
Abstract
Social determinants of health (SDH) impact health outcomes. Medical centers have begun to collect SDH data, urged by government and scientific entities. Provider perspectives on collecting SDH are unknown. The aim is to understand differences in views and preferences according to provider characteristics. A cross-sectional survey of University of Miami clinical faculty was conducted in late 2016. The survey contained 11 questions: 8 demographic and departmental responsibilities questions and 3 Likert scale questions to capture collection and use of SDH perspectives. The main outcome was whether providers thought the benefit of collecting SDH outweighs the burden and risks. In all, 240 faculty members were included. The majority were men (64%), with a mean age of 51 years. Among participants, 53.5% were non-Hispanic white, 32% were Hispanic, 5% were Black/African American, and 5% were Asian. The majority agreed that SDH are important predictors of health outcomes and quality of care (83%). When comparing minority to nonminority faculty, 25% believed that SDH should only be available to PCPs, compared to 8% of nonminorities (P < 0.01). In a multivariate model, belonging to a racial ethnic minority was the only characteristic associated with believing that benefits of collecting SDH outweigh the risks (odds ratio 1.87, 95% confidence interval 1.02- 3.5) after adjusting for age, sex, minority status, health care provider type, type of responsibilities, and department. This study reveals that although most providers of a health system believe social risks impact health outcomes and quality metrics, the buy-in to collect SDH varies according to the racial/ethnic composition of the faculty.
Introduction
T
Many health systems are already taking steps to collect these SDH through a combination of strategies such as collecting data directly from patients, using publicly available data, or using geographic information systems to assign census-based variables. 14 –21
Early views on this transformation reveal that common concerns include the privacy and ethical considerations 22 linked to possessing social risk data with limited health system infrastructure and psychosocial skills 22 –24 to address them. An unintended consequence of such a setup could be the erosion of the patient–physician relationship.
Collecting social risk factors from entire health systems can have significant implications for those interested in precision medicine, particularly for those institutions seeking precision medicine initiatives to reduce health disparities. 25,26
Nevertheless, the perspectives and beliefs held by physicians caring for patients who may have social risk factors that affect their health and quality of life are not fully known.
This study aims to evaluate the beliefs that clinical faculty in a diverse medical school have regarding the role that SDH play in the outcomes of their patients, and to explore preferences regarding possible strategies that could be used to collect and address SDH at the health system. The study team also wants to explore if these perspectives vary according to provider demographic and professional characteristics. This information may facilitate the development of a realistic and sustainable approach for using SDH data for targeted care.
Methods
Study design and population
A cross-sectional survey (Supplementary Data; Supplementary Data are available online at
Survey
The study team created a Qualtrics (Qualtrics, Provo, UT) survey that collected information anonymously and sent the survey link via the medical school listserv. The link was sent 3 times to all active faculty members at the University of Miami Miller School of Medicine from September to November 2016. The survey contained a total of 11 questions. Eight descriptive questions included age, sex, race, ethnicity, primary appointment department, departmental responsibilities, and health care provider type. Census-based questions were used to ascertain race/ethnicity. 27 For departmental responsibilities, faculty members were allowed to pick clinical, research, administrative, academic, or any combination thereof. In terms of health care provider type, faculty members were asked if they considered themselves a primary care provider (PCP) or a specialist.
Additionally, the survey contained 3 questions to capture perspectives on the collection and use of SDH within the study health system. The first used a 5-point Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree) to ascertain faculty members' perspectives on SDH usefulness, ideal collection data process, party responsible for collection, access to SDH data, and integration into care flow. The second requested that faculty members select the 2 most common concerns regarding collecting SDH, including privacy and liability issues, not having the necessary infrastructure to address SDH, or not knowing how to interpret and use the data if collected. The third requested that faculty members rank the preferred strategies to operationalize the management of SDH by the health system. Options included training and education of personnel on how to interpret and use SDH, systemic processes that address the most common SDH, creation of targeted programs for those at risk, and development of a devoted team to lead the collection, interpretation, and operationalization of systems to address SDH.
Development of survey
A qualitative process was used to develop the survey questions. The study team reviewed the literature reporting concerns about integration of SDH in health systems 14,22 –24,28 and discussed the evidence to date with University of Miami faculty who lead population health efforts. Based on these discussions, the team created a road map of implementation 13 that included meetings with key stakeholders to evaluate the weight they assigned to previously reported priorities and concerns. Data from these structured interviews were used to identify domains of most interest, which later were used to inform the final questionnaire. Several stakeholders – including leadership, providers, and investigators – reviewed and provided feedback on questions in order to capture the data of interest. Stakeholders identified key risks of SDH collection as not having the infrastructure to address social risks, liability and privacy issues, overwhelming the health system operations, and lack of clarity on who should react to the data.
Definition of minority
In this study, those faculty members who self-reported as Hispanic, Black or African American, American Indian or Alaska Native, Asian, or Native Hawaiian or Pacific Islander were classified as minority while those who answered non-Hispanic and white were classified as nonminority.
Outcome
The main outcome was whether providers thought the benefit of collecting SDH outweighs the burden and risks. This was measured on a 5-point Likert scale (strongly agree to strongly disagree). The study team dichotomized this outcome into agreed versus not agreed categories. Agree and strongly agree were grouped into the agree category and strongly disagree, disagree, or neither disagree nor disagree were grouped into the did not agree category.
Statistical analyses
The study team compared baseline characteristics by minority status, sex, provider type, and department using chi-square and t tests if normally distributed or the Wilcoxon rank-sum test if not normally distributed. Logistic regression was used to identify faculty characteristics associated with believing the benefits of collecting SDH outweighs the risks. The multivariate model included age, sex, minority status, type of health care provider (primary care versus specialist), type of responsibilities (clinical versus research), and department.
Results
Baseline characteristics
Table 1 reports the baseline characteristics of the 240 faculty members who responded to the survey. The general response rate was 18%. The response rate by department was medicine 30%, surgery and surgical specialties 15%, pediatrics 22%, OB/GYN 32%, psychiatry 14%, and physical medicine and rehabilitation 10%.
The majority of the faculty were men (64%), and the mean age of all participants was 51 years. Among participants, 53.5% were non-Hispanic white, 32% were Hispanic, 5% were Black or African American, and 5% were Asian. More than half of the faculty had primarily clinical responsibilities with no research effort and the balance reported research responsibilities. Half of nonminorities had research responsibilities compared to 40% of minority faculty (P = 0.16). More than 80% of the faculty were specialists, and 13% were PCPs. In all, 61% were from the medical department
Benefits of collecting SDH outweighs risks
When evaluating the perspectives of clinical faculty regarding the statement that the benefits of collecting SDH outweigh the risk, it was found that 16% strongly agreed, 42% agreed, 29% neither agreed nor disagreed, 8% disagreed and 4% strongly disagreed.
Other SDH perspectives
Figure 1 shows the dichotomized perspectives on collection and use of SDH among the faculty who responded to the survey. The majority of participants agreed that SDH are important predictors of health outcomes and quality of care (83%), that collecting SDH would improve comprehension of predictors of quality metrics (80%), and that it is crucial for the development of special programs (85%) for at-risk populations. Although 73% agreed that it should be available in the EHR to all providers and not only PCPs, slightly more than 54% thought the PCP should be the one responsible for managing social risk factors and 65% agreed a dedicated population health team should exist to assist in these efforts. Seventy-two percent agreed that collection of SDH would put additional burden on providers, but 58% thought the benefit outweighs this burden. Seventy-one percent of faculty agreed that clinics were not set up to address SDH at this time.
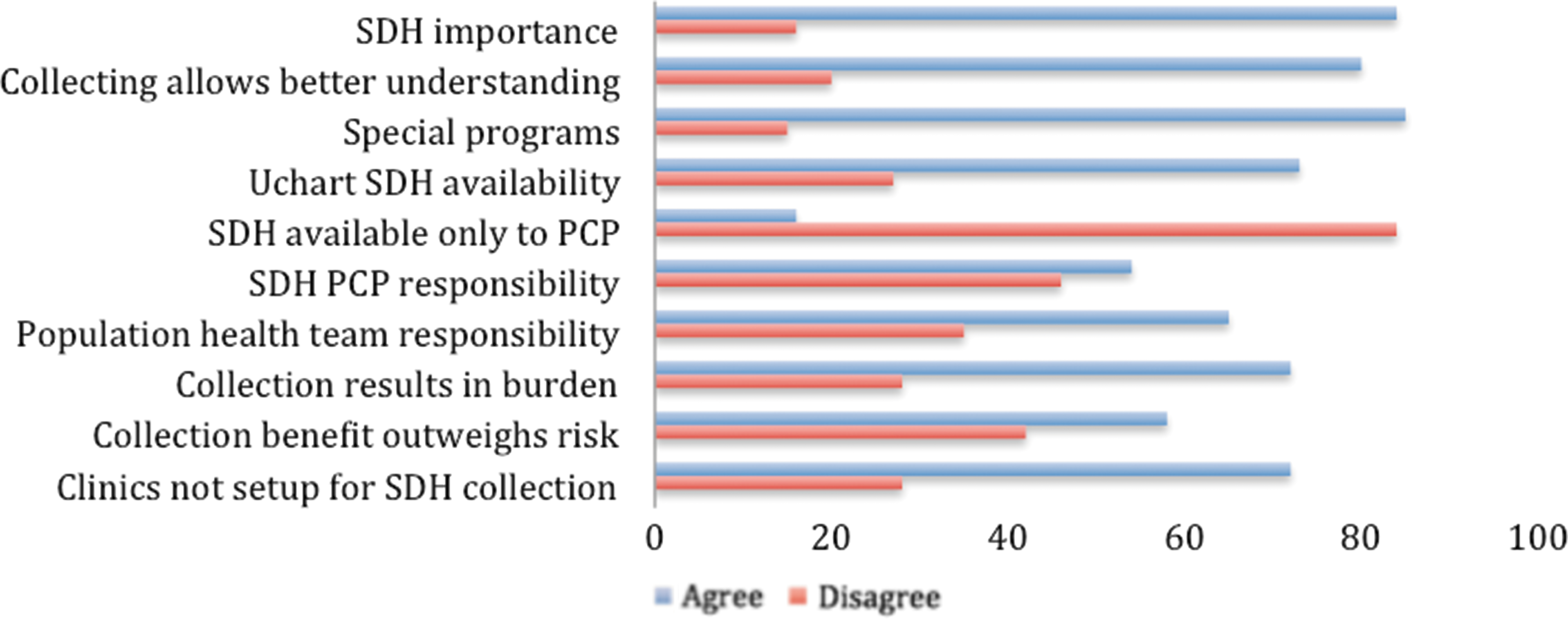
Overall perspectives of collection and use of social determinants of health. Based on faculty members who agree with statement. PCP, primary care provider; SDH, social determinants of health.
Perspectives of faculty subpopulations
When comparing minority to nonminority faculty, Figure 2 shows that more minorities (66%) agreed that the benefit of SDH collection outweighs the burdens and risks (P = 0.02) when compared to nonminorities (51%).
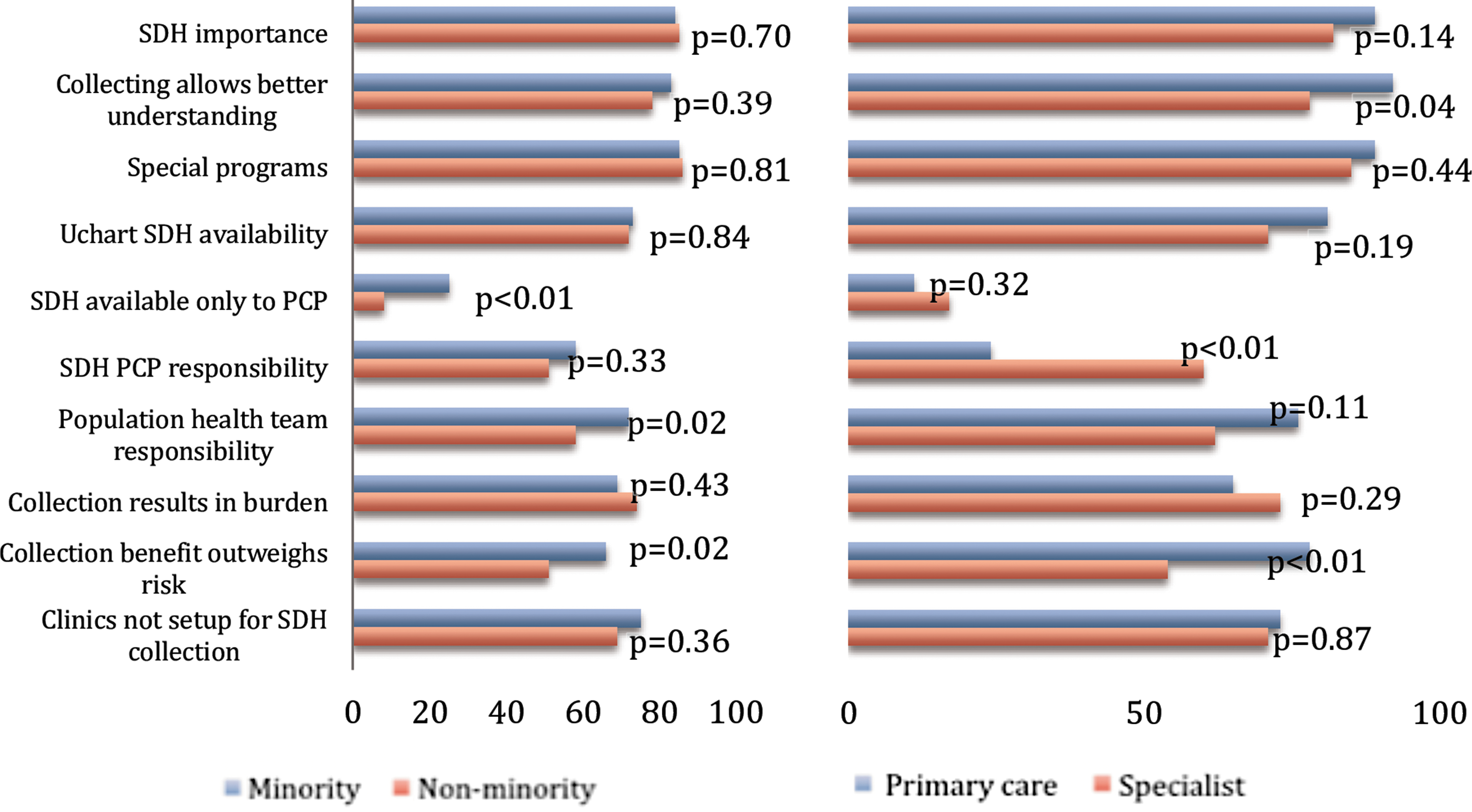
Collection and use of social determinants of health perspectives by minority status (left panel) and provider type (right panel). Based on faculty members who agree with statement. PCP, primary care provider; SDH, social determinants of health.
In addition, more minorities (72%) agreed that a population health team should be at the forefront of the effort (P = 0.02) compared to nonminorities (58%), and although not a common belief, more minorities (25%) agreed that SDH should only be available to PCPs compared to 8% of nonminorities (P < 0.01).
Additionally, differences were seen between PCPs' and specialists' perspectives (Fig. 2). More PCPs (78%) than specialists (54%) agreed that the benefits would outweigh the burden and risks (P < 0.01). A greater number of PCPs (92%) than specialists (78%) believed that SDH collection would allow for a better understanding of quality health metrics (P = 0.04). When questioned about whether PCPs should be solely responsible for addressing SDH, more specialists than PCPs agreed (P < 0.01). When comparing faculty members from different departments, similar perspectives were found throughout. However, more surgical departmental faculty (72%) than nonsurgical (47%) agreed that PCPs should be responsible for addressing SDH (P < 0.01).
When comparing perspectives by sex, a greater number of females (91%) compared to males (82%) agreed that SDH collection would allow for the creation of special programs for at-risk populations (P = 0.05), and more females (81%) than males (68%) agreed that SDH information should be included in the EHR (P = 0.02).
Multivariate model
In a multivariate model, belonging to a racial ethnic minority was the only faculty characteristic associated with agreeing that the benefits of collecting SDH in the EHR outweigh the risks (odds ratio 1.87, 95% confidence interval 1.02- 3.5) after adjusting for age, sex, type of health care provider, type of responsibilities, and department.
Concerns about collecting SDH and integration strategies
When faculty members were asked to identify the 2 most important concerns they have regarding SDH collection, 44% identified not having the clinic or health system infrastructure to address SDH issues, and 24% selected not knowing how to use SDH information to benefit patients. However, these views differed slightly by minority and specialty status (Fig. 3). Among minority faculty and primary care physicians, the second most common concern was liability related to not addressing a risk leading to an adverse outcome (eg, failure to address a positive depression or domestic violence screening), whereas for nonminority faculty and specialists, it was not knowing how to use SDH data once they are available.
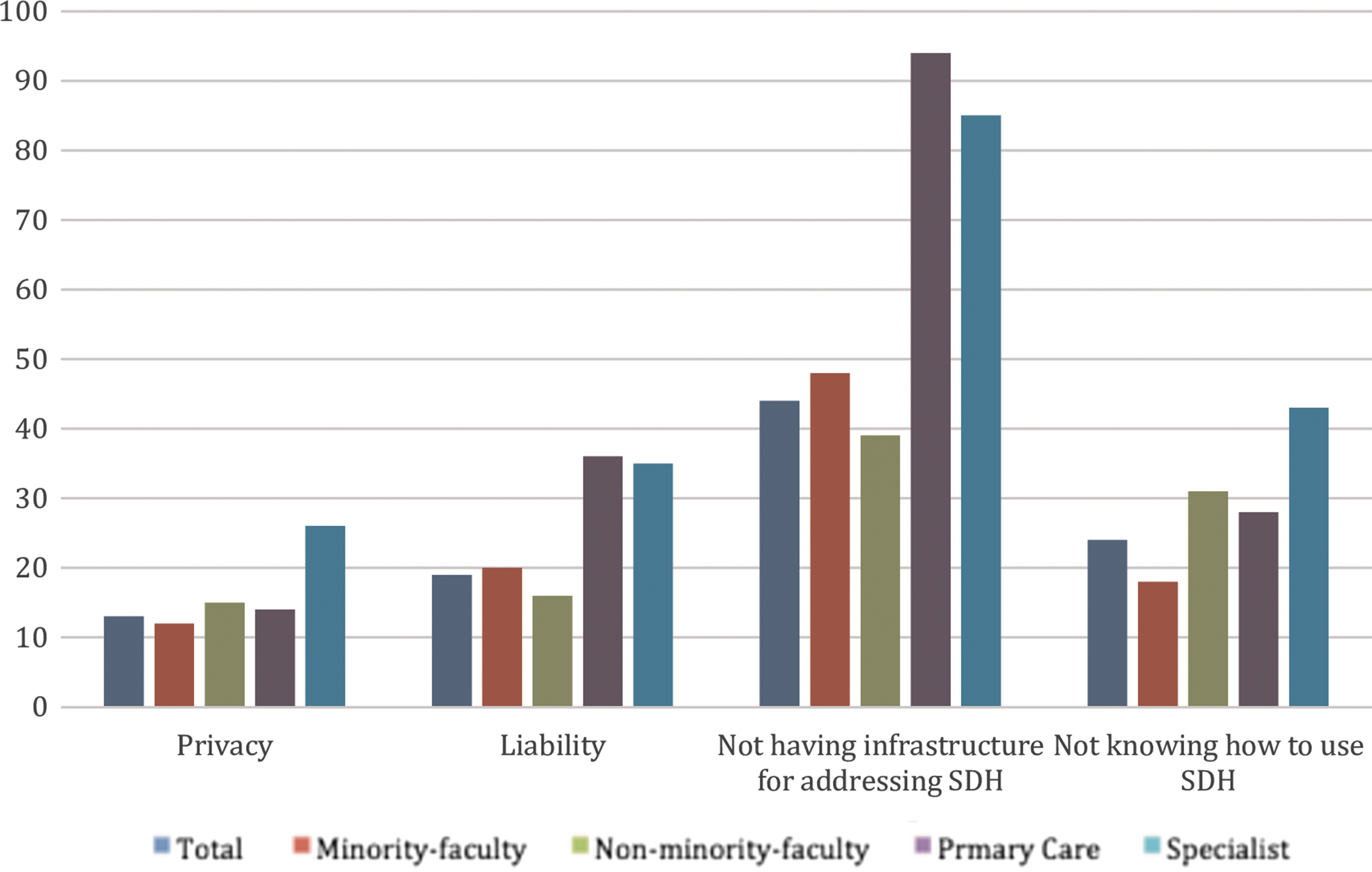
Most frequent concerns by minority and specialty status. SDH, social determinants of health.
When asked to rank the most important strategies to use SDH data for improving quality of care, the most common strategy cited by all faculty was having a dedicated team to analyze and report the SDH data to facilitate supporting services (32%). Figure 4 shows these preferences in the overall group and by minority and nonminority faculty. The second most frequently chosen strategy among all responders was implementing systemic processes to address the SDH across the health system (27%). This result was driven mostly by the fact that 35% of nonminority faculty and specialists selected this strategy as a first choice. The second most common strategy among minorities was training and education of personnel regarding how to interpret and address SDH (29%).
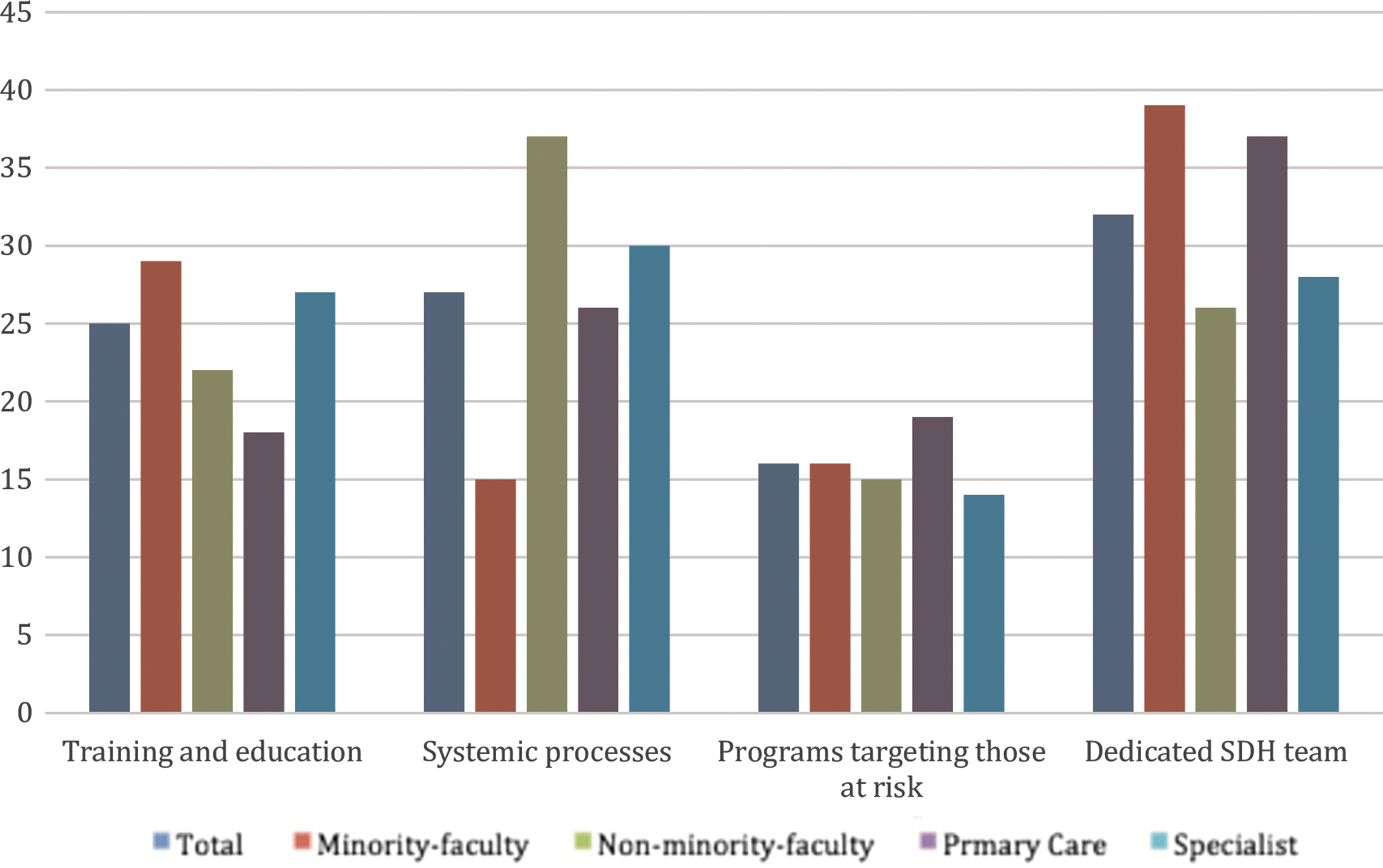
Preferred strategies to address social determinants of health by minority and specialty status. SDH, social determinants of health.
Discussion
This study, conducted in a large academic health system in Florida, found that the majority of clinical faculty believe in the importance of SDH in health outcomes and quality metrics. However, only half of providers believe the benefits of collecting SDH data outweigh the risks. The most common concerns were the lack of infrastructure to address SDH and the lack of adequate knowledge to use this information effectively. Interestingly, there were differences in these perspectives according to faculty characteristics. Faculty who self-identified as minorities were more likely to believe that the benefits of collecting SDH outweigh the risks when compared to nonminorities, and were less likely to cite lack of knowledge as a barrier. Additionally, more specialists and surgical department faculty members thought that PCPs should be responsible for addressing SDH when compared to PCPs and nonsurgical departments. The most accepted strategy to operationalize the integration of SDH in the health system, across departments and specialties, was having a dedicated team to address the social risk factors of the population served.
To the study team's knowledge, this is the first reported evaluation of the perspectives of clinical faculty members of a health system on the collection of SDH for operational purposes. A strength of this study is that it was conducted in a large academic center with significant racial/ethnic and professional diversity, which allowed for the comparison of faculty according to a variety of faculty characteristics.
This study has several limitations that deserve mention. First, the response rate was 18%, which could lead to selection bias. To better understand this risk, the study team evaluated participation by sex and by department, and found that the sample was representative of the distribution of the sexes. However, the team did find overrepresentation of minority faculty, primary care, and faculty with both clinical and research responsibilities. Overall, medicine departmental faculty participation was according to the University of Miami Miller School of Medicine faculty distribution. However, all other departments, including pediatrics, OB/GYN, psychiatry, and physical medicine and rehabilitation, were overrepresented, except for surgery and surgical specialties, which were underrepresented in survey participation. For this reason, the study team conducted stratified analysis by these characteristics.
Second, this was a single center study, limiting the generalizability of the results to other geographical areas or clinical settings. Multicenter, geographically diverse studies would help better define how health systems view the collection of SDH across the United States. Nevertheless, based on present study results, perspectives regarding the value of collecting SDH will vary according to the composition of the faculty and the population they serve. Hence, for quality improvement purposes, each health system should collect and interpret its own data.
Third, although the study team collected overall perspectives on strategies to integrate SDH into the EHR, the team did not collect specific information regarding logistic processes that could be used to collect SDH in particular settings or what SDH data should be prioritized or excluded. Finally, the team did not test the reliability of the survey instrument but plans to do so in the future.
This study aimed to elucidate views regarding utility of using SDH, concerns, and preferred strategies to move forward. Evidence suggests that Medicaid enrollees receiving care in managed care clinics screening for SDH had significantly higher use of PCP services and fewer emergency department visits, hospitalizations, and drug use. 29 Thus, managed care organizations estimated a 4:1 return on investment. 29 However, several reports exist on patient-, physician-, health system-, and policy-level concerns about screening for SDH. At the patient level, the individual may feel discomfort when reporting his or her information regarding social and economic needs. 14 There is potential for unintended harm if the patient has expectations regarding his or her SDH screening. 22 Additionally, there may be legal or ethical concerns in screening for a condition (eg, depression, domestic violence) without a clearly defined infrastructure to address it effectively. 22 In this study, the legal or ethical considerations were less commonly cited than the overall concern of not having the proper infrastructure to address SDH, which was the most common concern. This, as well as a lack of physician time or communication skills regarding SDH, 22 –24 has been reported previously.
Interestingly, the study health system had developed a multistakeholder process to implement the collection and use of SDH, 13 with the purpose of selecting social risks that can be addressed and identifying the resources that need to be in place to care for them. This highlights the fact that even though providers did not rank education or training as a top priority, putting in place strategies to keep the members of large health systems informed of new initiatives, new infrastructure, and resources, and how to access them, may facilitate the acceptance of SDH collection efforts. Additional barriers cited by others at the provider level are challenges entering diagnoses codes into EHRs for specifically identified SDH. 28 Unfortunately, no information was collected on this subject, as it was not considered a relevant domain during the survey generation process.
Nevertheless, this study contributes important information regarding the most common perspectives among physicians, as well as the differences seen across a diverse academic health system. The study revealed that developing infrastructure to address SDH is a key factor for all faculty, but also found several differences according to age, sex, race/ethnicity, and provider type. Interestingly, the adjusted model suggests that self-reported faculty race/ethnicity is the main driver of believing that the benefits of collecting SDH outweigh the risks. Although speculative, a potential explanation is that minority faculty could have been more exposed to the effects of social risks throughout their life experience.
These differences in perspective could increase in relevance as the diversity of a health system diminishes, because it could limit the buy-in for SDH collection or influence the preferred strategies to respond to social risks.
Of note, although most faculty members believe that social risk information should be available in the EHR, specialists are more likely to believe it is the role of the PCP to address the risks identified. This is an important insight because many large health centers, such as the one in this study, provide a large proportion of tertiary care services for cardiovascular, oncological, neurosurgical, and many other conditions that can be severely impacted by SDH. 30 –32 Although these health systems will be evaluated on those outcomes, the PCP most likely is part of another network, limiting the ability to influence social risk through primary care. Thus, the idea of having a population health team identifying patients at risk and assigning potential interventions seems to be a reasonable approach for certain populations at risk of severe or costly outcomes.
Others have reported strategies to mitigate logistical barriers associated with collecting SDH. These include: utilizing computer-based self-completed questionnaires, which are cost and resource effective 14,23 ; the use of community health workers to screen patients, because they have established relationships and trust with patients 17,18 ; providing physicians with SDH tool kits 20,33 ; and changing the EHR format and diagnoses codes to diminish provider burden. 28,34 Health systems can empower providers with resources to address SDH by making sure that there are established referrals and resource information that physicians can give. 22,23 They can provide electronic referrals to community agencies while coordinating with community resources. 22,23 The government can incentivize the collection of SDH in the EHR by matching the health care demographic data collection requirements to public health requirements 35 or allowing for reimbursement of EHR diagnoses and billing codes related to SDH-specific procedures. 28 However, among centers that have implemented the collection of SDH screening tools, the most important strategies cited have been the need to establish strong organizational support and increasing stakeholder buy-in. 33 The present study findings also suggest that understanding the perspectives of the health system personnel on SDH collection is key for a successful process.
In 2016, the US Department of Health and Human Services recommended to Congress to acknowledge and incentivize health systems serving the vulnerable in order to avoid any possible exclusion of these groups from health systems attempting to improve performance. 2 Moreover, using social risk data may allow health systems to test whether the provision of precision medicine leads to better outcomes and reduction of health disparities. 25 Hence, health systems should become active stakeholders and advocates for those exposed to the highest social risks. In order to make informed decisions and to interact with government agencies, health systems should understand their own providers' perspectives on SDH, generate consensus on what, how, and who would collect and address SDH, and propose incentive models that may mitigate the barriers they are facing.
In conclusion, this study reveals that although most providers of a health system believe social risks impact health outcomes and quality metrics, the buy-in to collect SDH varies according to the perception of health system preparedness and by the racial/ethnic composition of the faculty. Future studies should evaluate the effectiveness of concrete strategies to increase the preparedness, faculty buy-in and, ultimately, the use of SDH for clinical purposes.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The research reported in this publication was conducted under the auspices of the Precision Medicine and Health Disparities Collaborative (Vanderbilt-Meharry-Miami Center of Excellence in Precision Medicine and Population Health), supported by the National Institute on Minority Health and Health Disparities and the National Human Genome Research Institute of the National Institutes of Health under award number U54MD010722.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.