
Abstract
The objective was to assess whether a Comprehensive Wellness Assessment (CWA) is associated with reduced emergency department (ED) visits for Special Needs Program (SNP) enrollees with diabetes. This retrospective panel study used a Medicare Advantage plan's administrative claims data for 2010–2017 and pooled member-month observations. Multivariate regression and individual fixed-effects regression models were estimated. The outcome was ED visits measured as binary and continuous outcomes. Data were derived from claims data that included at least 1 ICD-9 or 10 code between January 2010 and December 2017. Regression results indicated that SNP enrollees completing a CWA was associated with a lower probability of any monthly ED use (β = -0.005, t-stat = -2.98) and fewer monthly visits (β = -0.008, t-stat = -2.95). Individual fixed-effects models also demonstrated a significant decline in SNP ED use after a CWA, though the strongest effects were confined to the first 4 months after a CWA. Care models with components such as CWAs may contribute an additional benefit in the form of a reduction in ED utilization. Completing a CWA appears to be effective in reducing ED utilization among SNP members with diabetes.
Introduction
Reducing avoidable emergency department (ED) use is a major priority for organizations seeking to control waste and inefficiency in the health care delivery system. According to the Centers for Disease Control and Prevention (CDC), there were 141.4 million ED visits in 2014, which represents a 10 million visit increase from 2013. Almost 22% of Americans ages 65 and older had at least 1 ED visit in 2015, while 1 in 10 Americans aged 75 and older had at least 2 ED visits. 1 –3
This study seeks to expand on previous research to determine if a Comprehensive Wellness Assessment (CWA) program was producing additional benefits related to an overall decrease in health care costs, specifically as it related to ED use by the Medicare Advantage (MA) plan's most vulnerable population - the dual eligible Special Needs Program (SNP) enrollees. These members are eligible for both Medicare and Medicaid. They are disproportionately members of racial or ethnic minority groups with low socioeconomic status (SES) and subject to many disparities in health access, health literacy, and health outcomes. Additionally, they face barriers accessing primary care services, which in turn can increase the risk of potentially preventable hospitalizations and ED visits. Dual eligibles continue to capture the attention of health care policy makers at both the federal and state levels because delivery of care for this population creates unique challenges on many fronts. One study suggests that delivery of care in clinical settings such as Federally Qualified Health Centers can reduce preventable hospitalizations for some dual eligibles but the authors indicate that further efforts are needed to understand how to reduce preventable ED visits. 4
MA plans employ a variety of initiatives designed to target high-risk members for population health interventions. One plan, Peoples Health in Louisiana, implemented a CWA program in 2014 that was designed to improve member engagement and health outcomes primarily, although not exclusively, for SNP enrollees. Prior research found that a CWA improved medication adherence among SNP enrollees diagnosed with diabetes. 5,6 The present study builds on that by analyzing whether a CWA also is associated with reduced ED visits among SNP enrollees with diabetes.
Peoples Health is a medium-size MA plan in Louisiana with approximately 60,000 members, 31.7% of whom are diagnosed with diabetes and approximately 30% of whom are dual eligibles enrolled in the organization's SNP.
In 2014, Peoples Health adopted a population health approach to care management. One element of that strategy was to reengineer a traditional medical management/utilization review program into a model of care focused on patient-centered care coordination that includes a CWA offered annually to its members. The CWA provides an opportunity for members to have a face-to-face, unhurried discussion with a nurse practitioner (NP), addressing questions and concerns about their health status, beliefs, and health preferences.
For all enrollees who participate, the main element of the CWA is an annual 1-hour in-person evaluation performed by an NP. The CWA is intended to give members an opportunity to participate in an extensive visit with a goal of improving self-management and member engagement – both of which ultimately could improve outcomes. As part of the scheduling process, 5 attempts are made during the year to schedule enrollees. The success rate has been approximately 50% for the overall population and 66.3% for SNP enrollees. Assessments are designed to accommodate a member at a location where the member is most comfortable. This could be in the member's home, her/his primary care physician's office, or one of the organization's regional service center locations. One key component of the organization's CWA visit includes the completion of a Health Risk Assessment (HRA), which identifies not only medical conditions, but concentrates on the sociodemographic, functional status and behavioral health issues as self-reported by the enrollee. The visit also includes a complete medication review, education on the importance of medication adherence, and evaluation of the enrollee's adherence to treatment regimens. The assessment affords the enrollee an opportunity to speak with a licensed clinical social worker and a clinical pharmacist, depending on the enrollee's conditions.
The organization also has developed an internal tool that captures the past 3 years of activity for the enrollee, including ED, primary care, and specialty office visits. The tool also displays the member's compliance with recommended preventive screening studies for the preceding 3 years and is available to the NP during the member encounter.
This extensive focus affords the NP time to educate the enrollee on multiple issues related to his/her chronic conditions and optimal ways to manage them, including health care utilization and primary care relationships. The ultimate goal of the CWA visit is to increase the enrollee's ability to make informed decisions regarding his/her health care and to improve patient self-management. The organization believed that the CWA would be particularly beneficial to SNP members because their low SES makes them more likely to have been uninsured during their adulthood, to have less health literacy, to have less experience with appropriate use of health care services, and to be less informed about how to do effective self-management of health issues. Hence, although the CWA is offered to all enrollees, the organization prioritizes SNP members for CWA visits early in the enrollment year. The CWA face-to-face visit is conducted in addition to an annual interdisciplinary care team review for the dual eligible population, which is a Centers for Medicare & Medicaid Services regulated activity, and is conducted telephonically to develop the annual care plan and set goals for these members.
As mentioned earlier, previous research established that a CWA improved medication adherence among SNP enrollees diagnosed with diabetes. 5 More recently, the organization sought to determine if the CWA program was producing additional benefits such as a reduction in ED use among SNP members. Extant research indicates that low SES patients are twice as likely as high SES patients to use ED visits 7 ; thus, it is of particular interest to explore whether a population health intervention such as CWAs reduces ED use for patients. Specifically, given prior evidence of CWAs being associated with improved medication adherence among the dual eligible members in the diabetes population, it was hypothesized that CWAs may be associated with reduced ED visits for this same population. The hypothesis is motivated by prior research that suggests that being medication adherent can be associated with fewer ED visits among patients with diabetes. 8 –10 Another study by Fan et al shows that being enrolled in Medicaid managed care is associated with lower probability of having any ED visits. 11
Methods
For this follow-up analysis, the authors utilized the same general approach as used in their previous work with this population. 5 To obtain more robust estimates of the impact of the CWA as the program became well established, the study team expanded the original data set to include January 2012 through December 2017. The data set was derived from Peoples Health administrative claims data. Using those claims data, a “new to diabetes” data set was created that included distinct members whose first definitive diagnosis of diabetes derived from claims data, with at least 1 International Classification of Diseases, Ninth or Tenth Revision code, and occurred as an enrollee in the plan between January of 2010 and December of 2017. 5,6 The Institutional Review Board of the University of Alabama at Birmingham considered this to be non-human subjects research.
Statistical approach
This retrospective panel study was based on the organization's administrative claims data and pooled member-month observations. The hypothesis of interest for this study is whether SNP members who received a CWA have reductions in ED visits. Multivariate regressions of the following form were estimated to test the key hypothesis:
This model is somewhat similar to the difference-in-difference model widely used in health services research. EDimt is ED use for members in month m year t; CWAimt is a binary indicator for whether the member had a CWA in the past 12 months, and SNPimt is a binary indicator for whether the member is an SNP enrollee. Thus, β1 captures the average association of CWA with ED visits for all members, β2 captures average differences in ED visits between SNP and non-SNP enrollees in the absence of CWA, and β3 – the coefficient of the interaction between SNP and CWA – captures the information that is of primary interest – namely whether SNP enrollees with a CWA have reduced ED visits compared to their counterparts.
Ximt is a vector of the other member characteristics described in the following. Mm is a vector of month-level dummies to capture seasonal variation in ED use, and Tt is a vector of year-level dummies to capture broad changes in ED use for all members over time. eist is the error term, clustered to account for repeat observations from each member in the data set. Monthly ED use is operationalized in 2 separate ways. The first is a binary indicator for whether the member had any ED visits in a given month, and the second is the actual number of times in a month the member had an ED visit. CWA is a binary indicator showing whether or not the member had a CWA within the past 12 months. Other member characteristics are sex (1 if female); race (1 if minority); age in years; binary indicators for each of the following chronic conditions: end-stage renal disease (ESRD), chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), cancer, hypertension, and chronic kidney disease; and the number of acute inpatient and observation days in that month.
To account for the possibility that the impact of receiving a CWA may not remain constant for the following 12 months, the study team also estimated an extension of this model whereby the CWA variable was replaced by a vector of 3 variables: CWA within the last 4 months, CWA in the last 5–8 months, and CWA in the last 9–12 months (with the reference group being no CWA in the past 12 months).
The team further estimated the aforementioned models using member fixed effects. These models essentially control for baseline variation in observed and unobserved member characteristics that may be correlated with their ED use and be correlated with them electing to have a CWA. Results can be interpreted as the estimate of the average change in the same individual's ED use when he/she receives a CWA in the past 12 months versus when he/she does not.
Linear probability models (LPMs) are used when the outcome is binary – any ED visits versus none. LPMs are preferred over logistic models because they allow for a more straightforward interpretation of the coefficient of the interaction between SNP and CWA and are more adaptable to the use of individual fixed effects than logits.
STATA statistical software, version 14 (StataCorp LLC, College Station, TX) was used for all analyses. For all regression models, α = 0.05 was used to determine statistical significance.
Results
Figure 1 shows that in 2012, 5.8% of member-month observations for SNP enrollees had a CWA in the last 12 months. This number rose to 20.7% in 2013, and then consistently stayed above 60% in the succeeding years. For non-SNP enrollees, there is a similar pattern of increase, though their rates of CWAs are always lower than SNP enrollees.
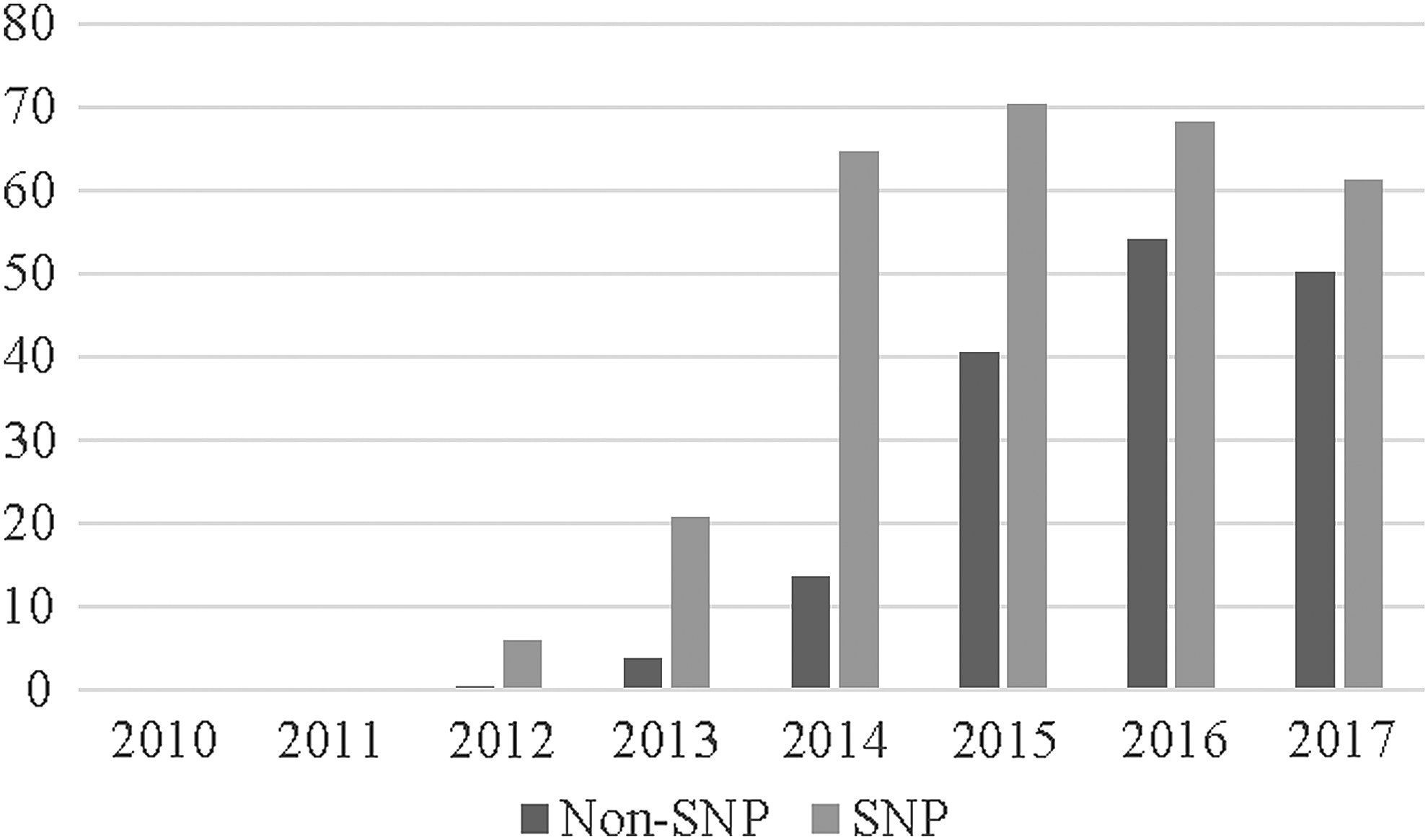
Percentage of members with a comprehensive wellness assessment. SNP, special needs program.
Table 1 presents descriptive statistics using pooled member-month observations for the years in the analyses. SNP enrollees are more than twice as likely as non-SNP members to have an ED visit in a typical month (6.89% probability versus 3.2% probability), and greater number of visits per month (0.087 versus 0.039). SNP enrollees also have more inpatient days and observation days per month, are more likely to be female, more likely to be a minority, to be younger, and more likely to have a diagnosis of ESRD, COPD and CHF. Finally, as evidenced by Figure 1, SNP enrollees are more likely to report a CWA in past 12 months than their non-SNP counterparts (60% versus 34%).
Descriptive Statistics for Special Needs Program & Non-Special Needs Program Enrollees
Non-SNP: N = 413,970 pooled member months.
SNP: N = 201,869 pooled member months.
CWA, comprehensive wellness assessment; ED, emergency department; OBS, observation; SD, standard deviation; SNP, special needs program.
Regression results in Table 2 support the main hypothesis that SNP members who received a CWA have lower ED usage. Specifically, (SNPimt x CWAimt) is associated with a lower probability of any monthly ED use by 0.5 percentage points (P < 0.01), and a reduction in monthly visits by 0.008 on average (P < 0.01). Notably, SNP enrollees per se are more likely to have any ED visits by approximately 3 percentage points (P < 0.01) and also a 0.04 higher number of monthly visits on average than their non-SNP counterparts. Thus, the reduction of 0.005 percentage points in the probability of any ED visits, and the reduction of 0.008 in number of ED visits essentially translates to a 16.67% reduction in the gap in probability of any use per month, and a 20% reduction in the gap in monthly number of visits between SNP and non-SNP members. Further, based on sample means (Table 1), the 0.005 percentage point decline and 0.008 number of visits decline translate to 7.2% and 9% reductions, respectively, in any monthly ED use and the number of monthly visits among SNP enrollees overall.
Multivariate Regression Results with Comprehensive Wellness Assessment in the Past 12 Months
CWA, comprehensive wellness assessment; ED, emergency department; OBS, observation; SNP, special needs program.
Predicted probabilities generated from the LPM regressions were within the [0, 1] boundary for 99.2% of all observations, with less than 0.8 lying outside. Therefore, the use of LPM models for these data is supported.
Results in Table 3 show that when having a CWA in the past 12 months is replaced by indicators for CWA within the past 4 months, 5–8 months, and 9–12 months (reference category being no CWA in the last 12 months), the interaction of SNP with these indicators continues to be negatively and significantly associated with ED use in all cases.
Multivariate Regression Results with Months Since Last Comprehensive Wellness Assessment
CWA, comprehensive wellness assessment; ED, emergency department; OBS, observation; SNP, special needs program.
Results from the individual fixed effects regression models are presented in Tables 4 and 5. Because individual fixed effects account for measured and unmeasured time-invariant member characteristics, sex and minority status now drop out of the model. The interaction of SNP and CWA in the last 12 months continues to be significantly associated with a reduced likelihood of any ED visits (β = −0.004, P < 0.05) and falls only marginally short of significance at 5% for number of ED visits. These results support the hypothesis that having a CWA reduces ED utilization for SNP enrollees. SNP enrollees who have a CWA on average show a reduction in ED utilization compared to SNP enrollees who do not have such a visit. However, individual fixed effects results also indicate that the effect is strongly significant in the first 4 months after the CWA, but less significant statistically for months 5 through 8 and months 9 through 12.
Individual Fixed Effects Regression Results with a Comprehensive Wellness Assessment in the Past 12 Months
CWA, comprehensive wellness assessment; ED, emergency department; OBS, observation; SNP, special needs program.
Individual Fixed Effects Regression Results with Months Since the Last Comprehensive Wellness Assessment
CWA, comprehensive wellness assessment; ED, emergency department; OBS, observation; SNP, special needs program.
Discussion
Efforts to improve health outcomes in the United States have incorporated several strategies that align closely with the Institute of Healthcare Improvement's Triple Aim to promote better care, reduce the cost of care, and improve the health of people and their communities. The Medicare annual wellness exam (AWE) and the completion of an annual HRA are 2 strategies – a direct result of the Affordable Care Act – intended to address these goals and to improve care for Medicare beneficiaries.
Prior research has shown that use of the AWE rose from about 7% in 2011 to 20% in 2016, with urban rates exceeding rural rates by 60%. Beneficiaries who did not receive an AWE were less likely to receive any of the screening services when compared to those who completed an AWE – 63% vs. 88%. 12
In addition to completing preventive screenings through the AWE, the HRA affords the provider the opportunity to assess patients' confidence in becoming actively engaged in their health care. Additional research that involved a survey of respondents from 2 separate organizations about HRA value, motivational influence, and ability to initiate a behavior change, demonstrated that 6 months after the completion of an HRA, 69% and 63% respondents, respectively, reported attempting a behavior change. 13,14
Finally, results from a randomized controlled trial with low-income geriatric enrollees enrolled in Wishard Health Services found that, compared to the control group receiving usual care, patients who received a comprehensive in-home assessment – which subsequently was used to build a tailored care plan – had better outcomes both in terms of more preventive care such as flu shots as well as fewer inpatient admissions. 15
The MA plan in this study has developed a CWA that includes an extensive HRA, complete medication review, complete review of systems, and documentation of all members' chronic conditions as well as other elements of the Medicare AWE. Administrative claims data from this organization demonstrate that SNP members utilize the ED at a significantly higher rate than the non-SNP population and the majority of the organization's inpatient admissions originate with an ED visit.
The design of the length of the CWA visit (1 hour) is intended to give the NP an opportunity to address all clinical and social issues with the member, with the goal being to effect behavior change, and to connect the member with her/his primary care physician in a meaningful way, resulting in a reduction in unnecessary health care utilization. As stated previously, prior research involving this MA organization indicated that having a CWA was associated with improved oral diabetes medication adherence among SNP enrollees, 5,6 hence motivating this current research to investigate whether CWAs were associated with lower ED use for the same population.
Poor adherence to treatment regimens has long been recognized as a substantial roadblock to achieving better outcomes for members, resulting in more than $100 billion spent annually on avoidable health care costs. 16 –19 Present study results confirmed that SNP enrollees had higher mean ED visits than non-SNP enrollees. Results of this study revealed that there were statistically significant declines of a non-trivial magnitude in ED use among SNP enrollees and that these findings persisted even after controlling for time invariant characteristics that could drive selection into having a CWA. Also, notably, these results were largely limited to the SNP population, with little indication that a CWA had any association with ED visits among non-SNP enrollees. This result reaffirms prior findings on medication adherence. The study team speculates that, because CWAs are designed to mitigate certain barriers to appropriate health care utilization (eg, poor communication, relationship between patient and caregiver, lack of understanding/awareness of the patient's lifestyle), they are disproportionately likely to benefit patients for whom such barriers are more severe. Additionally, data collected during the CWA afford the organization the opportunity to conduct future research on clinical and nonclinical aspects of wellness, such as retinal eye exam compliance for the population with diabetes and improved rates of glucose control. The team's future research will examine the effect of a CWA on additional variables not addressed in this or previous papers, such as inpatient admissions or diabetes vision screening.
Although most health care practitioners believe that CWAs are beneficial for patients, there is little consensus about their impact on an organization's bottom line. Health care purists make a forceful case for the merits of a CWA and the fiscally minded demand proof of merit in terms of improving the bottom line. One way to lend legitimacy to the CWA merit debate is to conduct a robust analysis to determine sustainability over time, implications on resource utilization, as well as overall return on investment.
The CWA represents a vital resource in the bid to effectively manage the care of MA plan enrollees. When a managed care organization commits to a resource-intensive strategy such as a CWA, it does so in the belief that the benefits can be summed up in terms of a healthier population and cost reductions. This study reaffirms that aspiration by providing additional insight into the overall effectiveness and cost benefit of programs such as the CWA.
Limitations
This study has several limitations. The focus is on ED visits but not on stratification based on the acuity of the visits. The sample was confined to enrollees who have been with the plan for at least 5 years and may not be generalized to members who stay for shorter periods. Individual fixed effects may not account for all time-varying unobservables that drive self-selection into participating in a CWA and thus some caution must be exercised when making causal inferences. The study is not able to provide more granular information on what components of a CWA are most helpful, or variations in the quality of a CWA. For example, it can be conjectured that a CWA might offer other intangible benefits such as a feeling of confidence regarding the state of one's health, but this study could not investigate whether that was a pathway by which CWAs influenced ED visits. Finally, these results pertain to one MA plan in the southeast, and the results may not be generalized across all MA plans.
Conclusion
In summary, this study aimed to build on previous research that demonstrated the value of a CWA on improved medication adherence among the population with diabetes of a MA plan in Louisiana. Additional findings from this research indicate that the completion of a CWA appears to be an effective method to reduce ED utilization among dual eligible members with diabetes in this study sample. Thus, this study provides important information on reducing ED utilization in a dual eligible population with a chronic condition.
Footnotes
Author Disclosure Statement
The authors declared the following potential conflicts of interest: Dr. Guerard is employed at Peoples Health; Drs. Omachonu and Sen have independent contractor agreements with Peoples Health. The authors received no financial support for this article.