
Abstract
Through retrospective chart review, this study described characteristics and length of stay for a cohort of newborns discharged on methadone following an inpatient weaning for neonatal abstinence syndrome (NAS). Data were assessed for all term infants born between January 1, 2010, and December 31, 2014, admitted to the hospital with a co-diagnosis of NAS at discharge, for gestational age, length of stay, days on treatment protocol before discharge, time to once-daily interval methadone dosing, and hospital charges, as well as for categorical characteristics. The 53 patients were predominantly male (58%), white (71%), and covered by Medicaid insurance (72%). Mean gestational age was 39.5 ± 1.1 weeks; length of hospital stay was 11.8 ± 5 days. Common co-diagnoses were newborn feeding problems (26%) and neonatal hypoglycemia (23%). In conclusion, use of the study site's methadone weaning protocol, which can be easily replicated, resulted in a relatively short length of stay and low readmission rates for these patients.
Introduction
N
It has been estimated that term newborns with NAS stay hospitalized for an average of 16.9 days compared to 2.1 days for those without NAS. Average costs for term newborns with NAS were estimated at $66,700 compared to $3500 for those without NAS. US health care expenditure related to NAS treatment reaches as high as $1.5 billion dollars per year, with the average stay costing in excess of $50,000. The bulk of these costs (∼80%) fall to state Medicaid programs. 4
Previous research has shown that inpatient management using traditional strategies of care for infants with NAS led to a length of stay ranging from 8–105 days with a median of 25–34 days. 3 –5 Oei et al 6 found that inpatient length of stay was decreased with the establishment of an outpatient clinic designed specifically for managing NAS patients.
Establishing a procedure for infants with NAS to be discharged from the NICU and managed at home has several advantages. Outpatient management has been shown to increase opportunities for maternal-infant pair bonding because of shorter hospital stays and increased rates of breastfeeding. 7 Abdel-Latif et al 8 found that breastfeeding during the outpatient management of NAS led to reduced withdrawal severity, delayed onset of NAS, and decreased need for pharmacologic treatment. Backes et al 9 calculated that patients in combined inpatient-to-outpatient management saved an average of $13,817 in hospital cost per patient compared to a traditional, inpatient-only management strategy.
This retrospective review assessed data from NAS patients discharged from the NICU after implementation of a standard transition consensus. The goal of the consensus was to outline appropriate weaning of medications used to treat opioid-exposed infants to improve the quality of care for the infants, standardize the approach to weaning, decrease inpatient length of stay, decrease hospital charges, and minimize the need for readmission.
This study aimed to characterize the demographics of those infants with NAS in the study population. Secondary outcome variables assessed included length of stay in the neonatal intensive care unit for NAS patients, and time from initiating methadone to achieving every 24-hour dosing. Also assessed was the number of readmissions for this cohort of NAS infants within 30 days of discharge.
Methods
This study was conducted at the main hospital campus of a large tertiary care health network in southeastern Pennsylvania. The setting can be described as suburban, but situated within 5 miles of the downtown urban area of the third largest city in Pennsylvania. After approval from the study organization's Institutional Review Board, the study team reviewed all term infants born between January 1, 2010, and December 31, 2014, and admitted to the hospital with an International Classification of Diseases, Ninth Revision co-diagnosis of NAS (779.5) requiring opiate therapy at discharge. All cases with this diagnosis were verified with chart review to assure that this code was appropriately linked to each case. Term infant was defined as an estimated gestational age (EGA) at or greater than 37 weeks. Data were collected independently by 2 investigators via electronic medical records (EMRs). Patients were excluded if they were treated for NAS for exposure to medications other than opioids, had an EGA <37 weeks at birth, had congenital anomalies, had iatrogenic NAS related to opiate administration while in the NICU, or were admitted to the NICU for NAS but did not need pharmacologic therapy. Also excluded were infants of multiple gestation pregnancies.
The study team assessed means and standard deviations of numerical data: estimated gestational age, total hospital length of stay, total days on methadone treatment protocol before discharge, time to once-daily interval methadone dosing. The team found the mean for the total hospital charges. The team also looked at frequencies for categorical data: sex, race, primary payer, 30-day hospital readmissions, need for breakthrough morphine dosing during hospital stay, and primary care provider. No patients completed NAS treatment before discharge, as this was not the goal of the weaning protocol. Readmissions noted were only those recorded at the home institution. All included patients were in the methadone weaning program through the entire protocol unless they were readmitted. It is unclear how many were lost to follow-up after the methadone wean. All statistics were generated using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Description of NAS management consensus
The NAS consensus at the study site was developed for newborns in the NICU with consistent Finnegan scores 10 >8. In addition to pharmacologic management, the infant also should receive nonpharmacologic measures including comfort measures such as swaddling, low light, clustering of care, and the use of a pacifier; nutritive therapy such as supplementation with high-calorie formula, and breastfeeding or providing expressed breast milk per American Academy of Pediatrics (AAP) guidelines; environmental modifications such as providing a quiet, low-stress environment; and room assignments where light can be dimmed and external stimuli can be minimized. Early and frequent breast feeding is encouraged if the infant's mother is compliant with her outpatient maintenance program as verified by NICU case management as well as by the mother's obstetrician. The mothers are permitted to visit any time; in fact, they are encouraged to visit as often and long as possible to encourage bonding and decrease withdrawal symptoms. The hospital NICU is a mix of private rooms and a ward design. Infants with NAS are prioritized to be placed in private rooms. Kangaroo care is encouraged to ease NAS symptoms.
In the term nursery, the infants are scored after each feed via Finnegan scoring. In the nursery, the infants stay in their mothers' rooms full time. If an infant scores 3 consecutive Finnegan scores of ≥8, he or she is admitted to the NICU and evaluated for the need for pharmacologic therapy. Pharmacologic therapy, if needed, consists of methadone initiated at 0.1 mg/kg/dose every 6 hours for infants with scores consistently ≥8. Morphine also is provided at 0.1 mg/kg/dose every 6 hours as needed for breakthrough NAS symptoms. The methadone dose is increased when scores remain consistently ≥8 or where multiple breakthrough morphine doses are required. An algorithm describing the dosage management of methadone is shown in Figure 1. No other medications were used as adjuvant therapies.
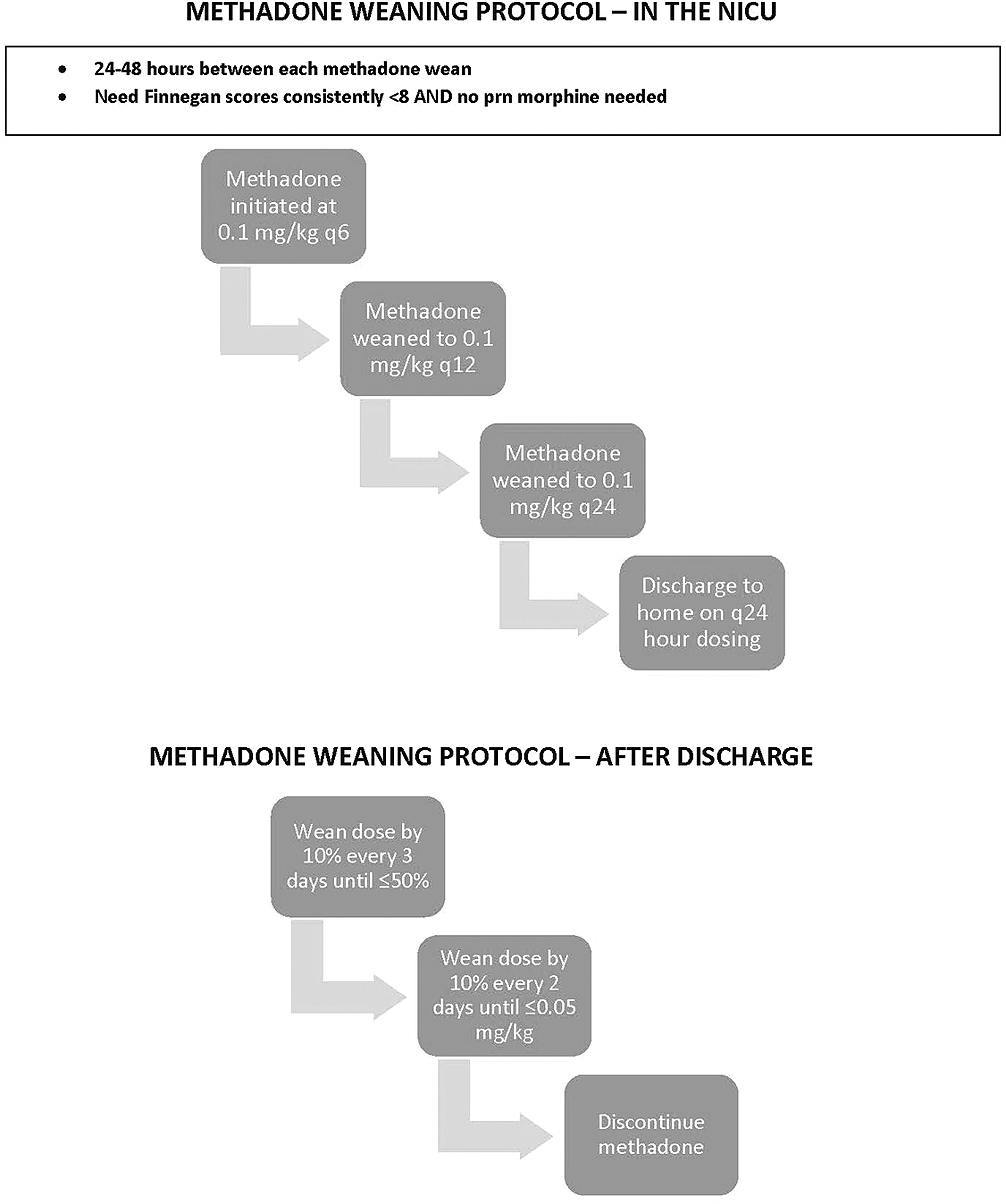
Methadone weaning protocol. NICU, neonatal intensive care unit; prn, as needed.
Once Finnegan scores remain consistently <8 for 1 to 2 days on once-daily therapy without the need for dose escalation or additional breakthrough medication, a weaning approach is generated for discharge. The mother or caregiver is taught by the nursing staff how to administer the methadone at home. All mothers and/or caretakers who are to take their babies home on methadone are screened by case management, county Children and Youth Services, and the Child Advocacy Team at the study hospital. If symptoms of withdrawal are present at any time during the outpatient weaning process, the parents are advised to contact the infant's pediatrician for clinical assessment.
The total exposure of methadone for a 3 kg infant (as in the example in the weaning protocol algorithm) is 4.02 mg of methadone, which is 1.34 mg/kg of methadone exposure for the total weaning protocol.
Organizational resources such as a dedicated pediatric pharmacist, a hospital outpatient pharmacy with knowledge of the outpatient weaning protocol, and an integrated EMR system are all utilized to implement this weaning protocol in terms of orders and dose verification while the infant is an inpatient. On the outpatient side, the parents come to the outpatient pharmacy at the hospital weekly for prescription refills. This helps validate dosing as well as verification that the family is using the health care system appropriately and that the prescriptions can be easily tracked via the EMR and the dedicated pediatric pharmacist.
Results
A total of 53 patients were identified who met the aforementioned inclusion criteria. All infants who were started on methadone were sent home with a caregiver.
Patient characteristics
The mean estimated gestational age of the patient group was 39.5 weeks (SD = 1.1 weeks). The patient categorical variables, shown in Table 1, indicate predominantly male and white infants. The majority of the patients were covered by Medicaid insurance plans.
Treatment and hospital stay
The mean total length of hospital stay for the patient group was 11.8 ± 5 days. Additional summary measures for treatment and hospital stay (eg, gestational age, treatment days) are shown in Table 2. Of the 53 patients treated with methadone, 37 (69.8%) required breakthrough morphine treatment during their inpatient stay. No patients were off methadone before discharge home.
Q24, every 24 hours.
Co-diagnoses in patient cohort
The most common observed co-diagnoses in the patient cohort were newborn feeding problems (9 infants, 26%) and neonatal hypoglycemia (8 infants, 23%). Low birth weight affected 6 of the infants, with 4 (12%) weighing 2500 g or more and 2 (6%) weighing from 2000 to 2499 g. Four infants (12%) experienced transitory tachypnea, 3 (9%) had respiratory problems after birth, and 3 (9%) suffered from newborn hypothermia.
The mean total hospital charge, provided by the study organization's finance department, for each of these patients was $58,257. In all, 32% of the pediatricians to whom the infants were discharged were employed in the resident clinic of the study hospital, while the remainder were in a variety of different physician practices in the community.
No patients were weaned off medication before discharge and no patients in the study withdrew from the weaning program as outpatients unless they were readmitted to the hospital as described in the isolated cases in the following section. All infants that were started on methadone were sent home on methadone.
Readmissions rate
Five 30-day readmissions to the study hospital occurred within this group, with 3 related to NAS, to give a 5.6% readmission rate for NAS in this cohort. The first patient was readmitted for neonatal drug withdrawal symptoms (NDWS) 11 days after initial discharge and was later discharged 16 days after readmission. The second patient was readmitted for NDWS and concomitant gastroesophageal reflux 24 days after discharge, was stabilized, and then discharged 3 days later. The third patient, readmitted for NDWS 28 days after initial discharge, tested positive for respiratory syncytial virus on the third day of stay; that patient stayed in the hospital for 6 total days.
Of the 2 readmissions unrelated to NAS, the first patient was readmitted for congenital pyloric stenosis 14 days after initial discharge and was discharged the next day. The second patient was readmitted for respiratory syncytial virus bronchiolitis 9 days after initial discharge with no recorded issues with methadone weaning during the length of hospital stay.
Discussion
The increasing NAS epidemic has created a significant burden on the American health care system in terms of care needs and health care expenditure. NAS has typically been associated with an extended hospital stay because of the time it takes to wean the patient off opiate replacement therapy (eg, morphine) before discharge. This study illustrated a health care system that created guidelines for the administration of methadone for the patient, with the goal of reaching a daily dose that can be managed by the infant's caretaker, and a protocol for weaning with the assistance of the primary care physician.
Although this was a small single-center study, a similar high percentage of Medicaid-insured patients among the study cohort was noted as has been reported by larger studies. 1,11
The length of stay achieved in this study, an average length of 11.8 days with 9.8 days of methadone, is comparable to that shown by Backes et al 9 in a combined (inpatient and outpatient weaning) cohort and is a notably shorter hospitalization than the ∼23-day length of stay for inpatient weaning demonstrated by previous studies. 1,11 Substantially reduced charges are realized by having the child discharged to home for the remainder of the weaning process. Hospital charges for pharmacologically treated NAS infants have been estimated at $93,400, 1 while the study institution's charge per patient was considerably less at $58,400. The patients were seen for regular well-child appointments as per the AAP periodicity schedule and as needed should any concerns arise.
The small percentage of readmissions is similar to prior research studying outpatient NAS treatment. 9,12 Methadone therapy offers the advantage of once-daily dosing compared to 4 or more doses per day with morphine used in other outpatient treatment protocols. 12 This is a significant convenience factor for families and may support greater compliance with therapy, potentially enhancing the success of the outpatient protocol. Methadone pharmacokinetics for inpatients treated for NAS show an early stabilization of NAS symptoms with very rare occurrence of somnolence or respiratory depression, also potentially enhancing the success of the protocol. No study regarding the safety of outpatient methadone dosing has yet been done. 12 A key concern of outpatient methadone is dosing accumulation and possible overdosing, which has not been studied to date.
Other methods could be formally incorporated into this protocol going forward. Nearly 74% of the infants in this study were formula fed for at least part of the inpatient stay. Further encouragement of breastfeeding can help reduce NAS symptoms by the passage of the mother's medication into the breast milk. Methadone and buprenorphine are not contraindicated in breastfeeding and are both transmitted at low levels through breast milk. Using maternal breast milk can decrease length of stay. Infants receiving maternal breast milk can be weaned from their medication quicker and discharged earlier because of the steady low dose of opiates given to the infant through maternal breast milk 11 Going forward, length of stay in the study institution's population can potentially be reduced further should more mothers breastfeed their withdrawing infants. Similar ideas such as rooming-in for the mother 11 also may be promoted in combination with a methadone weaning protocol such as this one to further reduce length of stay and hospital charges. Formally empowering the mother at discharge to continue kangaroo care and breastfeeding also could help reduce readmissions.
Limitations of this study include the retrospective design and the relatively small sample size from a single institution, which limits generalizability of the findings. The infants are predominantly male, which is unusual, though the predominance of white infants fits prior studies. Specifics regarding the outpatient course outside of readmission rates were not within the scope of this study, limiting follow-up data regarding the results of the home weaning protocol.
This study adds to the few publications the study team found about the processes and benefits of a successful outpatient methadone weaning program for NAS. Use of a program such as one described here, which can serve as a model for other institutions, eliminates the prolonged hospital stay necessary when infants with NAS remain in the hospital for the entire weaning period. Potential benefits include shortened length of stay, low readmission rates, and reduced costs, not to mention increased opportunity for mother/baby bonding and, hence, lessening of withdrawal symptoms. A dearth of literature about the topic of the long-term successes and failures of outpatient weaning programs provides fertile ground for further research. With the growing recognition of this epidemic, outpatient management of NAS will undoubtedly be of increasing interest to families, providers, payers, and population health researchers.
Footnotes
Acknowledgments
The authors are grateful to Claire F. Kukielka, MS, CPHQ, Clinical Quality Specialist, for assistance in data inquiry and to Jacqueline Grove for manuscript editing and preparation.
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.