
Abstract
The need for population health management expertise has increased as the health care industry shifts toward value-based care. However, many organizations report hiring gaps as they seek to fill positions. The purpose of this study was to analyze the types of population health management positions for which health care organizations are hiring, including qualifications and competencies required for these positions. A content analysis was conducted on 271 job postings collected during a 2-month period. A typology of qualifications and competencies was developed based on the content analysis. Profiles were generated for the top 5 job title classifications: directors, coordinators, care managers, analysts, and specialists. This study highlights the investment health care organizations are making in population health management and the prominent role these positions are playing in the health care environment today. Many organizations are building out population health management teams resulting in multiple positions at different levels being added. As the market demands competent candidates who are equipped with specialized population health expertise as well as practical experience in program development, technology applications, care management, and analytics, professional education programs will need to adapt curricula to address the required areas. Competencies for specific job title classifications may need further evaluation and refinement over time. Study results can be used by organizations for strategic planning, by educators to target needed qualifications and competencies, and by researchers and policy advisors to assess progress toward value-based care.
Introduction
H
Other research has noted the challenges of identifying candidates with the needed expertise to fill population health management positions. A recent survey of health care executive search firms identified the increased need for more population health roles, physician leadership, and more roles focused on clinical integration and/or medical group management. 6 The most in-demand competencies included change management, emotional intelligence, ability to influence, strategic thinking, collaboration, innovative thinking, and critical thinking, with innovative thinking being the most difficult skill to find. 6 Deep experience in population health management also was cited as being a difficult skill set to locate. 6 Research by the AHA has also noted that population health is a challenging skill set to find, with more than 40% of survey respondents listing population health management as a talent gap within their organizations. 7 Because of the need for population health expertise and current hiring gaps, it is important to understand qualifications and competencies required for these positions.
Because the industry shift to value-based care is fairly recent, very little academic research has been conducted as to what types of positions health care organizations are adding with regard to population health management. Thus, the purpose of this study was to analyze population health management job postings and identify the qualifications and competencies required for these positions. This study was guided by the following research questions: • What are the types of population health management positions for which US health care organizations are hiring? • What job qualifications and competencies do US health care organizations require to support population health management efforts? • How do population health management job qualifications and competencies vary by job title classification in the United States?
To address these research questions, a content analysis of population health job postings was conducted. Job postings can reveal current hiring trends and desired qualifications and competencies that employers seek in positions. Content analysis of job announcements is an established method to observe hiring trends in a variety of professions 8,9 and has been used for research in health care. 10,11 The research results can be used by organizations for strategic planning, by educators to target needed qualifications and competencies, and by researchers and policy advisors to assess progress toward value-based care.
Methods
Content analysis is a method of analyzing written communications or documents and consists of the 3 phases of preparation, organization, and reporting. 10 The goal is to reach a condensed but broad view of the research topic including descriptive analysis of categories. 10,12 Figure 1 outlines the steps followed for the content analysis process in this study, which were adapted from previous research. 10,12
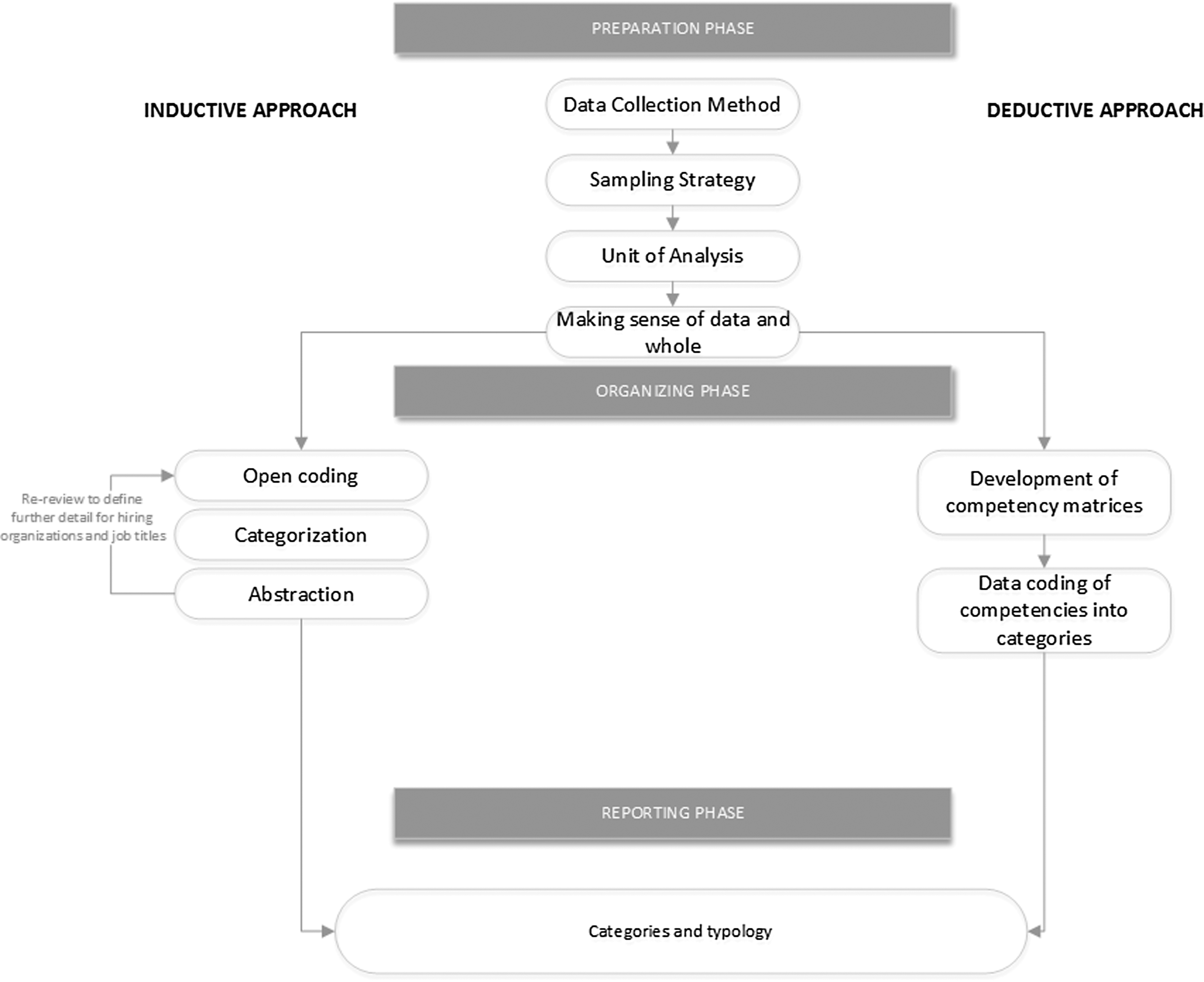
Content analysis process.
Preparation phase
The preparation phase included defining the data collection method, sampling strategy, and unit of analysis. 10,12
Data collection method
Job postings were collected for US health care positions during August-September 2016. Although job postings may actually have been posted prior to this time period, the posting continued to be active during the collection period. Each job posting consisted of semi-structured text and was copied into a separate document and saved with the job title and organization in the filename. Although there sometimes were section headings such as job description, qualifications, and required skills, headings varied significantly across the sample.
Sampling strategy
A convenience sample consisted of job postings for health care organizations such as health systems, physician practices, insurance companies, vendors, community organizations, and academia on
Unit analysis selection
The unit of analysis was an individual job posting. A review of the data was continually conducted to better understand the data and become familiar with the whole as well as the components of each job posting.
Organization phase
Both inductive and deductive approaches were used in this analysis. In an inductive content analysis, the concepts are generated from the data and thus adhere to the naturalistic paradigm. 11 The inductive approach was used in this study to capture core information about each posting and for categorization. Deductive content analysis is typically used to evaluate data in a new context or to test categories. 10 The deductive approach was used in this study to evaluate competencies required for selected job title classifications.
Inductive content analysis
Inductive content analysis includes open coding, categorization, and abstraction. 10 Open coding was completed by highlighting key parts of the document during the initial review and inserting comments via the word processing software. Meaning units or codes were identified for portions of the text. Descriptive headings were created to describe the content and possible categories were generated. Categories were recorded in a spreadsheet; each category was added as a column. Researchers have noted that the creation of categories is “a core feature of qualitative content analysis (p. 107).” 14 Categories help increase understanding of the research topic and generate knowledge. 15 Job postings were reviewed again and basic information abstracted such as job title, degree requirements, and years of experience. Abstraction depicts content at a higher logical level. 14 Job postings also were categorized as to whether the job was a clinical position, a management position, required technical skills, or specifically required population health experience. Job postings that required a nursing, pharmacy, or medical degree were classified as being clinical. Iterative reviews were conducted to identify classifications by type of hiring organization and job title.
Deductive content analysis
Deductive content analysis includes developing structured matrices and coding according to the matrix categories. 10 In the sample of job postings, positions were health care delivery centric and qualifications varied by position type (eg, job title classification). For this reason, competencies for the top 5 job title classifications were assessed based on domains identified by professional associations for the respective area and current research. Analyst positions were evaluated based on American Health Information Management Association's Certified Health Data Analyst domains. 16 Coordinator positions were evaluated based on the American Association of Medical Assistants occupational analysis of certified medical assistants (CMA) duties 17 and competencies required for the CMA exam. 18 Director positions were evaluated based on the American College of Healthcare Executives competencies. 19 Specialist positions were evaluated based on recent research on core competencies of program managers 20 and cross-checked with the Project Management Institute's program management domains. 21 Care manager positions were evaluated based on the National Academy of Certified Care Managers and Commission for Case Manager Certification exam domains. 22,23
A categorization matrix was developed based on the competencies by selected job title classification and data were coded based on the competency category. Competencies were coded based on required qualifications and a review of key responsibilities. An initial coding was completed for each of the 5 job title classifications to ensure competencies were holistically captured. Only qualifications that fit the competency categories were coded. Notations were made if there were any common competencies that did not seem to fit the defined list of competency categories. Recoding of each job title classification competency list was conducted again approximately 2 weeks after initial coding and any discrepancies were noted and reanalyzed.
Reporting phase
Descriptive statistics were completed for the overall sample as well as for specific subcategories. All data for each category were included in the frequency counts representing 100% of the sample. Frequency counts for job title classification subcategories also were generated to allow for more detailed analysis. Representative quotations were included for key responsibility areas for each of the top 5 job title classifications. A typology or systematic classification was developed based on the content analysis.
Trustworthiness
Trustworthiness is an important consideration in qualitative research. The content analysis process must be described in sufficient detail so that readers have a thorough understanding of the strengths and limitations of the study. 10 The concepts of credibility (eg, match between data analysis process and research focus), dependability (eg, data consistency), and transferability (eg, ability of findings to be transferred to other settings) have been used to describe various aspects of trustworthiness. 14 This study addresses these trustworthiness factors in the following ways. The unit of analysis, a job posting, was the most suitable given the research focus. Data analysis was conducted on specific items that addressed the research questions regarding population health management position qualifications and competencies. The categories selected reflected the research topic and sufficiently covered the data. Quotations on key responsibility areas of the top 5 job classifications were included for reference. Tables and figures were provided to show a direct link between the results of the study and the data. Finally, data were collected during a specific time period to ensure consistency and to address dependability.
Results
Descriptive statistics
A total of 271 job postings were identified during the specified time period. Descriptive statistics for the overall sample can be seen in Table 1. The sample included job postings from the following types of hiring organizations: health systems, physician practices, insurance companies, hospitals, vendors, community organizations, consulting, and recruiters, and the remainder in other (eg, retail pharmacy, post-acute care). The majority of positions required a bachelor degree and some required a master's degree. Specific degree areas included health care, nursing, or business administration depending on the focus of the position. A small number of positions required technical skills such as certification in information technology applications or database management and reporting. Job postings were distributed proportionally across the United States: the top 5 states based on the number of job postings were California, New York, Massachusetts, Maryland, and Pennsylvania.
GED, general equivalency diploma; IT, information technology; MD, doctor of medicine.
Clinical positions represented approximately 30% of the sample (Table 1). Clinical positions were typically nurses, care managers, or care coordinators in health systems. The majority of these positions required a bachelor degree (56.6%) with some requiring master-level degrees (10.8%). Years of experience ranged from 2 to 10, with 10 being an outlier. A small group of the clinical positions were for medical directors. These positions were at both health care provider organizations and insurance companies.
Approximately one third of the job postings were for staff management. The job title classifications for these positions included managers, directors, and executive positions (Table 1). Executive-level positions typically had the job title of Vice President, Population Health Management, or in 1 case, Chief Quality & Population Health Officer. Only 1 executive position required a clinical background. Executive jobs could be found at a range of hiring organizations including health systems, physician practice, consulting, and community organizations and typically required 7–10 years of experience.
Certain segments of job postings also were analyzed by type of hiring organization. For example, a small number of positions were found in academia. These positions were a mix of program director, faculty, postdoctoral, and administrator roles at academic institutions or associated research centers. Three positions were separately categorized as “research” because they were based at national research organizations. A broad range of positions were found at insurance companies; for example, analysts, care managers, program managers, operational leaders and medical directors. Physician practices had positions that were primarily care managers and coordinators.
Job title classification analysis
Profiles based on job title classifications were developed for the top 5 job categories: directors, coordinators, care managers, analysts, and specialists (Table 2).
Directors–“strategic leaders.”
Director-level positions (12.2%) included both operational leaders and program director roles responsible for specific initiatives. Some of these positions included being responsible for analytics as part of the population health operational leadership role. Typical job titles included the following: Director, Care Management & Population Health; Director, Population Health; Director, Population Health Analytics; and Director of Operations–Population Health. About a quarter of the director positions required a clinical background (24.2%). Hiring organizations included a mix of health systems, physician practices, community organizations, insurance companies, and other organizations. Years of experience required ranged from 3–15+, with the average being 5 years. Only 3 positions required technical skills. Top competencies were “knowledge of health care systems and organizations,” “leadership skills and behaviors,” “relationship management,” “communication skills,” and “general management” (Table 3). Examples of key responsibility areas were as follows:
EHR, electronic health record.
“Responsible for providing the oversight and direction for designing, implementing, and supporting a robust enterprise-wide population health management program, that is aligned with the Triple Aim of Better Health, Better Care, and Improved Cost.”
“Performs a key role in the development, implementation, coordination, and monitoring of clinical programs to support successful participation in Medicare Shared Saving Program, Medicare Advantage, MIPS, and commercial Value-Based care arrangements.”
“Works collaboratively with the Executive Team and physicians to provide strategic planning and implementation support for transition to Population Health Management.”
“Supervises, directs, and manages the Population Health Management care staff (eg, health coaches, analysts) that are responsible for the smooth deployment and standard operation of clinical programs and services which benefit the patient population.”
“Oversight of creating and expanding a PCMH model of primary care delivery.”
“Leads efforts to measure aspects of health care delivery germane to population health (eg, HEDIS, CMS ACO/GPRO, patient satisfaction, utilization metrics).”
“Uses clinical data to drive performance improvements and to build and evaluate effective interventions.”
Coordinators–“gap closers.”
Positions classified as coordinators (11.1%) were focused on coordinating some aspect of patient care. In many cases this was outreach related to care gaps or referrals, often in support of nursing staff. These positions were primarily found in health systems and physician practices (Table 2). Typical job titles were Population Health Care Coordinator or Population Health Program Coordinator. Almost half of the positions required a bachelor degree with about a quarter requiring high school only. Typically, 1 to 3 years of experience was required. Top competencies were “coordinate care and/or referrals,” “adapting communications/communication skills,” and “knowledge of clinical applications” (Table 3). Other skill areas that were frequently mentioned but not listed as part of competencies included collaborating with teams and conducting outreach. Examples of key responsibility areas were as follows:
“Manages panel of patients to ensure continuity of care, patient adherence to care plans, and identifications of barriers preventing adherence to care plan.”
“Provides outreach, education, and other needed activities to patients, referral sources, and the community.”
“Acts as a liaison between referral sources, facilities, and outside entities to prevent and/or resolve continuum of care issues.”
“Analyzes clinical data and identifies patients who have gaps in care and utilizes risk stratification intervention metrics for care coordination.”
Care managers–“patient managers.”
The category of care managers (11.1%) included both care managers and nurses, the primary difference being job title. These positions were focused on some aspect of providing care and quality improvement. Most of these positions required a bachelor degree as well as RN licensure (Table 2). Care managers primarily worked at health systems, hospitals, and physician practices. The top competencies were “coordinate care,” “assess client needs,” “analyze data,” and “quality/process improvement” (Table 3). Skills frequently mentioned in the job postings but not covered in the competencies included proficient computer skills, ability to use electronic health records (EHRs) and/or registries, and knowledge of medical record documentation requirements. Examples of key responsibility areas included the following:
“Ensures that inpatients experience an efficient transition from the hospital setting to the outpatient environment.”
“Designs and implements programs and processes throughout the continuum of care to ensure successful integration of strategic and quality improvement initiatives and goals clinic wide.”
“Responsible for providing interventions designed to ensure the coordination and continuity of care and services for at-risk patients with complex chronic medical, social, +/or behavioral or mental health illness over time.”
“Contributes to documentation of individualized care for identified patients, focusing on specific treatment goals. Assesses progress toward goals based on clinical judgment, review of patients' self-monitoring tools and trends in clinical data.”
Analysts–“analytic gurus.”
Analyst job postings (11.1%) were focused primarily on data analysis and often required some systems expertise. Typical job titles were Population Health Management Data Analyst and Population Health Analyst. About half of these positions required technical skills (Table 2). Positions were found across the spectrum of hiring organizations though primarily in health systems. The majority of these positions required a minimum of a bachelor degree and 3–5 years of experience. The top competencies were “analyze health data,” “generate reports,” “integrate data from multiple sources,” “conduct qualitative and quantitative analyses” and “provide recommendations to improve processes” (Table 3). Other skills that were frequently mentioned in the job postings but not specifically included in the competencies included expertise with SAS and/or SQL, project management, advanced Excel, and ability to use or program in MS Access. Examples of key responsibility areas were as follows:
“Use the claim data warehouse, population health tools, electronic health record, and other reporting systems to provide clinical and claims-related reporting and analytics.”
“Create models to forecast business variables and develop ad hoc analysis for senior management to assess current and historical trends and potential operational impact.”
“Develop and maintain quality dashboards to continually assess provider performance and identify improvement opportunities.”
Specialists–“domain experts.”
Specialist positions (8.8%) included the word “specialist” in the job title, which generally represented required knowledge in a specialized area such as population health program management, quality and process improvement, quality measures and reporting, or care processes. Typical job titles included Population Health Specialist, Population Health & Wellness Specialist, Population Health Performance Specialist, or Clinical Specialist, Population Health. Most of these positions were non-technical though in some cases skills related to the ability to use health information technology or EHRs were listed (Table 2). Most positions required a bachelor degree with some listing only high school graduation required. Two to 5 years of experience was typical. Top competencies were “communication skills,” “planning and organizational management,” “project and process management,” “teamwork,” and “stakeholder management” (Table 3). There were a number of skills that were prominent in the job postings that were not covered in the industry research competencies and these items included use of EHR including managing registries, analytics, quality improvement, knowledge of quality measures and reporting, and computer skills (Excel, Access). Examples of key responsibility areas were as follows:
“Triage clinical disease registries and prioritize coordination of patient's chronic care needs.”
“Work with patient registries and practice electronic health record to support quality reporting and monitoring of quality performance.”
“Report and monitor practice-level performance and implement improvement efforts related to overall quality and efficiency goals.”
“Work with various stakeholders at all levels of leadership within Medicaid and the community.”
A diagram of the overall categorizations (eg, typology) can be seen in Figure 2.
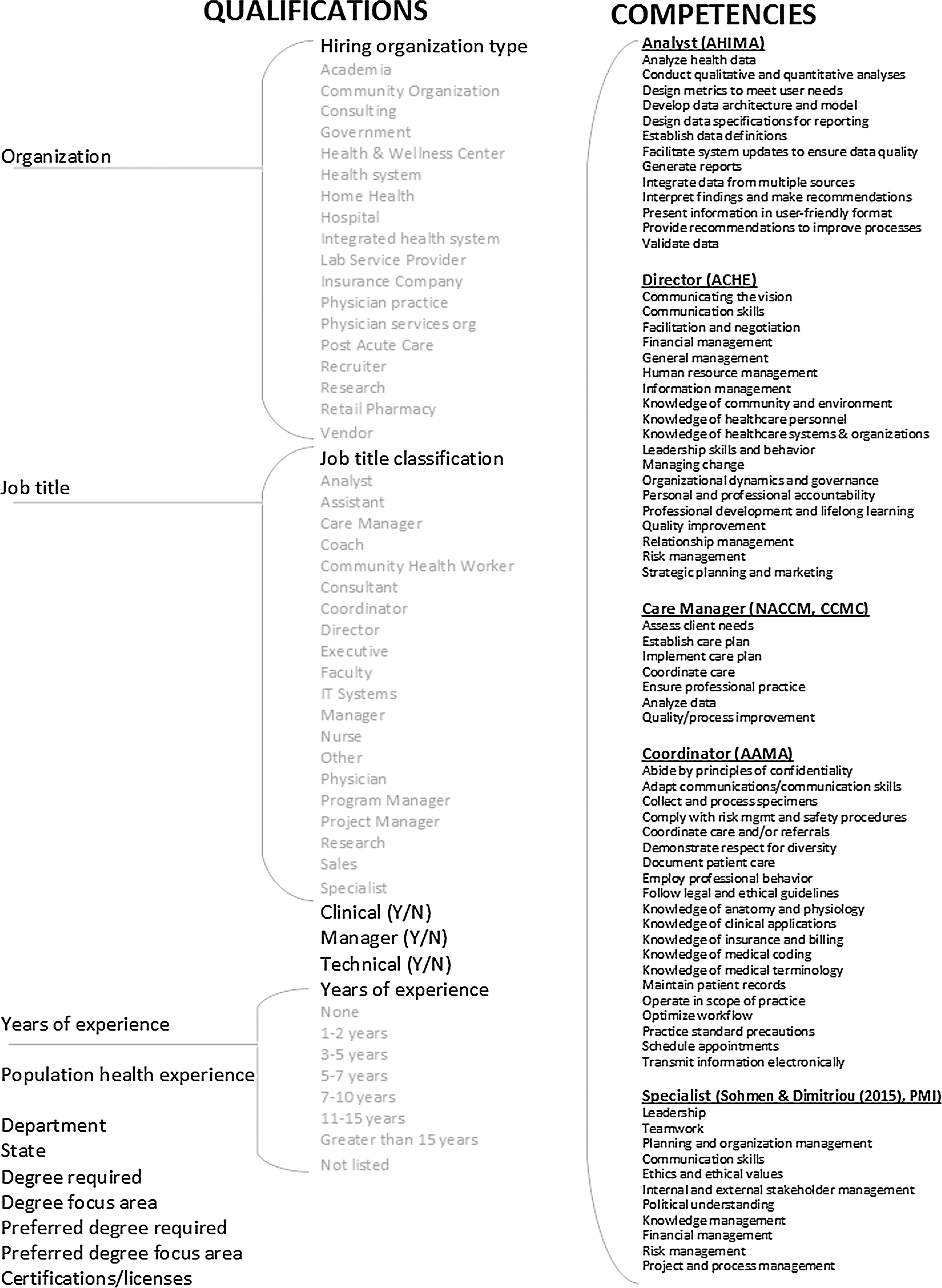
Typology.
Discussion
The purpose of this study was to analyze the types of population health management positions for which health care organizations are hiring, including the qualifications and competencies required for these positions. Population health management positions were primarily health care delivery-focused where patient populations were most commonly managed as part of an accountable care organization, value-based program, insurance plan, or other designated program. As social determinants were mentioned in only 11 job postings and health disparities or inequities mentioned in 5 job postings, there was limited evidence, based on this analysis, of efforts to address social circumstances and associated behaviors that are significant influencers of health.
Findings show that organizations are adding a broad range of positions in population health management; key job title classifications include directors, analysts, coordinators, care managers, and specialists. Many organizations are building out population health management teams resulting in multiple positions at different levels (ie, groups of positions) being added. Director-level positions represented the largest job grouping demonstrating the need for leadership of teams and new departments. At the same time, ensuring the seamless integration of functions with traditional organization positions requires population health management roles to have strong skills in communication, stakeholder engagement, and relationship building. The high demand for management positions and associated teams demonstrates strategic investment by health care organizations in the population health management function.
Clinical positions were targeted to build out a care management and coordination function to support population health management efforts. Primary positions in this grouping included nurses and care managers representing the continuing need for clinical skills and clinical support positions. Coordinator positions often were used to support nursing and care manager positions or specific programs, and included a mix of skills typical for CMAs. Within this context, coordinators tended to focus on closing gaps in care through outreach highlighting the importance of addressing care quality.
Population health management positions tended to be data-centric. Analytics expertise was frequently required in relation to patient population assessment and quality measure reporting including the need to understand various health data sources (eg, claims, EHRs). Analyst positions primarily supported this work. However, analytics skills also were represented in the specialist job grouping and, in some cases, the coordinator roles. Analytics expertise also was a requirement for many director positions, with some having population health analytics as a primary responsibility. Health care organizations increasingly are integrating analytics work into population health management positions and thus, demand professionals with qualifications in this area.
Population health management roles support a range of functions and thus require a blend of skill sets and the ability to work cross-functionally. This finding illuminates the challenge of finding applicants with the qualifications needed for population health management positions. Organizations recruiting for these roles will need to take a broader view and consider candidates with a variety of backgrounds and experience. Prioritizing top skills required and understanding what skills may be developed internally or through education will be critical to filling positions.
To meet market needs, academic institutions are hiring faculty, researchers, and related positions in population health management to support educational needs. Institutions educating health care workers must provide appropriate education and training to students to prepare them to be leaders in population health management in the value-based care environment. Higher education organizations are aware of this and are adapting and developing programs that address population health. 24,25 A move to increase more educational offerings in the population health management area is timely and a positive step to address market needs. As the market demands competent candidates who are equipped with specialized expertise in population health management as well as practical experience in program development, technology applications, care management, and analytics, professional education programs should provide hands-on experience via coursework, practicums, or internship programs. Furthermore, for core competencies represented in multiple job category areas such as use of EHRs and project management, new courses may need to be integrated into the broader health care curriculum.
This study had some limitations. The sample represented a snapshot in time and hiring trends and job requirements can change based on market conditions, limiting transferability. For these reasons, the results may not be generalizable. Additionally, content analysis coding is open to interpretation and can contain bias. To address this situation, coding was reviewed and validated multiple times. Analysis also was dependent on the content of job postings; some postings were missing key content areas (eg, required skills, years of experience), which may have impacted dependability. Finally, competencies were adapted from industry research and professional association roles that may not completely address competencies required for population health management positions given the diversity of positions and the fact that these positions are relatively new. For this reason, competencies may need further evaluation and refinement in the future.
Conclusion
This study highlights the investment health care organizations are making in population health management and the prominent role these positions are playing in health care organizations. The findings confirm that challenges and opportunities related to health care reform and new care models have motivated the development of new positions requiring specific expertise. The increased emphasis on population health management brings new demands for professional skills and experience, which must be met by enhancing professional development, training, and education. Required competencies will most likely evolve and need to be reevaluated periodically. Further study is needed to confirm findings and to monitor trends over time. By doing so, results can be compared to the current baseline data and progress assessed toward meeting organizational needs as well as industry progress toward supporting population health initiatives in the context of value-based care.
Footnotes
Author Disclosures
Dr. Meyer declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The author received no financial support for this article.