
Abstract
Five percent of Medicaid patients account for 50% of total costs. Preventable costs are often incurred by patients with complex medical, behavioral, and social needs who disproportionately utilize acute care services. Evidence for design, implementation, and evaluation of complex care programs in the urban Medicaid population is lacking. The article provides a description of a complex care program (CCP), challenges, and early outcomes based on a pre–post evaluation. The CCP was located within an existing urban medical home. Patients were eligible if they lived within 10 miles of the clinic and had at least 2 inpatient visits and/or 3 emergency room visits within the prior 6 months. Ambulatory Care Groups® were used to predict estimated total costs of patients, who were included if potential cost savings exceeded $5000. Patient experience and quality of care were assessed using validated measures and costs. Return on investment was calculated based on investment and cost savings. Costs include visits (clinic, specialty, and emergency room), hospital admissions, medications, tests and services, as well as salary and benefits of clinical staff. Eighty-six of 211 eligible patients (41%) were enrolled during the first 18 months of the pilot program. There were positive trends in quality metrics and patient satisfaction. The pre–post evaluation demonstrated a reduction in emergency room visits and hospitalizations (67% and 65%, respectively), which resulted in a 2.2:1 return on investment. This article offers lessons learned to colleagues considering population health approaches in the care of high-risk Medicaid patients.
Background
H
Innovative approaches are needed to support HNHC patients, who incur excess costs through complications of chronic illness or avoidable emergency room or inpatient utilization. 4 –9 During the last decade, numerous “complex care” programs addressing the needs of HNHC patients have been developed and evaluated. 4 –6,8 –24 Successful programs incorporate connections with patients and families, provide access and coordination of care, and support care transitions. They maintain reasonable clinician workload and increased visit times. They also employ data and analytics to target patients who are most likely to benefit, and monitor outcomes. Although some programs provide external case management services to complement existing primary care, most successful programs provide these services as part of direct patient care programs. 11 –24 A recent systematic review found mixed effectiveness on reducing outcomes such as mortality and hospitalizations; these studies included predominately elderly, nonwhite females. 24
The Medicaid population has unique challenges including housing instability, food insecurity, and psychosocial needs. 22 Evidence shows that addressing social determinants such as housing and food may reduce medical expenditures. 25 –27 In addition, because of the prevalence of substance abuse and mental illness in Medicaid beneficiaries, access to behavioral health services also is critical. 28 –32
Questions remain about how to translate these principles into practice. Gaps in knowledge, sustainability, and achievement of program goals have resulted in calls for ongoing study and experimentation with program design and supporting partnerships and policies. 5,18,24 In socially complex Medicaid populations, strategies to increase patient engagement and retention are needed. 4,12,13,22
The study team recently implemented a new complex care program (CCP) targeting Medicaid HNHC patients within an existing urban medical home (UMH) practice. This preliminary study sought to (1) develop a referral, retention, and transition framework, (2) characterize patients and their care needs, (3) pilot new analytics, (4) test staffing models, and (5) demonstrate feasibility of value-based care collaboration between a payer and provider group. While analysis is under way, the team presents some preliminary quality and cost outcomes from the first 18 months that have supported continuation of this program.
Methods
The study team developed a comprehensive CCP for Medicaid patients and launched this as a pilot in Baltimore, MD, a city that reflects disparities realized across the United States. The pilot was jointly sponsored by a large, regional medical group practice and a payer group that administered a Medicaid Managed Care Organization (MCO). Both were part of a large integrated academic health system. The health system used an electronic health record (EHR) with centralized data management and decision support, and the state offered a regional health information exchange system to link non–system hospitals and providers.
Key elements of the complex care delivery model
The CCP was developed as a separate service center within an existing UMH that provided care to a panel of 6500 adult patients. This practice identified more than 200 patients who were high utilizers despite ongoing efforts within the UMH. To focus resources on these more complex patients, the new CCP was designed to increase access, care coordination, continuity, and comprehensiveness of care, while providing social and behavioral services within the care team. Figure 1 depicts the conceptual framework of the complex care model. Patients transition back to standard primary care when individualized targets, such as disease control, utilization, and self-management skills (eg, schedule and attend appointments, request medication refills) are achieved. 33

Conceptual framework of the complex care program, Priority Access Primary Care. ER, emergency room; LCPC, licensed clinical professional counselor; PAPC, Priority Access Primary Care.
Payer–provider partnership
The Medicaid MCO and provider group entered into a 2-year agreement in November 2014. The payer allocated half of the grant up front, with the remainder contingent on meeting program metrics and milestones in year 2. The provider group also billed fee for service for patient care. Cost savings realized during the pilot phase went solely to the MCO, as it was the risk-bearing organization. Bidirectional data exchange between the clinical team and the payer was developed to identify patients and to monitor the program. The MCO provided claims data to determine patient eligibility and conducted quarterly pre–post claims utilization analysis. The provider group reported monthly on outreach, enrollment, and real-time utilization.
Clinical staff
The CCP clinical team consisted of 5 core team members: a community health worker (CHW) for connection to social services and to assist with outreach to new patients, a licensed clinical professional counselor (LCPC) for therapy and connection to mental health services, an office-based certified medical assistant (CMA) who served as a “health navigator” with both clinical and administrative duties, and a certified registered nurse practitioner (CRNP). The team was led by a doctor of medicine (MD) medical director who, together with the CRNP, provided primary care. All staff worked together in 1 office. The team participated in daily work rounds, weekly summary rounds, and monthly meetings included leadership and payer representatives.
Primary care delivery
The clinic held office hours between 8
Behavioral health services
All team members were trained in motivational interviewing and trauma-informed care, while the LCPC led behavioral health services and coordinated care with community mental health providers. All patients received baseline screenings for depression (Patient Health Questionnaire-9), anxiety (Generalized Anxiety Disorder-7), trauma (Posttraumatic Stress Disorder Symptom Scale), and substance abuse. Patients participated in regular counseling and engaged in art therapy within the clinic (Fig. 2). The MD on the team was certified to prescribe buprenorphine for opiate misuse disorders. Patients were referred to higher level behavioral health services, such as intensive outpatient programs or residential treatment programs, when needed.
Art therapy in complex care program.
Social services
The team's CHW coordinated social services and social needs screening. Screening included baseline and periodic assessment of barriers to care, such as food access, legal aid, child care, social security income, transportation, utilities, and housing. The CHW also accompanied patients on visits to social services agencies as needed. The program provided vouchers for taxi services to medical appointments until public transportation access was secured, and waived co-pays for formulary medications.
Care management
To address preventive care and chronic illnesses in the population, the CCP provided a team-based approach to assuring delivery of general preventive services and disease-specific care, assisted by decision-support tools built into the EHR. The entire team assisted with care coordination and care management. In addition to traditional care management roles of reminding patients of appointments and coordinating care, on admission to the program, patients developed a treatment plan in conjunction with the team's LCPC. The treatment plan identified medical, behavioral, and social goals, and was used to prioritize complex health needs and improve patient engagement by focusing on goals that are most important to the patient. The treatment plan was reassessed every 3–6 months.
Program monitoring and evaluation
Program metrics were developed to monitor program implementation in 3 areas: (1) patient characteristics, experience, and activation, (2) quality of care, and (3) utilization. A dashboard of key metrics was developed and monitored during the pilot to assist ongoing program improvement and process monitoring.
Patient metrics
Patient satisfaction was measured by the Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CGCAHPS) survey methodology. Patient engagement was assessed every 3 months using the Patient Activation Measure (PAM) tool, a validated assessment of the patient's interest and ability to engage in improving their own health. 34 Medication adherence was assessed with the Medication Adherence Questionnaire (MAQ-8) every 3 months, and the patient's experience of care delivery was measured with the Patient Assessment of Care for Chronic Conditions (PACIC) survey every 6 months. 35 Data from these validated assessments informed the program evaluation and were used during team meetings to guide education and interventions.
Quality metrics
Quality of care was evaluated in several areas, focusing on value-based purchasing incentives identified by the state and payer. Although numerous metrics were monitored by the larger group practice, the metrics of most interest in this Medicaid population included breast cancer screening, cervical cancer screening, diabetic eye examination, and controlling high blood pressure.
Utilization metrics
The number of hospitalization and emergency room visits were determined at a year's baseline prior to entering the program (to account for seasonal variability), and compared to after starting the program. Utilization metrics included costs of clinic, specialty, and emergency room visits, hospital admissions, as well as medications and testing services. Investment included salary and benefits of team members, along with costs of practice incurred. Return on investment for the program was calculated quarterly.
Patient eligibility
The payer and program leadership developed eligibility criteria based on demographics, utilization, complexity, and potential savings. Patients were eligible if they lived within 10 miles of the clinic and were “high utilizers” (≥2 inpatient visits and/or ≥3 emergency room visits; 1 standard deviation above the mean) or “super-utilizers” (≥3 inpatient visits and/or ≥9 emergency room visits; 2 standard deviations above the mean). Complexity and potential savings were modeled using Ambulatory Care Groups to predict patients' estimated total costs. This was compared to actual costs and patients with a potential cost savings ≥$5000 met the inclusion criteria. Patients were excluded if they had active cancer or predominately pregnancy-related utilization. Only MCO members were eligible for this pilot.
Identification and enrollment
Patients meeting eligibility criteria were identified by the payer and referred to the CCP team. Providers and staff from the UMH and other local practices also could refer patients to the CCP. Regardless of referral source, patients were reviewed by the CCP medical director to assure they met standard criteria and were appropriate candidates for the program. Eligible patients were approached by primary care providers and a CHW. To further aid enrollment, the MCO contracted a call company. Interested patients completed a secondary interview explaining the program goals of improved health and self-management. Participants signed an agreement upon enrollment to set the expectations of their role, and to agree to the additional payer benefits.
Analysis
Patients were included in the quality analyses if they had maintained membership in the CCP for at least 6 months. Quality outcomes employed a matched cohort in the UMH practice. Significance was determined using z-statistics. Preliminary hospital and emergency room utilization were based on pre- and post-enrollment data, and percent change was calculated. Monthly expenditures were calculated for each month's enrollment cohort and compared to costs prior to enrollment for the same duration. The Medicaid MCO's program investment was then used to calculate return on investment. This program was approved by the Johns Hopkins Medicine Institutional Review Board.
Results
The 18-month pilot began in November 2014. Despite preprogram planning, the program underwent iterative change as problems were identified and solved. The high acuity of patients in this population and challenges in understanding and implementing this new care model led to staff turnover such that only 1 of 5 starting staff, the medical director, remained with the program through the pilot phase. Ultimately, clinical staff best suited for this work were identified for program operations.
Recruitment and enrollment
Overall, 211 patients were identified as eligible and 86 (41%) eligible patients were enrolled during the pilot (Fig. 3). Multiple modalities were employed to recruit and enroll patients. Direct outreach by CCP providers yielded 38 (44%) enrollees, whereas 21 (24%) were recruited by the call company, 14 (16%) by direct outreach from a CHW, and 13 (15%) from community primary care providers. Among 191 patients identified by the payer, 70 (37%) enrolled, 45 (24%) could not be reached, and the remainder declined the program or failed to show after multiple scheduling attempts. A total of 78 patients were referred from providers from the UMH or surrounding practices: 20 (26%) were eligible, and 16 (80%) eligible patients were enrolled.
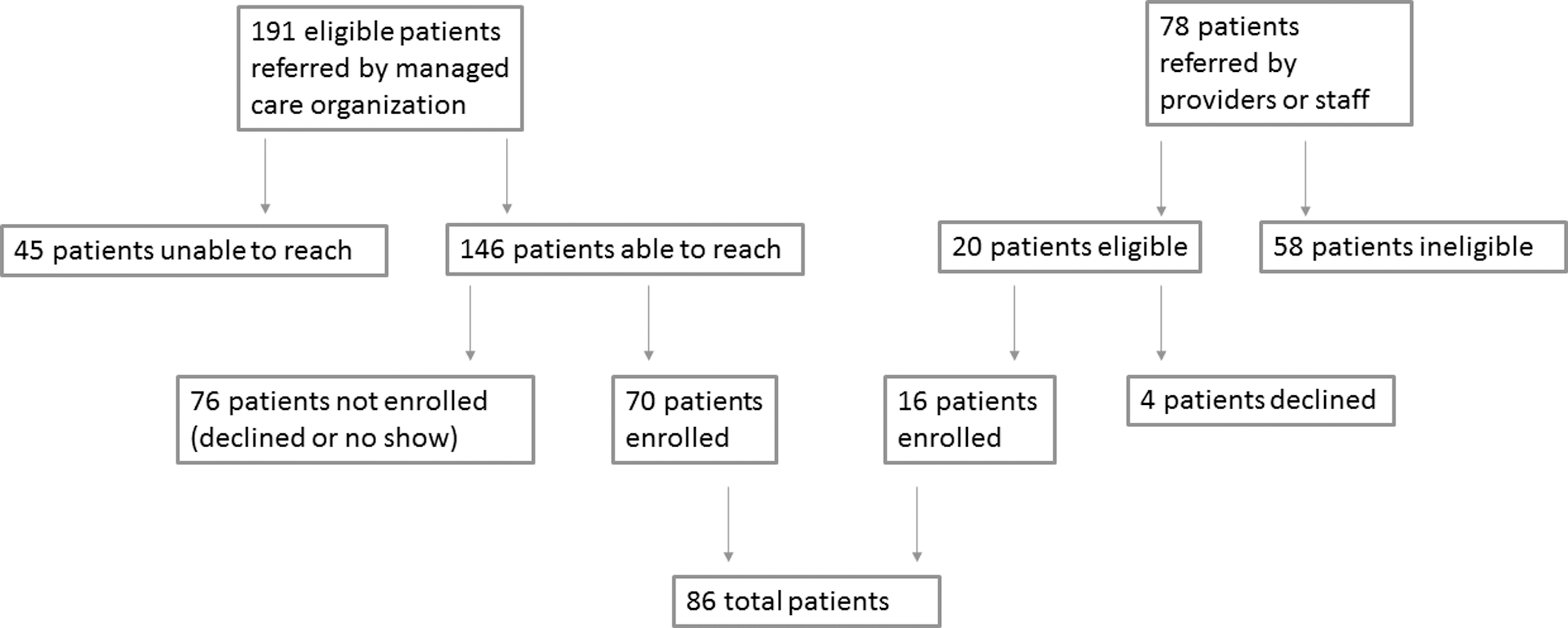
Flow diagram for complex care program patient recruitment and enrollment during the first 18 months of the pilot phase.
Program management
Once enrolled, the average participant remained in the program for 8 months. During the first 18 months of the pilot, the average census was 40 patients, with a maximum enrollment of 69 patients for this 5-person team. A total of 23 patients have been discharged: 11 changed insurance or moved out of state, 5 failed to engage because of substance use disorders, 3 were transitioned successfully to their previous primary care provider, and 4 were deceased. Most visits were face-to-face interactions in the clinic (76%); the remainder took place in the patient's home, at specialist appointments, or in acute care settings. Telephone encounters were used to assist with follow-up and appointment reminders. On average, there were 3 after-hours calls per day.
Population and patient characteristics
Baseline clinical characteristics of the patients compared to the surrounding UMH are shown in Table 1. Among 86 patients cared for, average age at enrollment is 44.5 years, and more than 60% are female. The majority of patients are African American. On average, patients are faced with 7.1 chronic medical and/or behavioral health conditions. Nearly all patients (97%) had at least 1 behavioral health (mental illness or substance abuse) condition. All patients had low incomes, and common social needs included inadequate access to transportation, low health literacy, food insecurity, unstable housing, and difficulty paying for utilities (Table 1).
No data available.
ACG, Ambulatory Care Group; MCO, managed care organization; SD, standard deviation.
Patient metrics
The PAM survey was completed at least once by 72 (84%) patients, with an average activation level of 3 and a mean score of 60.8. The medication adherence survey was completed by 67 (78%) patients and the results showed that 66% reported low adherence, 25% medium adherence, and the remainder high adherence. The PACIC survey was completed by 67 (78%) patients with an average score of 4.2/5.0. A CGCAHPS survey was completed by a random sample of 12 patients and it demonstrated >90% patient satisfaction. Despite efforts to prioritize surveys, patient acuity and time often affected completion rates during appointments. Trust in the relationship with the team influences these results, as well as information bias, as patients who regularly attend appointments and complete the survey are more engaged. Because of small enrollment numbers at the time of this evaluation, it was not possible to identify trends in activation or adherence during serial patient assessments.
Quality
Table 2 displays quality metrics for 55 patients who were enrolled in the program for 6 months. There was a statistically significant increase in completion of cervical cancer screening (from 61.8% at baseline to 88.2% for enrolled patients, P < 0.05), and nonsignificant increases in diabetic eye examination (P = 0.056) and hypertension control (P = 0.219).
Average for metrics in surrounding medical home practice: *77%, **61.5%, ±49%.
Utilization
Table 3 displays pre and post outcomes for the pilot phase of the program. Overall, the CCP resulted in a 65% reduction in hospitalizations and a 67% reduction in emergency room visits. CCP investment was $750,000. The program achieved a net $1.6M cost savings, resulting in a 2.2:1 return on investment.
CCP, complex care program.
Discussion
To improve efficiency of the health care system, high-risk patients with disproportionately high utilization must be matched with commensurate health care resources. The study team developed a program for HNHC Medicaid patients as a special service center within an existing large, urban patient-centered medical home practice, in partnership with a Medicaid MCO and a large regional medical group. Within the first 18 months, the team developed a new practice and care team, enrolled 86 patients, and has demonstrated positive patient experiences, improvements in quality, and cost savings. The detailed description of program characteristics bridges knowledge gaps in how CCPs are designed. 24
The model provided a home for complex and costly patients within an existing medical home practice. The study team effectively carved out a niche of high-value service for an underserved population within a large, complex health care system. It is unique as the payer and medical group both had evidence that the existing UMH was not caring effectively for the subset of HNHC patients eventually targeted by the CCP program. By identifying a specific cohort and targeting services accordingly, the program conformed to known best practices in complex care. 5,18 Although it was necessary to invest in hiring and training new team members to staff the complex care practice, the partnership allowed for the optimization of costs by leveraging infrastructure that was already in place, including pharmacy, radiology, laboratory services, office space, and an integrated EHR.
The unique provider–payer partnership provided real-time sharing of clinical and claims data, and has been particularly useful for patient selection and utilization management. However, with several major stakeholders involved, the pilot was subject to a complex management structure and frequent staffing changes. Lessons learned during the pilot have been applied to improve the team and function of the CCP. For example, to assure continuity and connection, 2 providers initially shared call 24 hours/7 days. During the year, the schedule was adapted to offset call coverage needs of the program with a small pool of additional clinicians. Overall, patients adjusted well to this iteration. Although the team was able to manage the patient cohort effectively, expanding the program may require additional clinical support. Future iterations of the program may include risk sharing between the payer and the provider, allowing for distribution of the actualized cost savings, and further alignment of performance incentives.
The CCP was located within an existing medical home practice for several reasons. That practice already included a subpopulation of HCHN patients who both leadership and providers felt would benefit from the intensive services that the CCP program provided. The EHR and regional health information exchange allowed for care coordination both within the health system and with surrounding health systems. In addition, because medical home practices have been shown to be more successful in achieving appropriate care transitions, 21,36 it was hoped that locating the CCP within an existing medical home would (1) assist partnerships between the regular care team and the CCP team and (2) assist with efforts to transition management back to primary care providers once self-sufficiency was attained.
Integrated behavioral health and social services were critical in the study high-risk Medicaid population because 97% had at least 1 mental health disorder and all had at least 1 social need. Consistent with other programs, the CCP team was trained to be flexible and to adapt to iterations of a new care model. 20 Others have observed the special impact of poor mental health care and substance abuse on utilization, and the CCP program sought to address this by training all members of the team and providing a full-time embedded clinical counselor. 18,30 –34 The team's weekly meetings served as a time for reflection on patient care challenges and also supported the resiliency of the team's members. Near the conclusion of the pilot, direct support and collaboration was requested from psychiatry colleagues to provide clinical oversight and specialized care of the complex patients, based on the experiences of others that these behavioral resources were critical for patient engagement, medication adherence, and overall success. 30 –34
As anticipated, enrolling patients was time intensive and challenging. 4 Knowledge of CCP enrollment processes is limited, 24 and this study uniquely describes this component of the program. In addition, this study reports on recruitment efforts: 41% of the targeted cohort ultimately enrolled in the CCP, while 21% of total eligible patients were unreachable. The highest recruitment rate – 80% – was among patients referred to the CCP by primary care providers in the surrounding UMH. Although not surprising, it supports the importance of engaging primary care providers when developing and recruiting patients to programs such as this CCP.
Preliminary results from the monitoring and evaluation plan are encouraging. The majority of patients have completed PAM, MAQ-8, and PACIC surveys, and further analysis is planned for the comprehensive program evaluation. Early measures of patient satisfaction are promising. Quality measures showed trends toward improvement in completion of clinical preventive services, with a statistically significant increase in cervical cancer screening completion. Of note, some measures, such as blood pressure control, were met at higher rates than in the surrounding UMH.
Consistent with other complex care models, CCP patients utilized health resources at lower rates compared with their pre-enrollment baseline. 15,16,26 Emergency room utilization may be inappropriately promoted by referrals outside the CCP, psychosocial needs (anxiety, substance abuse, and unstable housing in particular), and lack of disincentives. 37 In the study team's experience, cultural and family pressure to seek emergency room services also plays a role, and changing these behaviors takes time. Hospitalizations, in contrast, were impacted by care coordination and intensive outpatient follow-up.
Several limitations affect these results. Evaluation of CCPs such as this one must consider the impact of “regression to the mean” – a tendency for costs to decline over time regardless of interventions; others have observed that more than 70% of saving in programs such as this one can be attributed to this phenomenon. 38 –40 Although ongoing data collection will soon permit analysis against an adequate control, an adjusted return on investment exceeded the target of $5000 per patient, sufficient for continued investment in the program. This CCP was developed in an academic medical practice in 1 state, and may not be generalizable to other settings. The state has a “carve out” for behavioral health services so predictive models were based on only medical claims data, and the predictive model may have missed other complex patients. Finally, very few of the patients transitioned back to routine primary care during this preliminary study, so the success of those transitions is unknown. Research is ongoing in these areas.
Building on other high-risk care models that have emerged to care for the nation's sickest and costliest patients, this unique CCP was developed with the goals of improving patient experiences, enhancing health in the targeted population, and decreasing costs. Based on promising preliminary outcomes, the study team is sharing their experience as a base for ongoing research, and in the hope that it will assist others to create successful programs.
Footnotes
Author Disclosure Statement
Dr. Okeke received consultancy fees for management consulting for Veterans Health Administration - Booz Allen Hamilton. The other authors declare that there are no conflicts of interest. The authors received no financial support for this article.