
Abstract
The objective was to estimate the association between health care expenditures and implementation of preventive mental health programs by local health departments (LHDs). Multilevel nationally representative data sets were linked to test the hypothesis that LHDs' provision of preventive mental health programs was associated with cost savings. A generalized linear model with log link and gamma distribution and state-fixed effects was used to estimate the association between LHDs' mental illness prevention services and total health care expenditures per person per year for adults aged 18 years and older. The main outcome measure was the annual total health care expenditure per person. The findings indicated that LHD provision of population-based prevention of mental illness was associated with an $824 reduction (95% confidence interval: -$1,562.94 to -$85.42, P < 0.05) in annual health care costs per person, after controlling for individual, LHD, community, and state characteristics. LHDs can play a critical role in establishing an integrated health care model. Their impact, however, has often been underestimated or neglected. Results showed that a small investment in LHDs may yield substantial cost savings at the societal level. The findings of this research are critical to inform policy decisions for the expansion of the Public Health 3.0 infrastructure.
Introduction
M
Local health departments (LHDs) are positioned at the center of community health programs and play a valuable role in delivering essential public health services, 4 including serving as providers of last resort for vulnerable populations. Furthermore, LHDs play a central role in delivering population-level programing, including educating, screening, and referring community members to mental health care. LHDs can utilize existing infrastructure and resources to connect and collaborate across programs and organizations. 5 Available research documents clearly that LHD activities are associated with reduced preventable deaths, 6 lower racial disparities (comparing African Americans to Whites), 7 and improved self-reported health. 7 –10 The literature also shows that integration of LHDs with community partners is associated with a reduction in the incidence rates of infectious and chronic conditions. 11 –13
LHDs play critical roles in primary, secondary, and tertiary prevention according to the Essential Public Health Services model developed by the Centers for Disease Control and Prevention. 4 However, research is still needed to increase understanding of how LHDs can be effectively integrated with community partners to improve prevention of and treatment for mental illness. 2,14,15 In a previous study, the research team examined multiple roles that LHDs play in preventing mental illness. Using an ecological multilevel model to delineate the roles of LHDs, the team found that LHD mental health promotion activities and mental health preventive care were significantly associated with reductions in preventable hospitalizations for individuals with ambulatory care sensitive conditions and co-occuring mental health problems. 13 Another study also suggested that LHDs' delivery of mental illness prevention activities was associated with a significant reduction in the 30-day readmission for adults aged 18–64 years. 16
After reviewing the literature, the research team believes the present study is the first empirical effort to estimate the association of health expenditures with mental health preventive programs implemented by LHDs. Specifically, this study examines the extent to which total annual health care expenditures per capita vary by LHDs' provision of mental health preventive care. The research team hypothesizes that LHDs' provision is cost-effective from a societal perspective (ie, LHDs' inexpensive provision of preventive care is associated with lower total health care expenditures). In addition, untreated mental illnesses are associated with increased risk of developing major chronic diseases, including heart disease, diabetes, asthma, and hypertension, among others. 17 –19 The team further hypothesizes that LHD mental illness prevention works more effectively in the primary prevention, ie., it is associated with more cost reductions among the population who have not developed severe psychological distress (SPD) and/or major chronic conditions. The present study serves as a starting point to establish a baseline for future studies of LHD participation in population-level mental health promotion and mental illness prevention efforts. The findings of this research are useful to inform policy decisions for the expansion of the Public Health 3.0 infrastructure 20 and have implications for operationalizing the 21st Century Cures Act, 21 which strives to improve availability of evidence-based mental health services.
Methods
The research team constructed a unique multilevel data set at the individual-, LHD-, community-, and state levels. The main data set was the 2012 Medical Expenditure Panel Survey (MEPS), a nationally representative survey that provided comprehensive information on respondents' health care expenditures, as well as their demographic and socioeconomic status. MEPS data were linked to the National Association of County and City Health Officials (NACCHO) Profiles Survey, the Area Health Resource File, and US Census data using zip codes.
The key predictor was LHDs' provision of population-based primary prevention activities for mental illness, and the connection between LHD and community services. Four exhaustive and mutually exclusive dichotomous variables were constructed: direct LHD performance of mental illness prevention activities alongside community activities, direct LHD performance of mental illness prevention activities only, LHD contracted mental illness prevention activities, and no-LHD involvement in mental illness prevention (the reference group). Preventive care includes services such as initial screening and case detection, identifying and tracking those at high risk for relapse and those not adhering to treatment, structuring follow-up, and monitoring outcomes. The NACCHO data set contains detailed information on LHD activities and was used to construct this measure. Representatives of each LHD responded to the survey questions for its jurisdiction.
A generalized linear model with log link and gamma distribution and state-fixed effects was used to estimate the association between LHDs' mental illness prevention services and total health care expenditures for adults aged 18 years and older (Equation 1).
where
For all the multivariable estimations, the Andersen behavioral model was used to select individual-, LHD-, community-, and state-level predictors of health care expenditures. These variables included age, sex, race/ethnicity, education, family income, self-reported health status, presence of chronic conditions (eg, high blood pressure, heart diseases, asthma), urban/rural residence, percentage of the population residing in a county who report African American ancestry, percentage of the county population without high school degrees, percentage of the county population who were foreign born, county poverty level, number of Federally Qualified Health Centers in the county, number of community mental health centers, and the state indicator. These variables have been identified in the literature as predictors of health care costs. 22 All health care expenditures were adjusted using 2014 dollar values according to the Consumer Price Index for medical care. The final sample size was 22,530 adults.
In addition, analysis was conducted among populations who had not developed SPD or any major chronic conditions (ie, the population who might benefit the most from the preventive care). The Kessler 6 (K6) score (Kessler score ≥13) was used to measure the presence of SPD. The Kessler 6 score includes 6 mental health-related questions that assess the person's “non-specific psychological distress” during the past 30 days. These include feelings of nervousness, hopelessness, restlessness or feeling fidgety, being so sad that nothing could cheer them up, that everything was an effort, or that they felt worthless. The items were summed to a score that ranges from 0 to 24; higher scores denote a greater tendency toward mental disability. Individuals were considered to have severe psychological distress if their K6 scale was
Results
Figure 1 illustrates total health care expenditures by the population average, among people with severe SPD, without SPD, and without SPD or any chronic condition. Mean expenditures among adults were $5325 while the average cost of individuals with SPD exceeded $7364. Individuals without SPD or major chronic conditions spent $2301 on health care.
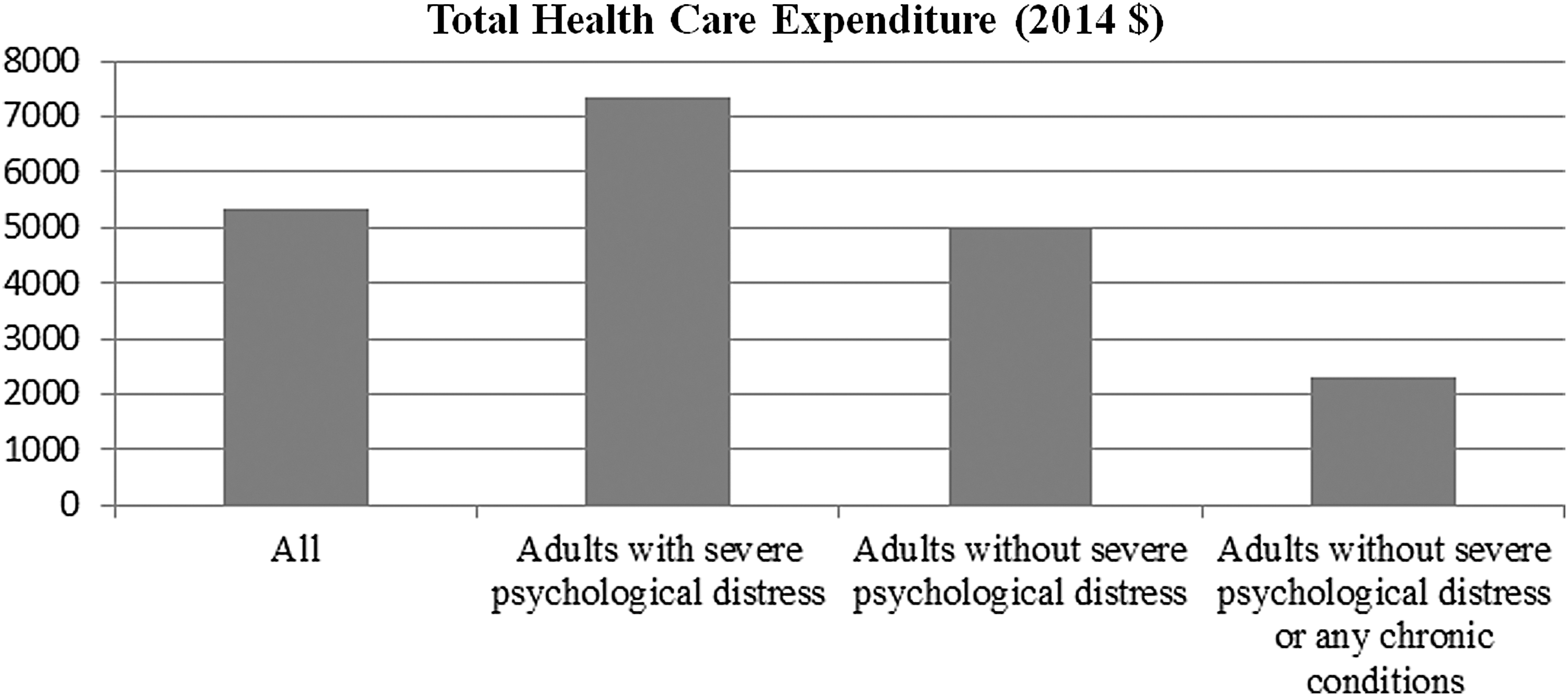
Variations of total health care expenditures by the presence of severe psychological distress. Source: The 2012 Medical Expenditure Panel Survey (MEPS). Results are nationally representative. All of the health care expenditures were adjusted using 2014 dollar values according to the Consumer Price Index for medical care. Major chronic conditions are identified in MEPS data. These conditions are high blood pressure (including multiple diagnoses), heart disease (including coronary heart disease, angina, myocardial infarction, and other unspecified heart disease), stroke, emphysema, chronic bronchitis, high cholesterol, cancer, arthritis, and asthma.
Approximately 17% of individuals lived in zip codes where LHDs were involved in the provision of preventive care for mental illness, and 73% of individuals lived in zip codes without either LHD direct performance or contracted provision of mental illness prevention activities (Table 1). Among individuals without SPD or any chronic condition, 18% were identified as African Americans and 35% as Latinos, while among individuals with SPD, 22% were identified as African Americans, and 30% as Latinos. Individuals without SPD or any chronic conditions were more likely to be younger and uninsured compared to the sample average. They also were more likely to live in areas with higher proportions of foreign-born individuals.
Data source: the linked data set of the 2012 Medical Expenditure Panel Survey (MEPS), the 2013 National Association of County and City Health Officials Profile Survey, the Area Health Resource File, and US Census Data.
Major chronic conditions are identified in the MEPS data. These conditions are high blood pressure (including multiple diagnoses), heart disease (including coronary heart disease, angina, myocardial infarction, and other unspecified heart disease), stroke, emphysema, chronic bronchitis, high cholesterol, cancer, diabetes, joint pain, arthritis, and asthma.
FPL, federal poverty level; FQHC, Federally Qualified Health Center; LHD, local health department; SPD, severe psychological distress;
Regression results (Table 2) showed that direct LHD performance of population based mental illness prevention activities was significantly associated with lower health care expenditures (coef = −0.23, P < 0.05). The results also demonstrated that LHDs' mental illness prevention activities worked more effectively among people who had not developed mental or physical chronic conditions (coef = −0.26, P < 0.05; coef = −0.51, P < 0.001, respectively).
Data source: The linked data set of the 2012 Medical Expenditure Panel Survey (MEPS), the 2013 National Association of County and City Health Officials Profile Survey, the Area Health Resource File, and US Census Data. The sample size of people older than 18 years was 25,446. After excluding 2916 observations with missing values (11%), the final sample size was 22,530. The Kessler 6 score (Kessler ≥13) was used to measure the presence of SPD.
P < 0.001, ** P < 0.01, * P < 0.05.
Generalized linear model with log link and gamma distribution was used to estimate the cost given its skewed distribution. All regressions controlled for age, sex, race/ethnicity, education, family income, self-reported health status, presence of chronic conditions (eg, high blood pressure, heart diseases, asthma), urban/rural residence, percentage of the population residing in a county who report majority African American ancestry, percentage of the county population without high school degrees, percentage of the county population who were foreign born, county poverty level, and number of Federally Qualified Health Centers, number of community mental health centers, and the state indicator. These variables have been identified in the literature as predictors of health care costs.
CI, confidence interval; Coef, coefficient; LHD, local health department.
Based on the cost equation, the research team further estimated that LHD-led provision of population-based prevention of mental illness was associated with an $824 reduction (95% CI: -$1562.94 to -$85.42, P < 0.05) in annual health care costs per person, after controlling for individual, LHD, community, and state characteristics (Table 3). Compared to communities without LHD involvement in mental health prevention, communities with LHD direct provision of mental health preventive care and other community resources had $565 lower average total health care expenditures, but this reduction was not statistically significant; communities with mental health preventive care contracted out by LHDs had $250 higher average total health care expenditures per person, but this difference was not statistically significant.
Source: the linked data set of the 2012 Medical Expenditure Panel Survey (MEPS), the 2013 National Association of County and City Health Officials Profile Survey, the Area Health Resource File, and US Census Data.
P < 0.001, ** P < 0.01, * P < 0.05.
Generalized linear model with log link and gamma distribution was used to estimate the cost given its skewed distribution. All regressions controlled for age, sex, race/ethnicity, education, family income, self-reported health status, presence of chronic conditions (eg, high blood pressure, heart diseases, asthma), urban/rural residence, percentage of the population residing in a county who report majority African American ancestry, percentage of the county population without high school degrees, percentage of the county population who were foreign born, county poverty level, and number of Federally Qualified Health Centers, number of community mental health centers, and the state indicator. These variables have been identified in the literature as predictors of health care costs.
CI, confidence interval; LHD, local health department
Discussion
National health care expenditure was $3.2 trillion, or $9,990 per person, in 2015. The public health system only received 3% of these outlays (ie, $108.92 per capita), with $55 per capita spent at the local level. 20 The present study findings suggest that LHD provision and involvement in population-level mental health activities has the potential to generate significant cost savings. In particular, these findings indicate that individuals living in areas with direct LHD provision of population-based prevention activities for mental illness had $824 lower annual health care costs per person, compared to individuals living in areas without any provision of similar services. Although the research team does not have cost data on expenditures by LHDs for preventive mental health interventions, they are likely to be far less than the cost savings associated with these public health measures. Results of this study provide the first evidence of the likely cost-effectiveness of integrating LHDs in the health care delivery system to promote mental health, especially for people with limited health care resources.
These findings align with the Substance Abuse Mental Health Services Administration and Health Resources and Services Administration integration model for mental health services 25 and the National Institute of Mental Health (NIMH) strategic initiative to augment the public health impact of NIMH-funded work. 26 The findings suggest that LHD-led initiatives to prevent mental illness and promote mental wellness can be effective in bending the health care expenditure cost curve. The research team speculates that because the public health model relies first and foremost on assessment of community health needs, LHD-led programs are more likely to be responsive to community needs, may be more likely to be sustainable over time, and are more likely to leverage community engagement and trust effectively to accomplish programmatic aims. Handler and colleagues wrote in 200127 that based on the Essential Public Health Services model, LHDs are charged with improving population health by informing, educating, and empowering community members about health issues. Further, within the framework of the Essential Public Health Services, LHDs are positioned to develop policies and support implementation of plans and programs that improve personal and community health. LHDs accomplish this charge by enforcing health protection laws and working with community partners and other local government entities to ensure safety. Finally, within the assurance function, LHDs serve as providers of last resort for the uninsured and link people with services and supports to enhance health and well-being. 27 In a recently described theoretical framework by Chen et al, 28 LHDs can serve as community-based leaders that assess, monitor, and assure population-level service provision to advance a patient-centered learning health care system. 28
Limitations of this study include using a binary variable to capture LHDs' preventive mental health care efforts. Variations in the percent of LHD time dedicated to such mental health prevention efforts, type of program, and program implementation methods are not captured. Secondly, LHD activities were self-reported, and thus might be exposed to measurement error. However, the LHD official responding to the NACCHO questionnaire should know the nature and scope of the services and programs that her/his LHD offers. Thirdly, a cross-sectional design was used to examine the association between health care expenditures and LHDs' mental health promotion activities. The strength of this approach is its ability to capture multiple levels of the social-ecological factors that impact health care expenditures; the weakness is that it is not able to establish causality.
Finally, despite controlling for a wide set of individual and community characteristics, some confounding variables, such as unmeasured characteristics of LHDs that engage in preventive mental health interventions and local areas with lower health care spending, might be omitted because of data limitations. To establish causality, nationally representative longitudinal data sets with comprehensive measures on local public health systems should be established and used to validate these findings. Nevertheless, this study is the first, to the research team's knowledge, to develop empirical estimates suggesting the cost savings of LHDs' provision of mental illness preventive care to the community.
Public health implications
As the United States seeks to control health care spending, it is essential that local organizations such as LHDs be involved in the coordination of preventive service delivery. Practical steps that LHDs can take include prevention of alcohol, tobacco, and other substance use through the use of liquor control boards and local zoning ordinances to reduce availability of harmful substances; promoting resilience through evidence-based marital and family approaches; and promoting positive social connectedness through community programs. Ongoing work is needed at the federal, state, and local levels to promote LHDs' provision of preventive mental health services to promote population health. Results of this study can help policy makers at the federal, state, and local levels further refine their policies targeting population health, and truly make care for mental health disorders integrated and sustainable.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The authors received the following financial support: This work was supported by the National Institute of Mental Health (Grant R21MH106813).