
Abstract
Understanding how unmet basic needs impact health care in patients with complex conditions is vital to improve health outcomes and reduce health care costs. The purpose of this observational study was to explore the association between health care and socioeconomic needs and health care utilization and disease management among patients with chronic conditions at an intensive, patient-centered, office-based program. The study used a cross-sectional design and a convenience sampling approach. Data were collected through a patient questionnaire and medical records. Analysis included descriptive and inferential statistics. Data from 48 established patients were analyzed. Financial and lack of transportation were the 2 most frequently reported unmet needs. More than 65% of participants had their chronic condition(s) under control. Sex and ethnicity were the only 2 demographic variables that yielded significant differences (P ≤ 0.01) on visits to the emergency room and having chronic condition(s) under control. Those who reported having unmet transportation needs were more likely to have a condition uncontrolled and to have lost medical appointments compared to those who had this social need met (P ≤ 0.05). Statistically significant differences in terms of missing medical appointments also were found between those whose overall financial and housing needs were unmet and those who had those needs met (P ≤ 0.05). Results indicate that participating patients generally had good control of their conditions. The study adds evidence in support of the call for health care to address patients' socioeconomic needs, and the health care benefits of intensive case management programs. The model may be considered for adoption throughout New Mexico, and nationally.
Introduction
P
Background
There is evidence of the health and economic impact of social factors on disease management and health outcomes. Some studies have attributed as much as 40% of health outcomes to social and economic factors. 6 Unmet social needs such as inadequate housing, food insecurity, and unemployment have been related to physical and mental health problems, shorter life expectancy, and increased health care utilization and costs. 7 –17 Evidence of the impact of social factors on health outcomes and health care cost is prompting providers to develop models and implement interventions that incorporate patients' social needs into standard care. Models include educating medical students on social determinants of health, 18 and developing a culture in which assessing and addressing social determinants of health is considered part of high-quality primary care. 19 –21
Promising interventions usually link patients who have chronic, complex medical conditions to existing community resources as part of the care management approach. They may allow providers to write prescriptions to alleviate basic needs, such as food and heat. 22 These “social” interventions may contain cost, 23 –25 improve providers' productivity, 26 and increase satisfaction for both providers and patients. 27,28 There is also some evidence that properly addressing the social context in the delivery of health care services can have an important impact in improving health. 29
The aim of this study was to determine the most prevalent health care and socioeconomic unmet needs as well as the association between these needs and health care utilization and disease management among patients at the University of New Mexico Health Sciences Center (UNM HSC) Care One program.
Care One Program
UNM Hospital (UNMH) is the state's primary referral center, cares for a large and diverse population with complex and urgent health needs, and receives more than 491,000 outpatient and 93,000 emergency visits annually. The Care One program at UNMH was established in 2004 to offer intensive case management in an office-based setting to high-cost, medically complex patients who reside in Bernalillo County. 30 Often these patients do not have a regular source of care and have difficulty navigating the health care system, and many only seek care after a catastrophic illness or event occurs. This leads to significantly increased utilization, poorer health outcomes, and higher costs.
The Care One team is comprised of a physician, a social worker/case manager, a patient care coordinator, and a mental health therapist. Participants in the program are selected by UNMH from among the top 1% of costliest and complex users based on claims and diagnosis/prognosis. The Care One team evaluates the patients' needs and selects those with the potential to benefit the most from the services offered by the program. The basic criteria for empanelling a patient include having 2 or more chronic medical conditions, likelihood of recurrent illness, high risk for future hospitalization, and willingness to attend outpatient visits and comply with therapy. Patients who agree to participate in the program must be willing to be monitored and contacted. Common exclusions include acute health events that are not expected to recur (eg, a motor vehicle accident), residing outside the service area, and chronic substance abuse as the primary issue.
UNMH primary care providers are incentivized to accept Care One patients, and patients receive priority access to specialists. Patients are offered ongoing care and social support, and a pharmacist assists with medication management services for patients with complex comorbidities and multiple medications. The typical Care One patient has 3 or more chronic conditions. Although the number of patients varies according to available resources, the Care One program currently serves an estimated 600 patients. Among these patients, diabetes mellitus is the most prevalent condition (more than half of the patients), followed by congestive heart failure and chronic pulmonary disease (about one quarter of patients). Regarding demographics, mean age is 55.5 years, 45% are females, and nearly 50% are Hispanic. Most patients have Medicare or Medicaid, and about one third are classified as indigent.
Participation in the Care One program offers patients access to assistance with a variety of social services, such as options for transportation to appointments, food stamp applications, home nursing care options, and assistance with paperwork for financial benefits. Although this service may address the unmet needs of Care One patients, how this may affect health care utilization and disease management has not been explored.
Methods
This was an observational, cross-sectional study, and was conducted between March and May of 2017. The UNM Institutional Review Board (IRB) approved the study, determining that it was of minimum risk, and all participants were presented with and signed a bilingual informed consent prior to inclusion and data collection (Study ID: 16–175).
A convenience sampling approach was implemented to recruit 60 participants from the approximately 600 patients who constitute the panel of the Care One program. Inclusion criteria included: (1) registered patient attending follow-up appointments; (2) adult 18 years of age and older; (3) English or Spanish speaker. Potential participants were identified through the clinic's Power Chart System, which includes appointment schedule and follow-up visits. A trained bilingual research assistant (RA) contacted patients who had upcoming appointments by phone. Those who did not answer the call or were not identified prior to the appointment were recruited on-site. The RA used an IRB-approved bilingual English/Spanish recruiting script to explain the purpose of the study. Those who were interested in participating were presented with the informed consent and asked to be interviewed right after the clinical visit. They received the same standard care as the rest of Care One clinic's patients.
Primary data were collected through a bilingual facilitated questionnaire with closed-ended and open-ended response scales developed by the research team; participants were given the option to select their preferred language. The questionnaire consisted of a demographic section with standard items such as sex, age, race/ethnicity, education, country of birth, and household income; and a 35-item section that included the study's 2 dimensions of interest: health care and socioeconomic needs. These 2 overall dimensions were further classified into several domains to better capture the breadth of each dimension. Health care needs consisted of 4 domains that addressed insurance, paying for care and medicines, literacy, and access (13 items). Socioeconomic needs consisted of 5 domains addressing transportation, food, general finances, housing, and other social needs (22 items). Interviews lasted approximately 30 minutes. All participants who completed the questionnaire received a $30 retail card.
Secondary data for each participating patient were gathered from the Power Chart, which contained information on the study's outcomes of interest: disease management and health care utilization. Specifically, it identified: (1) diagnosed conditions and whether they were under “control”; (2) number of lost scheduled appointments in the last 12 months; and (3) number of visits to the emergency room (ER) in the last 12 months. For instance, a patient with diabetes was considered to be “controlled” when her or his A1c level was <7.0%. For disease management and health care utilization, other indicators for considering a patient controlled included whether the patient missed scheduled appointments at either the Care One clinic or at the diabetes management clinic. Likewise, a patient with cardiac issues was considered to be controlled when she or he consistently went to either the Care One clinic or the cardiology clinic and was able to stay out of the hospital for at least 24 consecutive months. The information was compiled and confirmed by the clinic's primary care provider.
All data were entered into REDCap (Research Electronic Data Capture), a secure web application for building and managing online surveys and databases hosted at the UNM HSC. An independent researcher validated the original data entry by cross-checking all cases and values. Data for analysis were exported into SAS 9.4 (SAS Institute Inc., Cary, NC). To facilitate the analysis, each domain under the health care and socioeconomic needs dimensions was converted into a binary variable. Thus, each domain variable indicates whether the need was met (yes) or not met (no). Similarly, all 3 outcomes of interest (condition 1, 2, or 3 controlled; lost appointment; ER visit) were computed as binary yes/no variables. Finally, the binary outcome (not met vs. met) for each domain were constructed as a profile of the percentage of respondents not meeting a domain plotted vs. each of the 3 outcomes of interest computed as a categorical variable.
Analysis included descriptive statistics, t test for continuous variables, and Fisher exact test for categorical variables and small sample size. Data also were explored as the profile of the percent of participants (dependent variable) reporting unmet (vs. met) health care and socioeconomic needs (independent variables), with each of the 3 outcome indicators (condition 1, 2, or 3 not controlled; lost appointment; ER visit) as a factor. Overall P values for each of the 3 profiles were computed by a 2-way analysis of variance (ANOVA) with a categorical factor for health care and socioeconomic variables and a binary factor for the 3 outcome indicators.
Results
A total of 60 patients were recruited. Of those, 12 were first-time patients. Because a key outcome variable in this study was whether diagnosed conditions were under control (perhaps as a result of ongoing intensive care), only established patients were included in the analysis (n = 48). Demographics are presented in Table 1. Most were male, Hispanic, born in the United States, and had a high school education. Mean age was 57.3 years, and income level very low. Type 2 diabetes, heart disease, hypertension, and depression were the most frequently diagnosed conditions. Of the 48 patients analyzed, 28 (58%) had all 3 major conditions under control and 20 patients (42%) had at least 1 condition not controlled.
Mean ± standard deviation.
Associations between demographics and the 3 outcomes of interest were explored. Sex and ethnicity were the only 2 variables that yielded significant differences (P ≤ 0.01). Females were more likely than males to have visited the ER in the past 12 months. Similarly, Hispanic/Latino patients were more likely to have a condition not controlled compared to “other” ethnicity (Table 2).
Significantly different by Fisher exact test (shaded gray figures).
ER, emergency room; SD, standard deviation.
Regarding social needs, financial, including lack of economic resources to pay for health care and housing, and lack of transportation were the 2 unmet needs mentioned most frequently. Those who reported having unmet transportation needs were more likely to have a condition uncontrolled and to have lost medical appointments compared to those who had this social need met (P ≤ 0.05). Statistically significant differences in terms of missing medical appointments also were found between those whose overall financial and housing needs were unmet and those who had those needs met (P ≤ 0.05) (Table 3).
Significantly different by Fisher exact test (shaded gray figures).
ER, emergency room.
Figure 1 represents the profiles of the percentage of participants reporting unmet needs for each of the 3 outcomes of interest. This is a graphic presentation of the 2-way ANOVA that tested for overall differences across the individual domains, and reflects the values in Table 3.
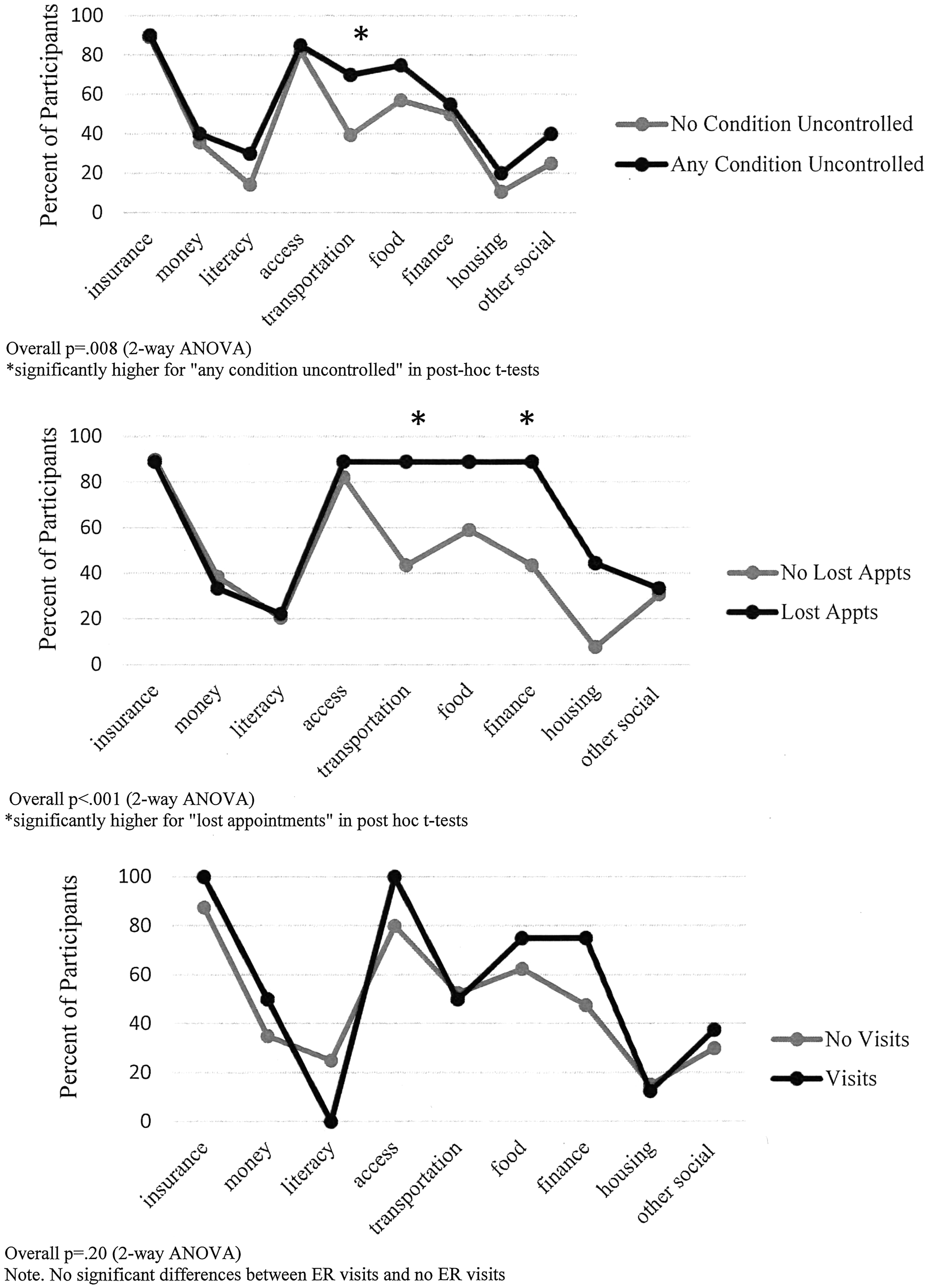
Unmet socioeconomic needs 2-way analysis of variance. ANOVA, analysis of variance; ER, emergency room.
Discussion
A prior study found the UNM HSC Care One program to be cost-effective. 30 The results of the present study seem to support the approach and the dedicated care that complex patients receive in this specialized clinic.
Compared to the overall demographics of the Care One clinic, participants in this study were slightly older (1.5-year difference) and Hispanics/Latinos were overrepresented (65% vs. 50%). Household income indicates a low socioeconomic group, for whom unmet social needs may be more prevalent. Some demographic variables and unmet socioeconomic needs were significantly related to health status and health care outcomes. These include sex and ethnicity; and transportation, financial, and household needs. This is consistent with the literature. Studies have attributed social and economic factors to poor health outcomes, 6,31 including financial 32,33 and nonfinancial barriers. 34
Results indicate that the majority of participants were effectively controlling their conditions independently of whether they experience social and financial needs. Nearly 60% of the participants had all 3 conditions under control. This suggests that dedicated care and socioeconomic support may facilitate better health outcomes in patients with complex medical conditions and unmet needs. To further address disparities in disease management and health care utilization, the Care One program should consider additional efforts toward Hispanic/Latino female patients with unmet transportation, financial, and household needs. This is particularly relevant in New Mexico, where the Hispanic/Latino population is one of the highest in the country and many people reside in rural, isolated areas that are economically deprived and lack adequate infrastructure and resources. Toward this end, a recommended approach is to develop cross-sectorial community partnerships that connect health care providers with community-based organizations with programs that address the social needs of patients. However, a recent systematic review concluded that there is no evidence of the effect of these programs on health care utilization and health outcomes as evaluation studies have to date focused “…primarily on process and social outcomes and are often limited by poor study quality.” 35 Future research should address these limitations, and perhaps develop strategies that properly overcome the challenges that, according to a Commonwealth Fund study, may hinder cross-sectorial community partnerships. 36 These include difficulties in sustaining the program and providing evidence of return on investment for both the health care and social services providers.
Regarding transportation, studies have found that the transportation system is essential to health care, 17 particularly in rural areas, and that lack of transportation is a major barrier to proper management of chronic conditions. 37,38 It has been reported that more than 3.6 million people in the United States miss nonemergency or needed medical care because of lack of transportation. 39 Nonemergency medical transportation has been suggested as a viable alternative to improve access to health care in certain groups, including vulnerable populations. 40 Although the present study did not analyze specific transportation alternatives, a previous study in southern New Mexico concluded that a bus system would have major impacts on resident's health through improved access to health care and economic opportunities. 41 Although most metropolitan areas, including the city of Albuquerque where the present study was conducted, would have a transportation system, access for chronically ill patients may be difficult. In New Mexico, both rural areas that lack public transportation as well as metropolitan areas in which the system is not convenient to chronically ill patients would benefit from an efficient and reliable nonmedical transportation system.
Limitations
This was a nonexperimental pilot study. Therefore, causal relationships cannot be established. Sample size was small and based on the study's purpose and resources (the study was funded through a very small pilot grant). Thus, generalizations should be made cautiously. Results may apply only to the participating clinic and patients. Although the questionnaire was facilitated by a trained member of the research team, it was self-reported and biases related to previous experience, misunderstanding, and social desirability are possible.
Conclusion
The UNM HSC Care One Program was established in 2004. Previous research yielded positive results in terms of reducing health care costs. The results of the present study support current literature recommending health care to address patients' socioeconomic needs in order to facilitate better utilization and health outcomes. Funding should be dedicated to further explore how health care may properly address patients' income and transportation needs, particularly among certain population groups. Although further research implementing an experimental design is needed to confirm the preliminary results reported by the present study, the Care One model may be considered for adoption throughout New Mexico and nationally.
Footnotes
Acknowledgments
We wish to acknowledge the assistance of the Care One team (Kathleen Atencio, Obdulia Arenivar, Davy Lovato, and Rosalva Andrade) without whose assistance this project would not have been possible.
Author Disclosure Statement
The authors declare that there are no conflicts of interest. This project was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences of the National Institutes of Health through grant number UL1TR001449.