmer scientific footing.
The treatment of VDPH is then extended to another stakeholder group, providers, where leading members have made promising strides toward improving quality of care while reducing the costs of care. This paper highlights the promising breakthrough efforts recently reported by Lee et al.
A brief outline is then presented of a framework for broadening the use of VDPH by each of 5 stakeholder groups to improve role performance. This framework is predicated on the crosswalk comprised of the PH-framed value equation whose form is common across stakeholder groups. To illustrate how this shared equation's parameters differ by group, a list of measures for assessing VDPH performance by stakeholder group is suggested.
Positioning VDPH
Programs and policies for PH management collectively focus on the entire health continuum in defined populations, including the healthy, not just those with disease or at risk. They also broaden the criteria for defining health beyond the absence of disease to include well-being, functionality, and performance. Value-based strategies focus on the comparison of benefit (effect) and cost outcomes linked to options for achieving the same objective. Where feasible, evidence on these benefit (effect)/cost calculations is factored into decision making.
It is how VDPH integrates these 2 sets of principles that differentiates it from other like-minded approaches to health reform.
Value-based insurance design (V-BID)
The payer sector has introduced V-BID which, similar to VDPH, is based on analysis of costs and outcomes data to determine relative value. Through selective application of cost allocation mechanisms, V-BID functions to incentivize and encourage patients and providers to use high-value services linked with the most beneficial outcomes relative to costs. 15 The latest V-BID model, high-value health plans, appears to be garnering bipartisan support. High-value health plans provide clinically nuanced pre-deductible coverage for essential services to manage chronic disease while requiring high deductibles for low-value services to discourage waste. 16
As structured, V-BID mechanisms encourage behavior change for 2 stakeholder groups: patients and providers. This constitutes one difference with VDPH, whose focus extends to all major stakeholder groups. The management of their common scientific underpinnings further sets V-BID and VDPH apart. Rather than incentivizing and encouraging physicians and patients toward certain choices, VDPH management instead works to actively shape utilization–indeed management–by fostering norms akin to how treatment guidelines function.
Specifically, as patients and providers consider the options for improving patient health status, well-being, and functional status, VDPH guides them toward the option the evidence indicates likely will produce the best outcome-to-cost ratio. Likewise, as patients and providers assess the options for improving value in health care delivery, VDPH guides them toward the option likely to produce the broadest total health improvements. Situational parameters may lead to a different choice, but the latter is made with clarity as to why it is not the best VDPH option.
Cost-effectiveness analysis
Cost-effectiveness analysis (CEA) is an analytic tool that calculates and compares the costs and effects of a program, good, or service with at least 1 alternative in ratios of incremental cost to incremental effect. It is increasingly being applied by and/or for payers, providers, and suppliers.
Two features distinguish CEA from conventional cost-benefit analyses. First, the effects focus on health outcomes such as quality(disability)-adjusted life years, not monetary measures. 17 Second, in updated guidelines, 18 the call is made for the use of 2 reference cases, or sets of standard methods, to improve analytic quality and comparability. One focuses on the social perspective, which considers the broad allocation of resources and outcomes regardless of who experiences them. The other focuses more narrowly on resource allocation for the health care sector to better understand the consequences of interventions that fall outside the latter.
CEA, therefore, amounts to a focused inquiry between trade-offs that seeks the alternative that will deliver the most health for the least resources expended. As such, CEA is closely aligned with VDPH. But, with its focus on improving the PH-framed value equation, VDPH's reach extends beyond trade-offs. In each case, role performance can be made better by improving the numerator (outcomes), reducing the denominator (costs), or accomplishing both. 19 Each of these contingencies may or may not involve trade-off(s).
The Triple Aim
The Triple Aim refers to simultaneously improving the individual experience of care, improving the health of populations, and reducing per capita costs of care in populations. 20 Recently, calls have been made to add improving the work life of providers as a fourth aim. 21 A guiding rationale for reform under the ACA, the Triple Aim has been widely used by physicians, hospitals, and health systems to improve performance. Three components have been identified for optimizing management: creating the right foundation for population management; managing services to scale; and establishing a learning system to sustain the work over time. 22
Like VDPH, the Triple Aim targets a wide range of health outcome and cost metrics. Although there are differences, what is most notable is the overlap between the two. Yet, the Triple Aim sets its sights primarily on providers. Although other stakeholders may be targeted, it tends to be only to the extent that their actions impact (or do not impact) providers. In contrast, for VDPH a key premise is that all major groups impact the quality/cost dilemma and thus merit attention.
Moreover, the priorities that comprise their focus set the two apart. The Triple (Quadruple) Aim endeavors to improve patient (and provider) satisfaction, improve health outcomes, and reduce costs. The theme of investment is given little explicit emphasis. For VDPH, investing wisely is given highest priority. Entities in all stakeholder groups have options for improving role performance, and VDPH endeavors to prioritize and foster the wisest choices.
Table 1 summarizes the targets, science, and management criteria in these distinctions.
VDPH and Workplace Wellness
Bolstered by a growing body of evidence, marketplace trends, and incentives in the ACA, employers have increasingly implemented workplace wellness programs (also known as health promotion, disease management, and health and productivity management). These programs are designed to support and improve health and well-being. They also work to reduce health care service use and productivity loss by fostering better management of health behaviors, health risks and chronic disease. The annual Employee Health Benefits Survey has documented steady growth, with up to 46% of small firms and 83% of large firms offering health risk appraisals, biometric screening, and/or health promotion/wellness programs in 2016. 23
However, the results on program impact have been uneven and sparked controversy, 24 –26 in large part because of program variation. Separately, in 2014 RAND differentiated 3 types of services—health risk screening, lifestyle management, and disease management—and concluded that only 13% of wellness programs had extensive services in all 3 areas and could be classified as comprehensive. 27
As such, many observers maintain that how a program is designed is crucial. Pronk has identified 5 elements defining comprehensiveness: health education, supportive physical and social environments, program integration into the organization's structure, linkages to related programs, and worksite screening programs. Yet, comprehensiveness is just 1 of 9 dimensions that underlie a total of 44 best practices. His premise: the more progress is made on all dimensions, the better the odds of success. 28
The approaches of leading employers (eg, those recognized by the C. Everett Koop National Health Award) are exemplary. These employers have fused key management elements of PH and value, and have blazed a trail for use of VDPH by a stakeholder group.
Applying a Scientific Lens
The empirical work comprising the evidence on workplace wellness can be appraised in terms of validity (ie, the extent to which measures assess what they are intended to assess) and reliability (ie, the extent to which measures yield consistent results). 29 Employer efforts have made material progress relative to these guideposts even as more work is needed.
Face validity
An initial consideration is face validity. For measures to fulfill their purpose, they need to be seen as adequately tapping pertinent constructs in ways that are pivotal to organizational priorities. For employers engaging in workplace wellness, high on this priority list has been reducing health care costs and improving employee health and productivity/performance. 30
A core set of measures to address these priorities seems to have emerged. On the health care side, these include drivers and costs linked to inpatient admissions, outpatient visits, laboratory tests/imaging, and filled prescriptions. These measures also span indirect drivers and costs linked to health-related productivity loss, including presenteeism, health-related absenteeism, disability, and workers' compensation.
From the perspective of VDPH, these measures cut right to the heart of employer capacity to perform as purchaser on behalf of covered populations. With the exception of presenteeism, for which more standardization is needed, 31 they now enjoy broad-based employer support and thus exemplify the kind of role-specific impact metrics needed for each group.
Predictive validity
A second consideration concerns predictive validity. At issue here has been whether the implementation of workplace wellness has been linked to future changes on outcome measures that would be predicted if they were achieving their objectives.
A leading employer database offers findings on the multifaceted measurement and management approach to workplace wellness that Navistar evolved for its continental US workforce from 1998 to 2009. Navistar's approach 32 included the following management components, many of which were coordinated with the company's health plans, behavioral health services provider, or pharmaceutical benefits manager: company health personnel at all major company locations; on-site medical clinics; 16 disease management and health risk behavior programs; a workers' compensation/disability management program; and tiered drug pricing. It also included various measurement components: in-house and external databases; independent analyses by company personnel and external experts; dashboard reporting for senior management, and numerous “special topic” studies. 33
In analyses that tracked aggregate workforce changes from 2001–2009, 34 employees reported significant reductions in inpatient hospitalizations, outpatient visits, and filled prescription use, and across-the-board significant reductions in presenteeism, health-related absentee hours, and workers' compensation and disability episodes (Fig. 1). These reductions remained highly significant across healthy and major disease groups (eg, hypertension), even with controls for changes in workforce composition (eg, age).
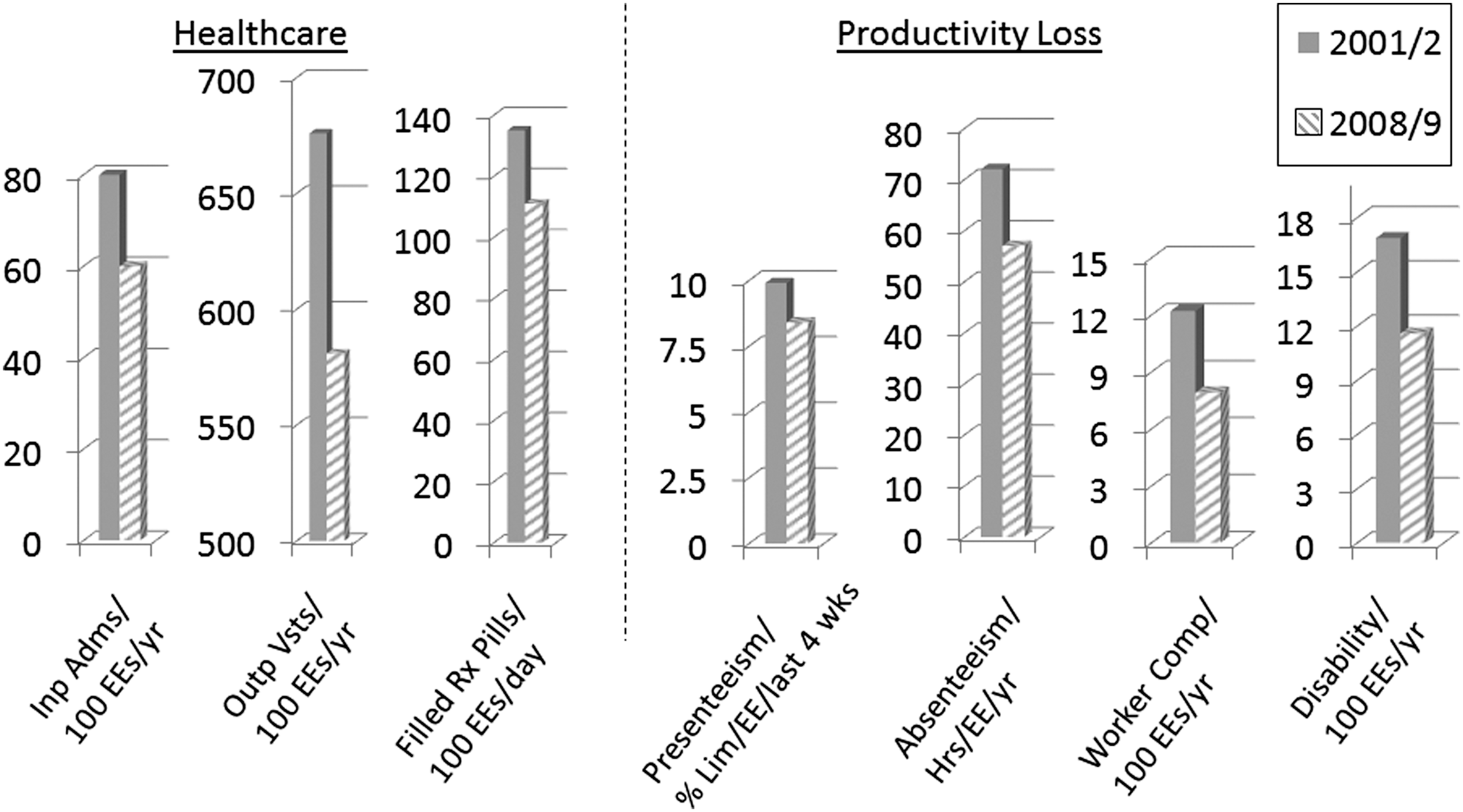
Drivers of health care utilization and productivity loss at Navistar from January 2001 to December 2009. Adjusted for changes in workforce demographics (eg, age) across the February 2001 to September 2008 time frame. Adapted from Allen et al. 34 EE, employees; Inp Adms, inpatient admissions; Hrs, hours; Lim, limited; Outp Vsts, outpatient visits; wks, weeks; yr, year.
This near-uniform pattern of results provided strong evidence of program effectiveness and exemplified similar results for employer wellness approaches elsewhere. 35 It also was consistent with VDPH. Not only was the approach linked to changes as predicted on measures of purchaser role performance, these changes registered across the health continuum.
Internal validity
Another consideration concerns internal validity, or the extent to which cause and effect inferences can be drawn from the methods deployed. At issue has been whether workplace wellness itself has produced the changes observed. Often challenged by issues of feasibility and utility, the gold standard of randomized clinical trials has rarely been possible in workplace wellness studies. Instead, investigators have resorted to quasi-experimental/statistical methods that have yielded improved but still not definitive bases for inferring cause and effect.
Employer interventions have targeted such health behaviors as smoking. 36 Consider the Health Enhancement Initiative (HEI) at WE Energies, a utilities company whose still ongoing 20+ year approach garnered the Koop Award in 2007. Health risk assessment responses are used to drive several programs for health promotion and risk behavior reduction that are designed to strengthen individual accountability. As of 2007, more than 85% of employees had participated since the program's inception, with more than 50% participating for 3+ years. 37
From 2003 to 2006, employees were designated as low- (0–2 risks), medium- (3–4 risks), and high-risk (≥5 risks) groups based on 12 health risk factors. A significant net migration of overall risk from higher to lower risk categories (ie, high risk: from 11.7% to 7.3%; medium: from 25.8% to 20.6%; low: from 62.5% to 72.1%) was observed. Moreover, a study of return on investment (ROI) found a cumulative ROI from health care costs and time away from work of 1.66 from 1999–2007. 38
Research on HEI impact has continued and now includes comparisons of observed risk with concurrent estimates of risk that would be expected in the absence of the intervention, computed using the Edington Model of Normal Risk Migration. Figure 2 tracks the observed and expected low-risk group percentages in a panel of 684 employees across annual assessments spanning 2014–2016 (D. Edington, PhD, e-mail communication, 2016). In 2014, those at low risk comprised 74% of the panel. By 2016, the expected low-risk group percentage recorded a net drop of just over 4½ percentage points. This compares to the corresponding actual net drop of less than 1 percentage point, underscoring the need to correct for the normal migration of population risks.

Change in low health risk population: post intervention (observed) versus natural migration of risk (expected). 2014–2016 Employees who have completed 3 consecutive annual health risk appraisals.
Such refinements are increasing confidence in the estimates of wellness impact being reported. Yet, studies of health risk reduction have yet to systematically address other factors that also could affect behavior change (eg, household/family support). Although progress has been made, more work is needed to put these and other internal validity concerns to rest.
Reliability and external validity
Workplace wellness more recently recorded another milestone with studies that conducted simulated comparisons of the stock performance of the Standard & Poor's (S&P) 500 Index versus portfolios of employers with superior wellness programs. 39 –41 In brief, 3 different sets of investigators conducted these studies. The methodology for each was essentially the same: stock price was monitored before and after receipt of the superior designation; dividends were reinvested quarterly; and the portfolio was rebalanced each year after new award-winning companies were announced and added. Each of 3 portfolios was found to outperform the S&P 500 by substantial margins. The average annual increment of each portfolio's gain over the corresponding S&P Index gain ranged from 8% to 15% (Fig. 3).
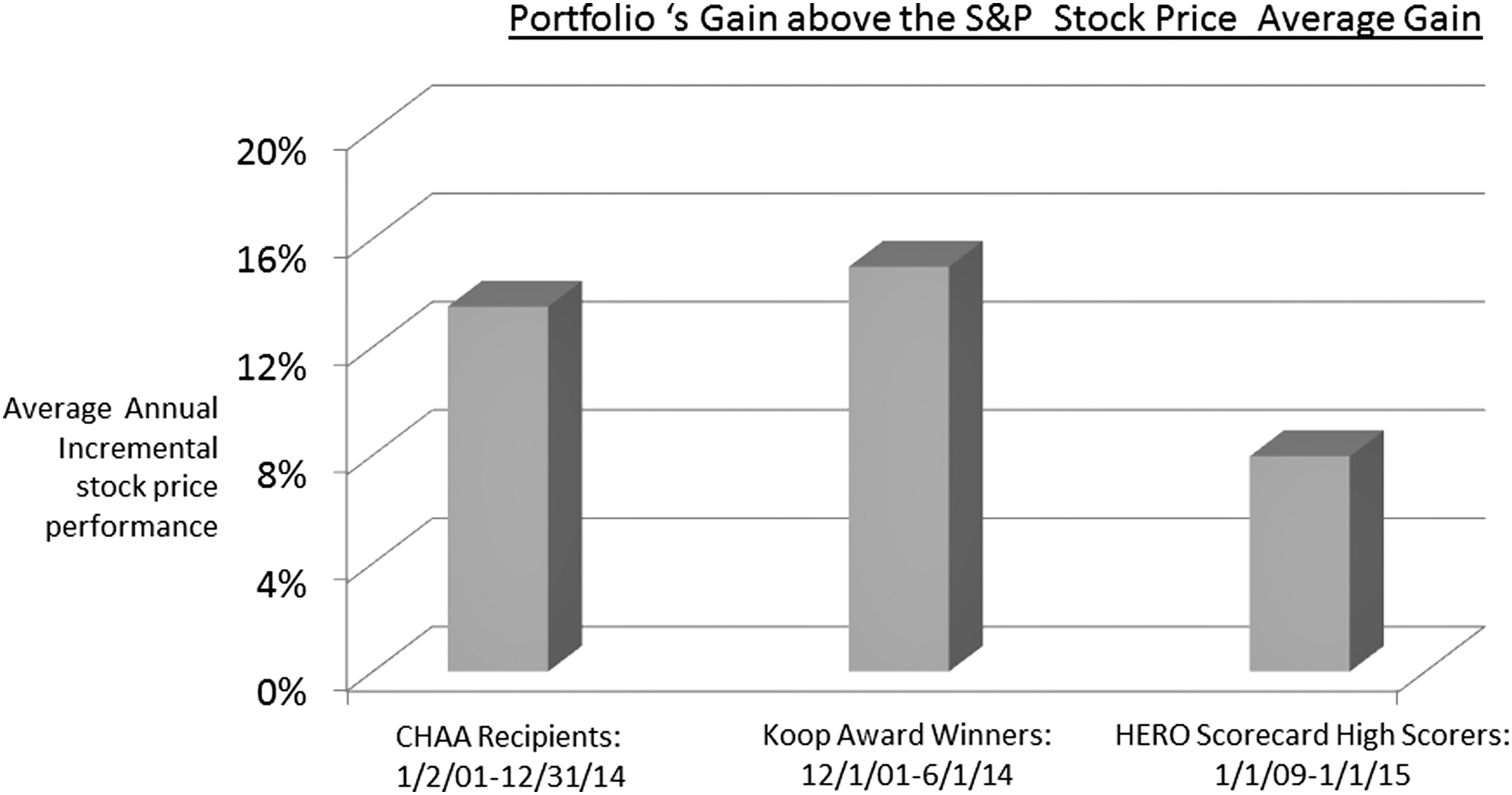
Cumulative stock performance: three portfolios of employers with superior workplace wellness programs vs. S&P 500 Index. CHAA, Corporate Health Achievement Award; S&P, Standard and Poor's.
These results can be viewed in terms of 2 types of reliability. The first concerns parallel-forms reliability, or the extent to which multiple tests constructed in the same way give consistent results. The second concerns interobserver reliability, or the extent to which different observers give consistent estimates of the same phenomenon. The 3 teams applied different incarnations of the same method on different sets of companies and obtained results in the same direction with similar orders of magnitude–an ample show of reliability on both counts.
These results also can be viewed in terms of external validity, or the extent to which results can be generalized to other situations as theory would predict. Although the correlational evidence yielded partial support for generalizability, none of these studies attempted to control for the possibility that these high-performing companies also excelled on other corporate practices over and above wellness (eg, workforce education and training). Hence, there was no way to separate out the specific contributions of workplace wellness from the effects of other corporate practices that could have affected stock price.
VDPH and Providers
As with leading employers in the workplace wellness space, momentum has been growing among providers to improve quality of care relative to the costs of this care. Since 2000, leading providers and their catalysts have reported striking gains. Virginia Mason's use of Lean production to improve quality and safety while eliminating waste is one example. 42 The Institute for Healthcare Improvement's recent synthesis of 7 years of collaboration with 141 participating organizations to finalize principles for guiding Triple Aim efforts is another. 22
The recent growth of accountable care organizations (ACOs) exemplifies this momentum. Premised on the idea that accountability will create care efficiencies, improve quality, and lower costs, ACOs are contractual arrangements whereby providers enter into a risk-based agreement with a payer to take on financial risk associated with the care and outcomes of a defined population. 43 From zero when the ACA was passed in 2010, a total of 838 ACOs were actively operating as of January 2016, with service areas in all 50 states and the District of Columbia. A total of 1217 contracts covered 28.3 million lives, with 61%, 29.3% and 2.9% of these enrollees in commercial, Medicare, and Medicaid ACOs, respectively. 44
Yet, in what are perhaps the most comprehensive results reported on ACO performance to date, the 220 ACOs in the Medicare Shared Savings Program (MSSP) have shown mixed initial success with respect to improving quality and reducing costs. One study tested whether changes in spending or quality from the pre-contract to a post-contract period for 2 cohorts of MSSP ACOs entering in 2012 and 2013 differed from concurrent changes for local non-ACO providers. The first full year of MSSP participation was associated with early savings among 2012 entrants but not 2013 entrants. Moreover, performance on quality measures differentially improved in the ACO cohorts on a few measures but did not differentially change for other measures, and there was no differential change in the use of low-value services. 45
A second study compared the actual performance of the MSSP ACOs on the program's quality metrics in their first year in the program with CMS benchmarks for these measures. To earn Quality Incentive Payments in the second and third years, any earned savings would be subject to actually reaching prespecified benchmarks. Overall, the results showed that there was considerable room for improvement. Of the $296.8 M in earned savings distributed in the first year, $71.1 M proved subject to being withheld because of failure to achieve full-standard quality. Furthermore, when first-year quality data were extrapolated using third-year payment calculations, the ACOs on average would have qualified for 74% of their share of total savings. 46
In large part, these early reports reflect the difficulties that long-entrenched fee-for-service reimbursement continues to pose for the shift from volume to value. But these reports also highlight the need of providers–even those embedded in ACOs–for a sustained in-house approach for tackling the PH-framed value equation that governs their role performance.
Value-driven outcomes tool
The measurement/management approach that Lee et al recently reported for optimizing care for specific medical conditions at University of Utah Health Care (UUHC) would seem a promising candidate. 47 Described elsewhere by acknowledged experts as forging a new path from volume to value, 48 this approach eschewed conventional tactics such as targeting all patients in high-cost areas such as readmissions. It instead introduced a new tool, labeled value-driven outcomes, to allocate clinical care cost and quality measures to individual patient encounters, prioritize improvement opportunities based on cost and quality variation, and support physician collaboration with process improvement experts to improve quality and cost outcomes.
In their 3-year, uncontrolled, pre-post study, Lee et al evaluated program impact on the direct care cost and quality composite indices targeting 3 clinical areas exhibiting high cost and quality variability: total hip and knee replacement, hospitalist laboratory testing, and sepsis management. For total joint replacement from baseline to 1-year post implementation, the quality index increased from 54% to 80% while mean direct costs decreased 11%. Mean laboratory testing costs per day decreased from $138 to $123 from baseline to the evaluation period with no significant change in mean length of stay. For the sepsis intervention, the mean time for appropriate anti-infective administration dropped from 7.8 hours to 3.6 hours.
As investigators consider how to advance this work, the progress that leading employers have made on validity and reliability criteria with respect to workplace wellness offers corollaries that are applicable.
Striving for common measures
One issue concerns priorities and measures that reflect these priorities. In their focus on clinical practice pathways that can gauge progress toward improved health outcomes and lower delivery costs, the Lee et al measures are consistent with the priorities that VDPH would encourage for providers.
Of concern is the risk of curtailing the capacity to learn from interventions elsewhere. To what extent will the Lee et al measures facilitate, not impede, dialogue on results, not just internally within UUHC but also externally with other providers? The temptation may be to become insular and ignore comparability. VDPH would have consensus-building with external parties and different stakeholders begin now on mutually agreed-upon goals and metrics.
Discerning cause and effect
For workplace wellness, questions of cause and effect have centered on whether it accounts for the gains reported. As pressures mount for greater transparency, employers are likely to encounter growing demands for data that clearly and credibly differentiate the changes their wellness programs are inducing. Similar dynamics can be expected as use of Lee et al's tool widens and management predicated on its usage proliferates.
Questions of internal validity in the clinical space often hinge on complex protocols marked by intricate sequences of steps, with testing focused on identifying the specific sequences that deliver the best results. The need to document this testing and the clinical decisions made as a consequence in formats that are publicly accountable will likely intensify. Lee et al acknowledge the need for comparison/control groups and statistical methods that address these demands. VDPH would prioritize this direction and support accelerating it.
Differentiating contributions to health
Already discussed were the recent studies by different investigators that applied essentially the same method and found that 3 employer portfolios outperformed the S&P 500 by substantial margins. Yet, the extent to which well-done workplace wellness can be specifically attributed as the cause of the portfolio gains requires greater clarity.
Lee et al mention that their patients came mostly from Utah, whose younger, more physically active population characteristics may limit the generalizability of their results. Further tests replicating their tool in health systems elsewhere will address this limitation. But, VDPH would further focus investigators on the growing recognition that various factors (eg, poverty, access to care) often outweigh clinical decision making in determining health outcomes. When it comes to outcomes, just what are providers responsible and not responsible for?
Here providers face an external/internal validity challenge not too dissimilar from purchasers, and VDPH would urge investigators to seek out ways to apply the Lee et al tool. Such applications likely will need to be comprised of up-front in-house analysis of quality and cost variation and subsequent collaboration between physicians and process improvement experts. But they also need to be configured to be sensitive to VDPH outcomes in the larger societal context. One issue, for example, is whether it is the health care organization or some other (eg, philanthropic) entity that measures and manages the full array of outcomes. 49 Another concerns the collaborative activities that will be needed across these entities and how these activities and the investments are measured. 50 In both cases, VDPH likely will require that the PH-framed value equation governing provider role performance be revisited.
Broadening the Applicability of VDPH
The common interests that providers and purchasers share in advancing health 13 underscore the promise of adapting these linkages from employer workplace wellness successes to future provider efforts to build on the Lee et al work. The same applies to all major stakeholder groups whose role performance impacts the quality/cost dilemma in health and health care.
VDPH by stakeholder group
Figure 4 offers a summation of VDPH as a strategy for improving role performance for each of 5 stakeholder groups: providers (eg, physicians, hospitals, health systems), purchasers (eg, employers, government), suppliers (eg, pharmaceutical firms, specialty vendors), payers (eg, commercial and public health plans), and patient/consumers. For each group, a brief distillation of the objectives that VDPH pursues to improve the PH-framed value equation that governs role performance is offered as well as a tool, lifted from the foregoing discussion, that has been or could be deployed to improve that group's role performance. To provide context, the overall results that VDPH targets at the system level from these separate stakeholder streams of activity also are listed.
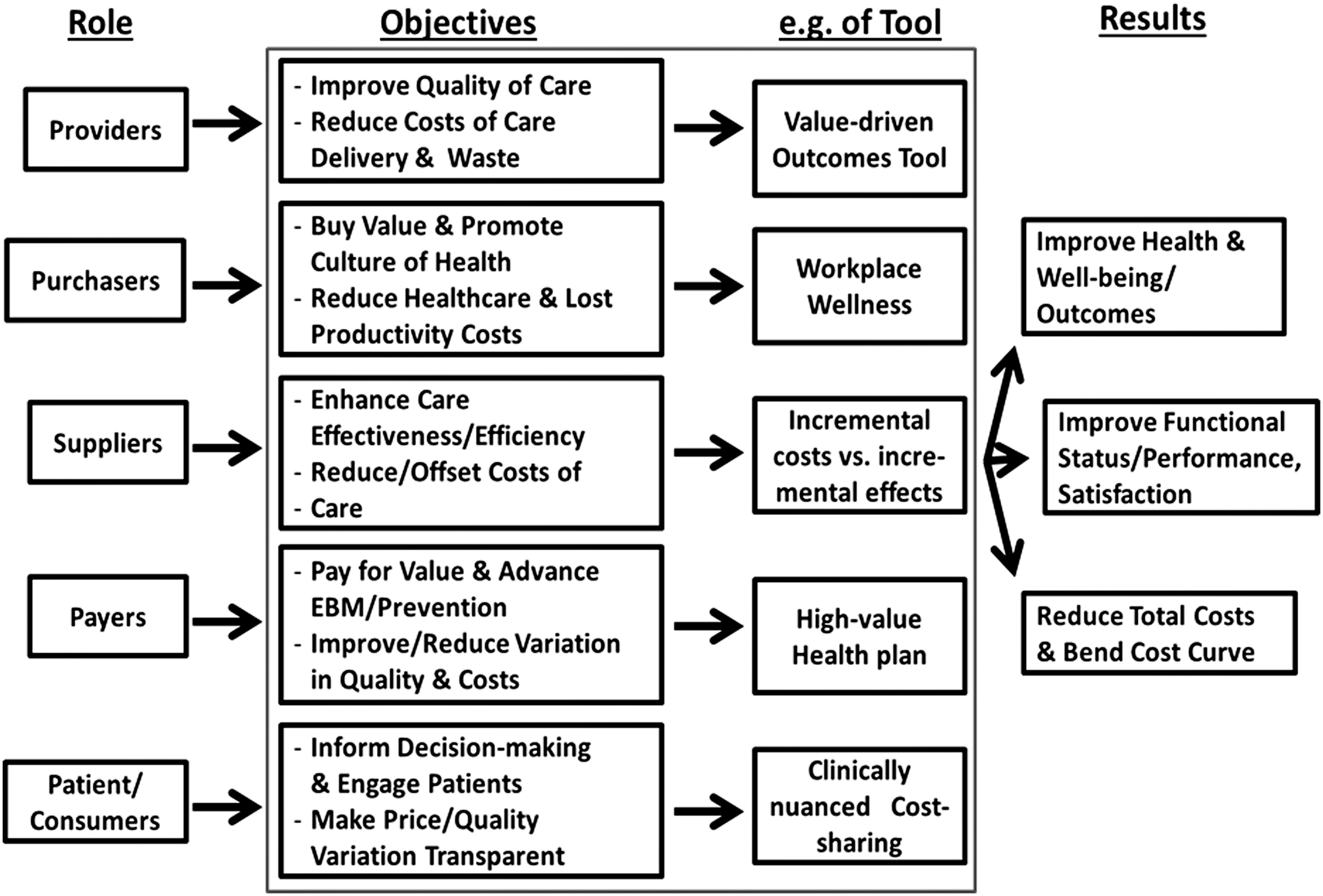
Value-driven population health: improving stakeholder role performance. EBM, evidence-based medicine.
Implicit is the assumption that members in each stakeholder group are going to face increasing pressures in the marketplace to perform their role in ways that contribute to the collective attainment of better health outcomes at reduced costs. They each will need to realize and show material progress in doing their part. To achieve this progress, the evolution of the science of VDPH that applies to their role can help to point the way. This evolution is likely to increase the credibility of–and confidence in–the steps identified as best practices that each group can take to improve the PH-framed value equation governing its role performance. It could well facilitate the uptake of VDPH by each stakeholder group in the marketplace.
To help advance this evolution, the foregoing discussion has examined recently reported work by leading employers in the workplace wellness space, and by leading providers in the quality of care improvement/cost reduction space, through a scientific lens of validity and reliability criteria. These criteria have functioned as guideposts for informing and shaping the evidence acquisition and synthesizing activities of future studies that can serve to strengthen the scientific footing underlying each group's management of VDPH to improve role performance.
As such, this treatment yields an initial road map with some pointers for other purchasers and providers as well as other stakeholder groups. For each group, this road map encompasses the stakeholder equivalent of the following milestones, although not necessarily in this sequence: • Adoption of the VDPH vision for their stakeholder role, the prerequisites of this role, and measures that adequately reflect these prerequisites. • Use of these measures in contextually viable studies to develop evidence for improving role performance. • Implementation of interventions based on this evidence and evaluations of their impact. • Broadening of performance distinctions based on these evaluations to more encompassing questions of organizational functioning in the marketplace. • Continued strategy refinement based on this cycle to maximize stakeholder role performance and advance the science of VDPH.
Figure 5 suggests a list of measures for monitoring the performance of each of these 5 stakeholder groups in light of this road map. As shown, these measures focus on 1 or more outcome and cost reduction objectives that comprise the PH-framed value equation for each group, with each measure expressed as an average for the defined population. This list is tendered as a work in progress at a high level. In each case, more research is needed to cultivate consensus, not only with respect to item content, but also with respect to method aspects (eg, sampling) that will determine how corresponding data are acquired, examined, and interpreted.
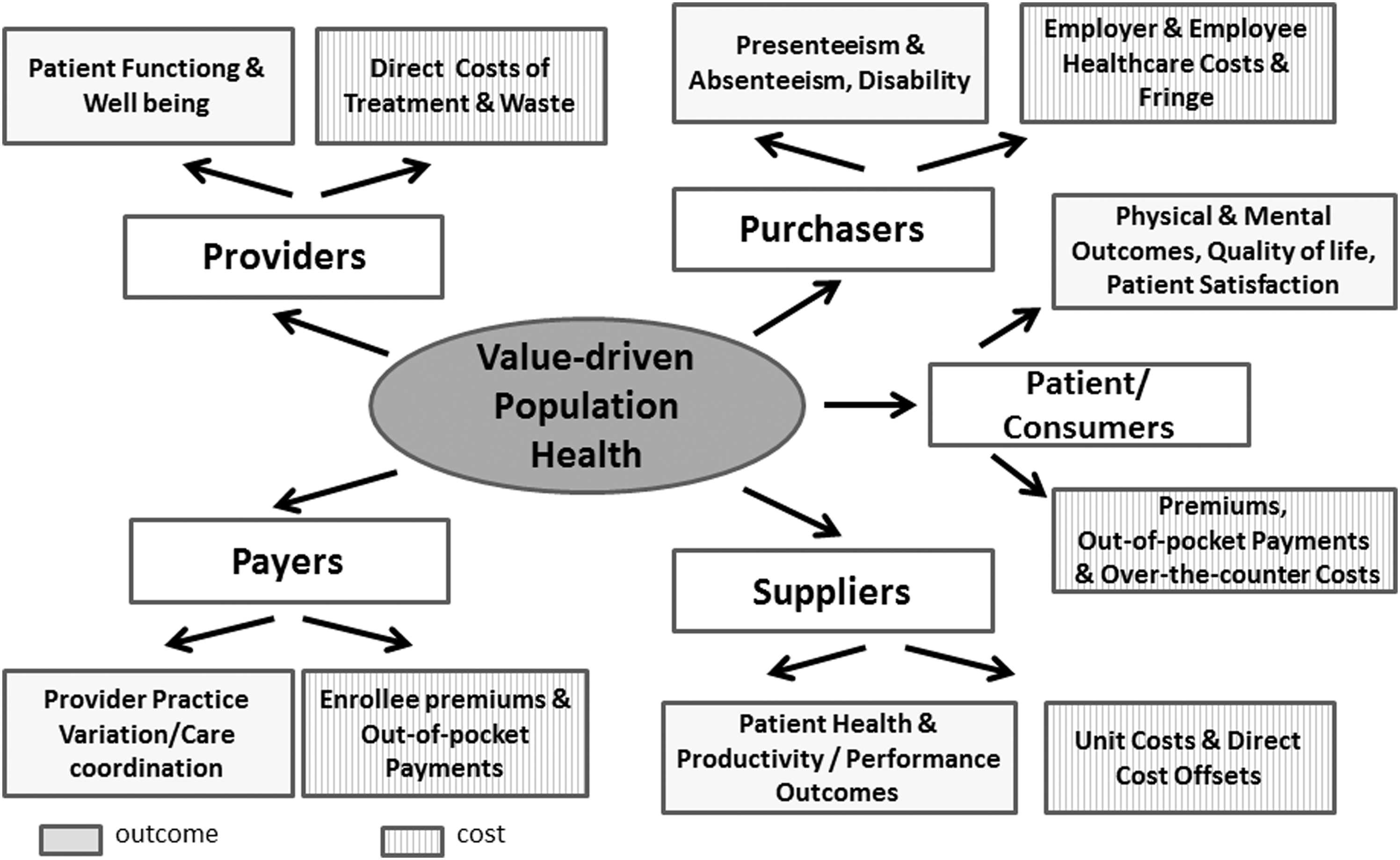
Value-driven population health performance measures for five stakeholder groups: a working list. All measures computed as averages for the defined population.
Implications for health reform
VDPH offers a strategy for health reform that confers several potential advantages. One stems from its inclusion of all major stakeholder groups. Adroit application of the science and management of VDPH for each group offers the possibility of bringing each into closer collective alignment.
A second derives from VDPH's incorporation of these other approaches for health care reform. The overarching framework afforded by VDPH endeavors to utilize whatever has been shown or has the potential to deliver greater PH-framed value. The track records that V-BID, CEA, and the Triple Aim have amassed have amply demonstrated the capacity of each in this regard and, to this end, tools drawn from each are classified here as levers for promoting VDPH in the marketplace. Just as the VDPH crosswalk can serve to support each stakeholder group's drive toward improved role performance, VDPH can harness the strengths of these approaches and foster their harmonious usage.
Finally, as the revision of the Affordable Care Act gains momentum, VDPH is predicated on a “both/and” (as opposed to an “either/or”) mind-set that can serve to consolidate recent gains in value achieved under the ACA while also supporting new more marketplace-oriented priorities. Embedding new legislation with tax incentives that promote each stakeholder group's objectives in Figure 4 offers just 1 example on how it can used to bolster the new administration's vision of a strengthened health care marketplace. How VDPH is adapted likely will do much to determine its usefulness in the years ahead.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dee Edington, PhD for his input on ideas developed in this paper and the anonymous reviewers for their comments.
Author Disclosure Statement
Drs. Allen, Burton, and Fabius declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the development of this paper.