
Abstract
The guidelines provided by experts regarding various cancer screening tests are not universally accepted by physicians or patients. This systematic review describes the literature regarding the associations of physician characteristics with the implementation of and referral of patients for selected cancer screening tests. In October 2016, the authors conducted a thorough search of articles found in 4 databases, using keywords describing physician characteristics and cancer screening. English-language articles reporting on patient surveys or records of patients' screening history, and surveys of physicians' practices or opinions, in the United States were included. The physician characteristics most commonly analyzed were specialty and sex. The screening tests most commonly analyzed were those for cervical and colorectal cancers. Female and white physicians were found to screen more patients than male and nonwhite physicians. Obstetrician-gynecologists screened more for breast and cervical cancer than internists, who screened more than family or general practitioners. Physician sex, race, and specialty were consistently associated with cancer screening practices and should be the focus of efforts to harmonize practices with recommendations.
Introduction
R
Like most medical decisions, those regarding cancer screening involve the interplay and interaction of 4 groups of variables: patient demographic characteristics (eg, age, 9 –12 sex, 12 –16 race/ethnicity, 12,17,18 socioeconomic status 12,19,20 ), patient clinical characteristics (eg, risk of the disease in question, 21 –24 comorbidities 25 –27 ), system characteristics (eg, type of insurance, 20,28 –30 setting in which the patient is seen 31 –35 ), and physician characteristics (eg, specialty, 36 –38 age, 39 –41 sex, 39,40,42,43 board certification, 38,40,44 foreign medical graduate 39,40,44 –46 ). Studies have investigated the effects of patient and system variables on the utilization of various cancer screening tests.
This paper reviews the biomedical literature regarding the associations of physician characteristics with decisions regarding various common cancer screening tests. An understanding of these relationships may help to explain why screening practices vary 1 –4 and often are at odds with recommendations from expert panels and public health agencies. 47
Methods
Citation search strategy
The databases MEDLINE (1946 – October 2016), PubMed (1900 – October 2016), PsycINFO (1967 – October 2016), and EMBASE (1980 – October 2016) were searched using terms describing physician characteristics (keywords: physician characteristics, physician age, physician gender, physician education, physician specialty, physician training, physician experience, physician race, physician practice, international medical graduate, and board certification) and cancer screening (keywords: cancer screening, screening practices, and screening patterns). The “related articles” feature of PubMed was used to identify additional relevant articles. The study team also hand searched the references of retrieved articles to identify studies that the search strategy might have missed (Figure 1). Abstracts were included only if the data were not yet published in peer-reviewed journals.
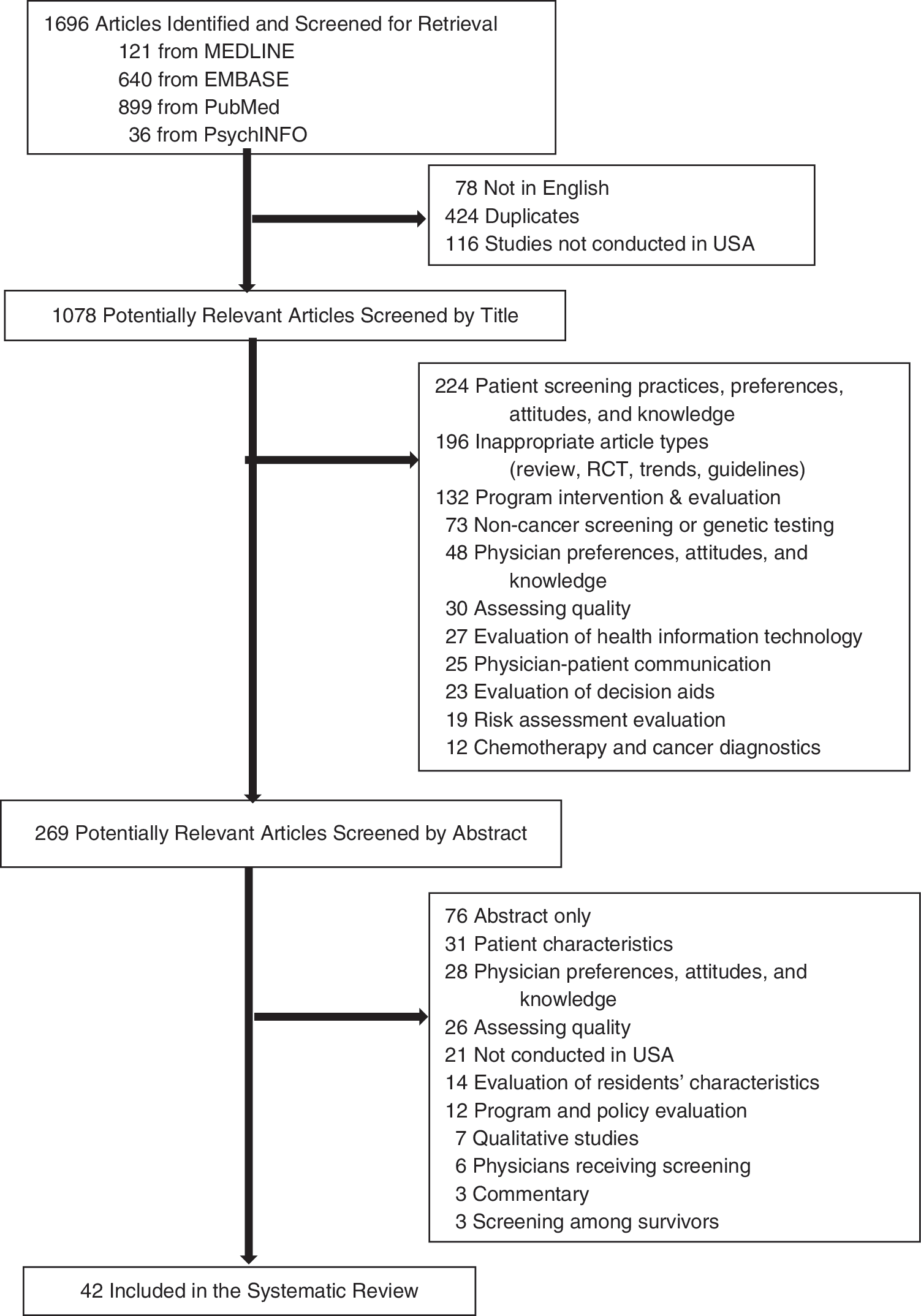
Flow diagram of article selection based on searches of keywords related to physician characteristics and cancer screening. RCT, randomized controlled trial.
Study selection
After all studies based on the search strategy were identified, 2 authors independently reviewed titles, then abstracts, then articles to confirm potential eligibility. Studies that were non–cancer related, focused on basic research, evaluated policies or programs, did not report on physician characteristics, were written in languages other than English, or sampled populations outside the United States were excluded.
Studies that focused on physician characteristics associated with receipt of cancer screening, selected studies that used patient-level data on cancer screening patterns linked with data on attending physician characteristics, and surveys of physician attitudes, recommendations, and use of cancer screening procedures were included. For studies that examined several different preventive screening practices, only those outcomes that were cancer related were included. The few discrepancies between the 2 reviewing authors were quickly resolved by either reaching consensus or seeking an opinion from a third author.
Data extraction and synthesis
A standardized extraction form was used to obtain data on study design and relevant results. The articles selected were reviewed, and data on study design, subjects, sampling methods, sample size, screening test type, response rate, and quantitative results were recorded in table form. All data were abstracted independently by each of the 2 authors and verified for accuracy by a third.
The selected articles were categorized into 10 groups based on physician characteristics observed in the studies: age, sex, race, experience, specialty, board certification, degree, physician training location (Unite States or foreign), volume of patients, and academic affiliation. Study design was classified as prospective cohort, retrospective cohort, case control, or cross-sectional. Subjects were classified as patients or physicians. The sample description was a brief summary of the cohort source. The screening test types included breast cancer (mammogram), colorectal cancer (CRC; colorectal screening), cervical cancer (Pap smear), and prostate cancer (PSA [prostate-specific antigen]), among others. The response rate included both the percent of physicians who responded to a survey and the percent of patients ascertained. The quantitative results were the measures of association obtained from the adjusted regressions. The quantitative results of each article were classified based on the overall effects observed.
Results
The search returned 1696 articles, 42 of which were included in the analysis (see Supplementary Table S1). Twenty-two studies (52%) were surveys of physicians, 14 (33%) were medical record reviews, and 6 (14%) were patient surveys.
The physician characteristics most commonly analyzed were specialty (81%), sex (69%), race (33%), experience (31%), and age (31%). Almost half (45%) the studies analyzed screening for cervical cancer, 33% for CRC, 29% for breast cancer, and 19% for prostate cancer; 1 analyzed lung cancer screening.
Demographics
Age
The papers yielded no consensus on the association of physician age with breast cancer screening (Table 1). For mammography, 2 studies had null results, 42,48 while others found a positive relationship 40 and an inverse relationship. 49 For clinical breast examination, results showed no association 49 or that older physicians screen less often. 48 Two of the 3 studies on Pap testing for cervical cancer 48,50 found no association with physician age and 138 found an inverse relationship.
ACS, American Cancer Society; CBE, clinical breast exam; CI, confidence interval; COL, colonoscopy; CRC, colorectal cancer; DRE, digital rectal exam; FOBT, fecal occult blood test; FS, flexible sigmoidoscopy; OR, odds ratio; PSA, prostate-specific antigen; yrs, years.
Reference.
Three of 5 studies found a positive relationship between physician age and CRC screening rates. 41,44,51 These studies generally looked at a combination of CRC screening methods, including fecal occult blood test (FOBT), flexible sigmoidoscopy, and colonoscopy. Two studies found that older physicians screen less often for CRC, 39 but Brownson et al found that older physicians screened less often with FOBT, but not with flexible sigmoidoscopy. 48 Two studies found no association of physician age with PSA testing, 52,53 but Hall et al found that older physicians were marginally more likely to have a policy of encouraging patients to get PSA tests.
A study by Weisman et al found that older physicians were less likely than younger physicians to adhere to American Cancer Society (ACS) guidelines for breast, cervical, and CRC screening of asymptomatic patients older than 65 years, although it was unclear whether the nonadherent physicians screened more or less often than recommended. 54
Sex
Physician sex most strongly influenced screening practices for breast cancer, but also influenced gynecological and CRC screening (Table 2). Six of 10 studies found that female physicians screen more often with mammography than male physicians. 40,42,45,49,55,56 One study found that males screen more often, 57 and 3 others showed no association. 58 –60 For clinical breast examinations (CBEs), 1 paper showed no association, 57 and another that females screen more often. 49
AMA, American Medical Association; CBE, clinical breast exam; CI, confidence interval; COL, colonoscopy; CRC, colorectal cancer; FOBT, fecal occult blood test; FS, flexible sigmoidoscopy; LDCT, low-dose computed tomography; OR, odds ratio; PCP, primary care physician; PSA, prostate-specific antigen; yrs, years.
Reference.
Studies of gynecological cancer screening did not show an obvious pattern. Only 4 of 12 studies found that females screen more often. 43,56,59,60 Six of the 8 remaining studies found no association, 38,50,55,58,61 –63 and 1 found that males screen more often. 64
Three of the 9 studies of CRC screening found that females screen more often 39,65,66 and 6 found no association. Four studies found no association between physician sex and prostate cancer screening discussion, recommendation, or frequency. 20,52,53,67 The one study of physician sex and lung cancer screening found no correlation. 68
Race/ethnicity
Findings varied regarding the relationship between mammography/CBE screening and physician race (Table 3). Leach et al found that non-Hispanic white physicians were less likely to over-recommend screening than physicians of other races, 42 while another study found no association. 49 Lew et al found lower screening rates among patients of Korean physicians in the United States than among patients of non-Koreans. 69
CBE, clinical breast exam; CI, confidence interval; COL, colonoscopy; CRC, colorectal cancer; FOBT, fecal occult blood test; OR, odds ratio; PSA, prostate-specific antigen; yrs, years.
Reference.
Several studies showed that Asian physicians screen less often for gynecological or ovarian cancers. One study found that Asians screen less often for cervical cancer than blacks, 62 and another found that Asians screen less often for ovarian cancer than whites. 43 A third found that white physicians recommended Pap and HPV DNA screening more than did Asians, but that both did so more than others 63 ; another study found higher Pap screening rates among patients of non-Korean physicians than among patients of Koreans. 69 Two other studies found no association. 50,64
Two studies suggested that white physicians did more CRC screening than physicians of other races. 46,66 Zapka et al 46 found that non-Hispanic white and Asian primary care physicians were more likely than other primary care physicians to report recommending FOBT with colonoscopy/colonoscopy only, compared with other tests or test combinations. However, their 2012 study 41 did not find an association of race/ethnicity with increased (over time) ordering of colonoscopy vs. other tests.
Two studies indicated that black physicians screen more than those of other races for prostate cancer. One study found that black physicians were less likely than others to discontinue annual screening of patients older than a specific age cutoff, 20 and another found that non-Hispanic black physicians were more likely to discuss PSA tests than non-Hispanic whites. 52 Conversely, Wallner et al found that white and Asian providers screened more often than black and Hispanic providers. 70
Training and background characteristics
Degree
The one study to compare screening practices of allopathic and osteopathic doctors found that allopathic physicians screened more with mammograms, CBE, Pap tests, digital rectal exams, sigmoidoscopy, FOBT, skin exams, oral cavity exams, and testicular exams (data not shown). 48 Another study found no differences between allopathic physicians and physician assistants and nurse practitioners with respect to mammography, Pap test, and CRC screening. 60
Training, foreign vs. United States
Findings varied regarding the relationship between location of medical training and mammographic screening practices (Table 4). One study found no association, 42 another found that foreign-trained physicians screen more often than US-trained physicians, 40 and a third study found that physicians trained in the United States or Canada screened more often than those trained elsewhere. 45 Findings regarding training location and CRC screening also varied. One study found no association, 45 but another found that US-trained physicians screen more often than those trained elsewhere. 39 Yabroff et al found that US-trained physicians were more guideline consistent than others, 44 suggesting lower screening rates, while Zapka et al 46 found that US-trained physicians were less likely than foreign-trained physicians to discuss more than 1 test option with their patients.
CBE, clinical breast exam; CI, confidence interval; COL, colonoscopy; CRC, colorectal cancer; FOBT, fecal occult blood test; FS, flexible sigmoidoscopy; OR, odds ratio; yrs, years.
Reference.
Board certification
Two studies found that board-certified physicians screen with mammography more often than those without such certification (Table 5); 40;45 another study found that non–board-certified physicians are more likely to under-screen (screen less often than guidelines specify) with mammography, 55 although a fourth study found no association. 42 One study found that non–board-certified physicians over-screened with Pap tests, 55 and another determined that board-certified physicians were more guideline consistent than those without certification. 38
BC, board-certified; CBE, clinical breast exam; CI, confidence interval; COL, colonoscopy; CRC, colorectal cancer; FOBT, fecal occult blood test; FS, flexible sigmoidoscopy; LDCT, low-dose computed tomography; NBC, non–board-certified; OR, odds ratio; PSA, prostate-specific antigen; yrs, years.
Reference.
In 2 studies, board-certified physicians were found to perform more colon cancer screening than other physicians, 45,65 but Yabroff et al found that board-certified physicians were more guideline consistent (less likely to over-screen) than others, 44 and Zapka et al found no association. 46 The one study of lung cancer screening found no association with board certification. 68
Specialty
Three studies found that obstetrician/gynecologists (OB/GYNs) perform more mammographic screening than internists and family practitioners (FPs) or general practitioners (GPs) (Supplementary Table S2). 36,42,71 Five studies also found that FPs screen less often than internists, 36,40,45,49,54 but Leach et al found that internists screen less often than FPs. 42 Four studies found no association with mammography. 54,55,60,72
Three studies found no association of specialty with gynecological cancer screening, 55,62,72 but 6 found that OB/GYNs screen more often FPs/GPs. 36,37,43,54,61,63 All but 1 of these studies found that internists screen less often than FPs/GPs. 63 One found that internists screen more than FPs. 60 Two studies found that OB/GYNs were less guideline consistent than internists. 38,50
Armour et al found that internists screen more often for CRC than physicians in other specialties. 73 Two studies found that internists screen more often than OB/GYNs. 41,54 Four studies found that internists screen more often than FPs/GPs. 39,44,45,60 However, Zapka et al found that FPs were more likely to discuss more than 1 test option than internists, 46 and Richards et al found that GPs screen more often with FOBT than internists. 51 Three additional studies found no association. 58,65,72
Specialty was not consistently associated with PSA testing. Four of 7 studies found no association. 20,52,53,74 Two of the remaining 3 suggested that FPs/GPs screened more often than internists, 67,75 but the third suggested that internists screened more often than FPs/GPs. 70 The one study of lung cancer screening found that internists screened more often with low-dose computed tomography (LDCT) than FPs/GPs. 68
Practice characteristics
Experience
None of the 3 studies of breast cancer screening found an association between years of experience and screening rates (Supplementary Table S3). 45,55,76 Most studies of gynecological cancer screening also found no association, 55,61,63,76 although 1 found a positive relationship. 43 Two of 4 studies found no association of CRC screening with physician experience. 45,73 One found a positive association of experience with the use of FOBT among patients with terminal comorbidities, but a stronger inverse relationship of experience with flexible sigmoidoscopy use in patients with no, mild, or moderate comorbidities. 65 Singal et al also found an inverse relationship of experience with any form of CRC screening. 39 For PSA testing, 2 of 3 studies found no association. 20,52 Edlefsen et al did find a positive relationship of experience with screening among male physicians, but no association among female physicians. 67 The one study of lung cancer screening found a positive relationship between experience and screening with LDCT or chest radiographs. 68
Volume of patients
Most studies found positive associations between the volume of patients seen and cancer screening practices (Supplementary Table S4). For breast cancer, one study found no association, 76 but another found that physicians with more patients screened more often with mammography for patients with a life expectancy of at least 7 years than physicians with fewer patients. 40 Similarly, physicians who saw fewer patients per week reported more guideline-consistent CRC screening practices than those who saw more patients. 44 One study found that physicians with more patients were more likely than those with fewer patients to have a policy of trying to talk patients into getting a PSA test, 52 and another found a positive relationship between number of patients seen and PSA testing rates. 53 However, physicians with fewer patients were more likely to screen for lung cancer with chest radiography than physicians with greater patient volume. 68
Academic affiliation
Three of 4 cross-sectional studies found no association of academic affiliation with cancer screening practices (Supplementary Table S5). 38,42,44 The fourth found that non-affiliated physicians were less likely to recommend FOBT with colonoscopy or colonoscopy alone versus other screening types for CRC than physicians in academic settings, but the study did not explore overall testing frequency. 46
Discussion
This systematic review analyzed 42 studies exploring the associations of 10 physician characteristics with screening for breast, colorectal, cervical, prostate, and lung cancers. The aim was to examine the roles of those characteristics in discrepancies between screening frequency and the guidelines regarding specific cancer screening tests. The study team found that: Female physicians, OB/GYNs or internists, and board-certified physicians were more likely than males and non-specialists to perform, to refer for, or to recommend mammographic screening. Asian physicians were less likely and non–board-certified physicians, OB/GYNs, and FPs more likely to screen patients with Pap tests. White physicians, internists, and those with more patients were more likely to screen patients for CRC than Asian or black physicians, other specialists, or physicians with smaller practices. Black physicians and those with more patients were more likely to screen patients with PSA tests than physicians of other races.
Because only 1 study of lung cancer screening was found, the study team was unable to draw conclusions about relevant physician characteristics; the team suggests that future studies examine this topic.
Several of the aforementioned observations may reflect physician diligence about screening for patients with whom they personally identify. 77 Black physicians may screen more for prostate cancer because of their concern about the high prevalence of prostate cancer among black men. 20,52 Likewise, female physicians may screen more for breast cancer because they identify with their female patients and because female patients may be more likely to follow through with obtaining a mammogram when a female physician suggests it. 56
Differences in practices associated with physician specialty may have arisen because subspecialists are more confident than generalists in the guidelines developed by the governing organization of their particular subspecialty. 36,78 Leach et al suggest that OB/GYNs make greater use of mammography than other physicians because they are more often targets of medical malpractice suits. 42 Internists may refer patients to subspecialists for preventive care more often than do FPs and GPs because they have more established subspecialist referral networks. 45
Specialty and sex were by far the most common characteristics studied, and the associations of screening with those variables were consistent across studies. Future investigators of screening practices might contribute to the literature by examining the association of screening practices with physician race/ethnicity, practice volume, and board certification.
The studies included were published between 1989 and 2015, a time frame during which cancer screening guidelines changed dramatically. Most of the studies were cross-sectional, and each presented data on rates of screening or consistency with the guidelines at its time of publication. The ACS has updated and publicized its guidelines for breast, cervical, colorectal, prostate, and lung cancer screening every few years since 2001. 79 Therefore, it would be beneficial for future studies to examine changes in screening practices in relation to physician characteristics before and after changes in those guidelines, as Goodwin et al did. 53
The study team did not perform meta-analyses because the 42 studies varied in design and outcomes. For example, some studies reported on the proportions of patients who had or reported having a given test, whereas others analyzed physician responses to hypothetical vignettes. Given the small sample (42 papers) and the diversity of approaches, meta-analysis would have necessitated a large number of calculations that would have been difficult to interpret meaningfully.
Several studies found only that physicians with a certain characteristic used certain screening tests more or less than others without that characteristic. The studies that analyzed the consistency of screening-related behavior with guidelines were more useful from a public health perspective, especially when they specified the direction of the inconsistencies. 38,44 A few studies also assessed physicians' beliefs about the efficacy of screening and potential influences, such as clinical evidence or patient insistence. 38,44 It also may be useful to consider how physician characteristics and screening-related behavior relate to knowledge of or agreement with screening guidelines, or to the potential economic benefits of screening.
This review had several limitations. Given the number of characteristics and screening tests that could be used as search terms, the study team may not have found all relevant studies, despite hand-searching bibliographies. In addition, two thirds of the studies reviewed were surveys of patients or physicians rather than chart or database reviews that documented actual practice; thus, the findings may have reflected reporting biases. Some physician surveys asked for opinions but did not relate the opinions to the guidelines. Patients' reports on their past medical or screening history also may have been subject to faulty recall. Most of the physician surveys (59%) used data from the American Medical Association Master File. If their purpose is to relate physician characteristics to the proportions of patients actually tested, future studies should be based on patient chart reviews or billing records.
Another possible source of bias was the overall agreement among authors about the criteria for article selection. Figure 1 lists those criteria; through them the study team may have inadvertently excluded some articles that would have provided a different slant on the determinants of physician screening behavior.
However, this systematic review highlights several physician characteristics that were correlated with cancer screening rates, namely physician sex, specialty, and race/ethnicity. Based on these results, members of the medicine and public health communities can better understand the discrepancies between recommendations and physician practices. As electronic health records and health communications systems become more sophisticated, it is increasingly possible to notify physicians when patients are due for a given test and when referrals for tests are inappropriate. We can then study the effects of such communications on both physician and patient adherence to the guidelines, given their individual characteristics.
Footnotes
Author Disclosure Statement
Dr. Neugut has consulted for Pfizer, Teva Pharmaceuticals, Eisai Pharmaceuticals, Otsuka Pharmaceuticals, and United Biosource Corporation, and is on the Medical Advisory Board of EHE, Intl. None of these associations is related to the topic of this study. The other authors have no conflicts of interest. Ms. MacLean was supported by a grant through the Brain Tumor Foundation.
Supplementary Material
Supplementary Table1
Supplementary Table2
Supplementary Table3
Supplementary Table4
Supplementary Table5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.