
Abstract
There is an association between food insecurity, poor health outcomes, and increased health care spending. The Temple Food Insecurity Program was initiated to screen patients for food insecurity as part of the post Temple University Hospital discharge process. The community is economically challenged and food insecurity is a significant problem. Food insecure patients were identified and referred to community-based resources, with a 30-day follow-up call. Screening was successful in 3655 patients, 27% (n = 987) of whom reported food insecurity. Of these patients, 66% (n = 647) were already receiving benefits through the Supplemental Nutrition Assistance Program (SNAP), but were still food insecure. All patients with food insecurity were referred to one of 2 resources for help. Despite significant need, less than a quarter of patients connected with these resources. Qualitative data revealed that some patients did not remember the information provided to them, were overwhelmed with poor health or other social determinants of health, had competing priorities, did not perceive the need for food assistance; and experienced system barriers. Health literacy also was an issue. Health care systems addressing food insecurity should consider the high prevalence of food insecurity in impoverished regions, the reality that SNAP benefits may not alleviate food insecurity for many patients, and the need for individualized, custom care plans that address barriers and reflect patient priorities and capabilities. Engaging patients differently may be aided by additional communication from community food resources directly to patients who provide permission for this added service.
Food insecurity – the lack of accessible and affordable nutritious food – is a major population health issue in the United States. In 2016, 12.3% of households reported being unable to acquire enough food to meet the needs of all their members because of insufficient money or other resources for food. 1 The association between food insecurity and negative mental and physical health outcomes is well documented, including higher incidence of obesity, chronic diseases, and mental health disorders. 2 Poor health translates to higher health care costs, with health-related costs attributable to food insecurity estimated at $77.5 billion dollars annually. 3
As health care transitions from pay for performance to a value-based system, health care organizations are engaging in strategies to improve the health of the communities they serve. These efforts include screening for and addressing food insecurity. The approach to this work is challenging given the limited number of published studies on effective strategies to address food insecurity and the need for new protocols, relationships, and system changes that are required to integrate care with community-based resources. In response to the problem of food insecurity identified by the Temple University Hospital (TUH) 2016 Community Health Needs Assessment, the Temple Center for Population Health (TCPH) launched the Temple Food Insecurity Program (TFIP), including screening recently discharged adult patients for food insecurity, and providing referrals to community-based food resources when needed. TFIP was part of a citywide initiative to address nutritional food access for at-risk patients, consisting of 9 health systems, community-based organizations, health plans, and public service agencies in the Philadelphia area. The program, facilitated by the Hospital Association of Pennsylvania and convened by the Healthcare Improvement Foundation, was the inaugural COACH (Collaborative Opportunities to Advance Community Health) program.
This study was designed to evaluate the effectiveness of TFIP on 3 parameters: number of patients screened for food insecurity, number of patients referred to appropriate food resources, and the rate of follow-up after a referral was made. The study proposal was submitted to the Temple University Institutional Review Board and was determined to be quality improvement as the results are being used to inform program redesign.
Methods
This was a prospective emergent mixed-methods study design with 2 study strands: quantitative and qualitative. The qualitative strand of the study was added while collecting quantitative data to better understand the low rate of patients connecting to community resources. The 2 strands were designed as separate inquiries with the results mixed together during data interpretation to enhance quantitative findings. 4
Setting
Temple University Health System (TUHS) is located in North Philadelphia, providing care for an ethnically and racially diverse population, with 67% of the residents living in poverty, 20% unemployed, and 23% with less than a high school education. 5 Screening for food insecurity was integrated into the routine postdischarge follow-up call process conducted by TCPH community health workers (CHWs) within the Hospital Access Center for patients who were hospitalized in TUH.
Sample
The quantitative strand of the study was a convenience sample of adult patients aged 18 years and older who were contacted within 48–72 hours following discharge from an inpatient hospital stay at TUH as part of the routine care for postdischarge patients.
A purposeful typical case sampling method was used for the qualitative strand, focused on a homogenous group of patients representing the usual patient encounter. 6 For this study, sample selection criteria included patients who were between the ages of 33 to 69 (mean ±1 standard deviation), African American, of mixed race, or Hispanic (80% of the population), and lived in the 11 zip codes surrounding TUHS. Deviant case sampling was used to identify challenges outside of those expressed in the selected patient sample.
Procedures
The postdischarge calls included screening for food insecurity using the 2-item Hunger Vital Sign™ tool that has been validated to screen for food insecurity in children and families. 7 The questions are: (1) In the past 12 months, have you worried whether your food would run out before you got money to buy more? and (2) Within the past 12 months, has the food you bought just not lasted and you didn't have money to buy more? A positive response to either question indicated food insecurity. Patients who reported food insecurity were asked a probing question to determine if they were already receiving food benefits through the Supplemental Nutrition Assistance Program (SNAP). Their response to this question determined which of the community resources they would be referred to: The Greater Philadelphia Coalition Against Hunger (CAH) for those who needed to apply for SNAP benefits, and 2-1-1 South Eastern Pennsylvania (SEPA) if additional food resources were needed. These 2 community agencies were selected to participate in TFIP because they were part of the citywide COACH initiative. CAH is a citywide organization that connects people with food assistance programs and nutrition education, provides resources to a network of food pantries, and educates the public and policy makers about responsible solutions to prevent people from going hungry. 2-1-1 SEPA is part of the national 2-1-1 Call Centers initiative that provides a web resource for finding health and human services for everyday needs, including food, as well as in crisis situations. A follow-up call was made (with permission) after 30 days to assess if patients connected with the food resources recommended to them. Patient responses were documented in the Midas Care Management system (Conduent, Inc., Florham Park, NJ), a secure patient folder used by the CHWs who conducted the calls. Program processes are detailed in Figure 1.
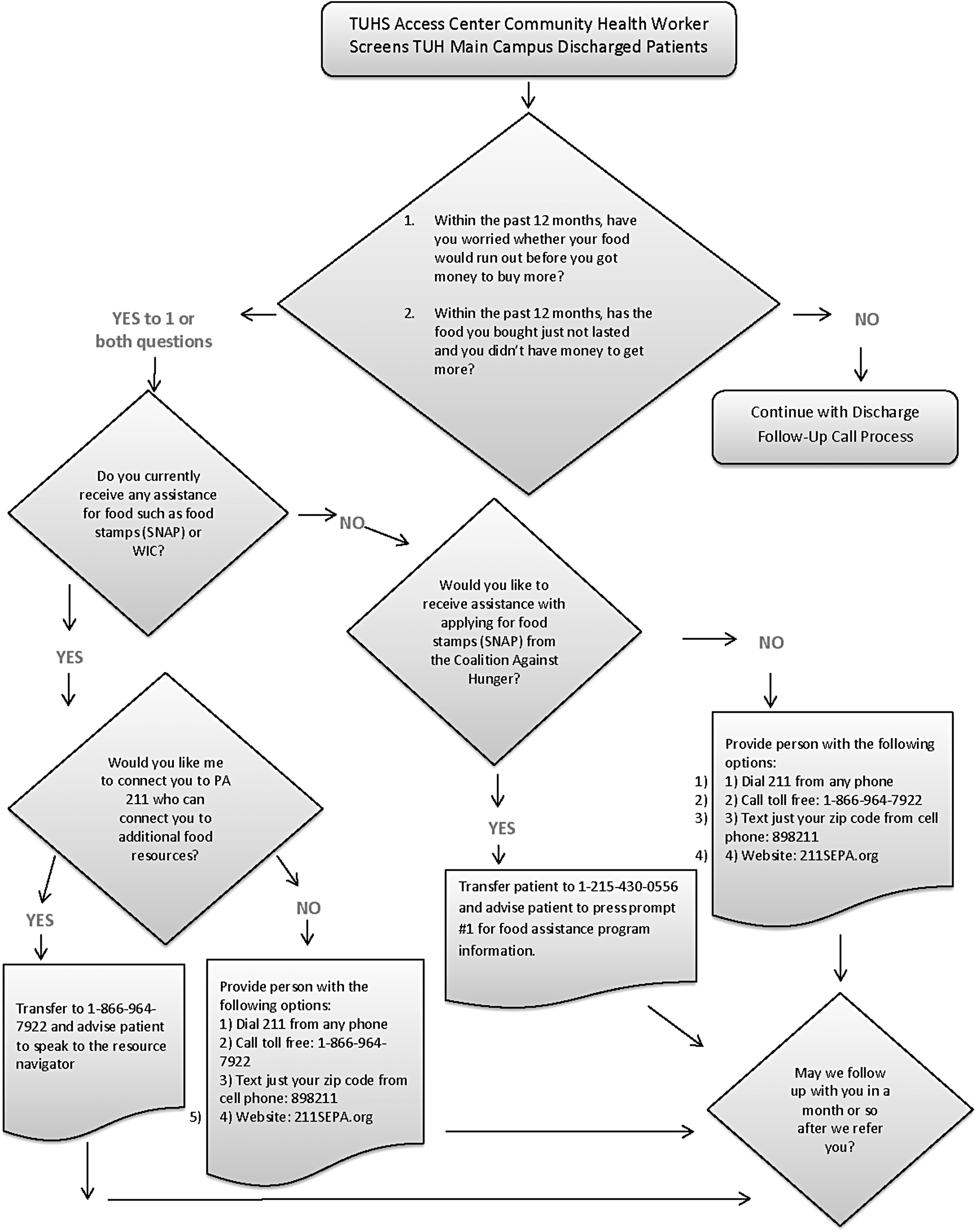
Food insecurity screening workflow. SNAP, Supplemental Nutrition Assistance Program; TUH, Temple University Hospital; TUHS, Temple University Health System; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Initially, patients who screened positive for food insecurity and agreed to a follow-up call were contacted by a CHW to explore if they connected with the food resources provided. The community agencies were also collecting information to determine the number of patients referred to them and who connected with their organization. Early in this process the data collected by the CHWs identified an unexpected number of patients who had not connected to these resources. It was at this point that the qualitative inquiry was added to the call to explore facilitators and barriers. Follow-up calls were conducted by a TUHS employee who also was a graduate student and familiar with qualitative methods. The employee used a script to introduce the call and obtained permission to ask a few questions. For patients who agreed to be questioned, the employee continued to explore if they connected to food resources and if they would share what helped in the process or why they did not connect to resources, depending upon the initial response. Patient responses were documented, including quotes, in an Excel sheet in a secure folder accessible only to the study team.
Data analysis
Quantitative data, including demographic information, screening responses, and follow-up with community resources, were analyzed using univariate descriptive statistics.
The qualitative analysis was guided by the following 2 theoretical frameworks: Minimally Disruptive Medicine (MDM). MDM is a patient-centered approach to health care that prioritizes patients' goals for life and health while minimizing health care disruption in patients' lives.
8
The foundation of MDM is based on the knowledge that patient self-care must compete with the demands of family, job, and community life.
9
These competing demands can be especially challenging for patients who suffer from chronic diseases that involve complex self-care demands.
10
Overwhelmed patients may not have the capacity to access care or enact self-care and thus will experience suboptimal disease outcomes.
9
Complex Responsive Processes (CRP). The theory of CRP provides a process perspective on individuals and organizations that are continuously being informed by each other. CRP is part of the Complex Systems Theories that point to the complex nature of reality and, consequently, to the innate limitations of describing systems.
11
The theorists do not consider individuals as autonomous of their environment; that is, they cannot form goals and action plans without at the same time being influenced by their environment.
12
Using this theoretical framework helps to make sense of phenomena emerging in organizational settings to understand what people do right or need to improve in system settings.
Qualitative data analysis was an iterative process, beginning as early in the project as data became available for patients who met the inclusion criteria. The analysis began with using the template organizing style, in which a few predetermined codes were developed a priori, based on prior experiences and the guiding frameworks. 6 Revisions to existing codes and the development of new codes were defined as the text was read. Two members of the project team independently coded data that later were discussed to develop an agreed-upon codebook. At the completion of coding, the team met periodically to conduct targeted analysis, first by sorting segments and then by displaying the data to discover connections. In the sorting process the codes with the most frequency were used to identify key areas for further analyses. Data collection finished when there was data saturation. Maps and matrices were then used to arrange data by themes. The final step in the analytic process was to combine the quantitative and qualitative analyses for interpretation that informed program revisions that are needed to engage patients who are food insecure. Findings were shared with the staff member who conducted the calls as a member-checking task to enhance credibility and applicability of the findings.
Results
A total of 3860 recently discharged patients were called over a 6-month period (August 2017 to January 2018). Ninety-five percent (3655) agreed to be screened for food insecurity and 205 refused screening. Overall, more than half of patients identified as being African American and more than one quarter as Hispanic (Table 1). Mean age was 52.6 (± 14 years). Gender and insurance breakdowns are available in Table 1. Seventy-eight percent of the sample lived in the 11 zip codes surrounding TUH.
Demographic Variables
SD, standard deviation.
Of those screened, 27% (n = 987) of patients were positive for food insecurity. More than two thirds of patients who were food insecure were already receiving food benefits through SNAP (Table 2). Within the food insecure group, approximately one quarter of patients did not want information on community resources, with the remaining patients referred following the TFIP care protocol. Early analysis of the data provided by the community agencies (2-1-1 SEPA and CAH) revealed that only 20% of patients referred actually received services (Table 2).
Results of Screening for Food Insecurity
CAH, Coalition Against Hunger; SNAP, Supplemental Nutrition Assistance Program.
Follow-up calls 30 days after the initial screening process were conducted between September 15, 2017, and January 31, 2018 to collect both quantitative and qualitative data. During this time, 297 calls were made to patients, connecting to 123 patients. Of these patients, only 22% (n = 27) reported connecting with a community resource. Eighty-nine patients met the study inclusion criteria as a typical case for the qualitative strand of the study. From the analysis, 5 themes emerged related to MDM – the first of the theories used – particularly related to the concept of patient capacity and how it interacted with self-care for the typical patient: (1) Did Not Remember, (2) Overwhelmed, (3) Competing Priorities, (4) Low Health Literacy, and (5) Multiple Interacting Social Determinants. Each of these themes is defined in the following sections and detailed in Table 3.
Results of Qualitative Analysis: Patient Capacity
MDM model
Did Not Remember. In a word search of documented patient responses, 20% of patients used the words “don't remember” or “don't recall” in their responses. Specifically, they did not remember the follow-up call or content of the discussion, or what they did with the food resource referral information. Patient responses under this theme did not attribute the forgetfulness to any external or internal stressors or events that may have played a role in remembering the initial follow-up call or information provided.
Overwhelmed. A subset of patients reported that poor health or other social situations interfered with their memory or ability to follow through with addressing their food insecurity. These included being rehospitalized, feeling too ill to remember or carry out the activities required to access food resources, or significant family problems.
Competing Priorities. Patients also reported having competing priorities within their complex lives. Most of these reports were related to ongoing health care problems or other social determinants of health that patients reported as more important for them to address before food insecurity.
Low Health Literacy. A subset of patients reported barriers in connecting with food resources with signs indicative of low health literacy; specifically, those who needed help filling out forms or those who were unable to understand the information provided to them.
Multiple Interacting Social Determinants. A group of patients viewed improving their food security as a priority but had problems with insufficient funds for transportation to travel to food pantries or a grocery store.
There were 3 themes related to the second guiding theory, CRP, where data were analyzed to explore the interaction of organizations and patients. These included: (1) System Elements to Promote Patient Adaptation, (2) Disconnect Between Organizations and Patient Perception of Food Insecurity, and (3) System Barriers. These themes are defined in the following sections and detailed in Table 4.
Results of Qualitative Analysis: System and Patient Interactions
CRP theory
System Elements to Promote Patient Adaptation. In general, patients who connected with community services appreciated it when the organization contacted them, and reported an improvement in their food insecurity, particularly with access to food banks. Patients who did not connect with services suggested a more proactive approach to care by having the community resources contact them to help navigate the system.
Gap Between Screening Results and Patient Perception of Food Insecurity and Need for Food Resources. Patients who screened positive for food insecurity but did not perceive they were food insecure at the time of the follow-up telephone call or that they needed assistance with food resources.
System Barriers. System barriers discussed by patients that interfered with accessing food resources included: (1) the food provided did not follow the medically recommended diet, (2) the patient scored positive for food insecurity but was ineligible for assistance, and (3) despite reaching out to community resources, the patient did not receive a follow-up call.
Data analyzed for deviant cases (n = 34) did not reveal any new information or generation of additional codes than were found with the typical case analysis. The only differences between the typical and deviant cases were based on age. Patients in the deviant case sample who were younger than 33 years of age and who did not connect with food resources only reported forgetting the information or perceived that they did not need assistance. In comparison, patients in the deviant case sample who were older than 69 years of age also reported poor health as a barrier to accessing resources and carrying out referral recommendations.
Combining the quantitative and qualitative data revealed that at the time of screening 24% of the patients did not want information on community-based food resources, and an additional 21% of patients contacted at 30-day follow-up perceived they did not need assistance with food, representing a significant proportion of patients who would not benefit from community-based assistance after discharge from the hospital. Several of the patients who did not perceive they needed assistance reported receiving food assistance from friends and family. More than half of patients reported that difficulties with navigating the community-based systems, or complexities in their health and lives, impacted their desire or capacity to follow through with referrals to food resources. These factors were confounded when patients also reported signs that indicate low health literacy. This group of patients demonstrates the challenges that must be addressed by health care providers to successfully embark on a food insecurity program.
Discussion
This study explored the outcomes of a food insecurity program for adult patients in a challenged urban population who were recently discharged from the hospital. The results revealed a higher than expected rate of food insecurity in this population and, perhaps more importantly, that SNAP benefits did not alleviate food insecurity for more than half of the food insecure patients. In addition, a subset of patients did not perceive that they needed additional food resources. Significant patient complexities and system factors negatively impacted connection with community-based food resources for more than half of patients.
Twenty-seven percent of patients screened reported food insecurity. This result is reflective of the severity of poverty in the surrounding community served by the hospital when the data are compared to a citywide incidence of 19.3%, a statewide incidence of 13.5%, and a national incidence of 12.9%. 13,14 The research team anticipated the incidence of food insecurity for this population to be similar to the city's, considering that Philadelphia is ranked as the poorest large city in the United States. 15 The team did not anticipate that 66% of those who screened positive for food insecurity would already be receiving food benefits through SNAP. However, the findings from this study are similar to those reported by the US Department of Agriculture (USDA) in 2014. That study showed that participation in SNAP for approximately 6 months was associated with a decrease in the percentage of urban households with food insecurity, but 60.7% of households remained food insecure. 16 Present study results indicate the severity of food insecurity in impoverished urban neighborhoods, how essential partnering with multiple community-based agencies is to address food insecurity for patients receiving SNAP benefits, and the important role of CHWs in helping patients access these community resources. These results also highlight the need to advocate for policy change that expands SNAP benefits.
During the qualitative inquiry, 21% of patients who screened positive for food insecurity did not perceive that they needed food assistance. For some patients, this was because support was being provided by family or friends. For others, the gap between screening results and patient perception may be a limitation of the screening tool that asks respondents to report on the last 12 months, during which time frame the problem may have been resolved. It is important to note that food insecurity has been shown to be episodic, with the inadequacy of food generally brief and often at the end of the month. 17 This pattern tends to recur frequently and over long periods of time, suggesting that using a screening tool alone does not provide the detail needed to fully understand patients' needs. A few additional patient assessment questions about their positive screening responses, assistance acquired over the past 12 months, and current need for food assistance would be helpful to develop an individualized plan of care. The use of one of the USDA's assessment tools, which categorize levels of food insecurity as marginal, low, and very low food security, also may provide helpful information. 18
The low rates of patients connecting with the food resources recorded at 2 different time points in the study led the team to explore the facilitators and barriers in this process. The findings support the MDM model that proposes that treatment plans should reflect the capacity of patients to provide self-care to minimize the burden of treatment. 8
Two themes that emerged from the qualitative data – lack of memory regarding the recommendations and referrals, and health literacy issues – reflect an opportunity to improve care transitions to support patients recently discharged from the hospital. A number of studies have identified patients not remembering or understanding their instructions during this transitional time. 19 A simple research-supported intervention, teach-back, can be used to check understanding by asking patients to state in their own words what they need to know about their care. 20 Additional navigation resources also may be required to complete the process and aid patients with complex connections.
As highlighted in the MDM model, many patients must fit self-care into their already complex lives. To achieve this patient-centered care, the MDM Care Model suggests 2 strategies: (1) identify the right care and (2) make the right care happen. 21 Given the importance of good nutrition to healing and health, addressing food insecurity is the right care. 22 To make care happen, patients were asked what would be most helpful. Patients offered suggestions for system redesign, which included shifting responsibility for outreach from the patient to the community-based organization. This push–pull technique was described by Lean methodology and has been proven to optimize process redesign. 23 Assuring compliance with privacy laws is a potential challenge in addressing this suggestion. Additionally, follow-up calls also may be considered an effective strategy to help make the right care happen, as in this program the calls identified patients who needed continued assistance with navigating the community and health systems. With a recent study showing a relationship between lower self-efficacy and higher incidence of food insecurity, patient encounters should employ tactics that target increasing self-efficacy. 24
How to identify the right care and make the right things happen also are important considerations when evaluating the themes of competing priorities and multiple interacting social determinants of health. For some patients, addressing other health issues (eg, accessing medications) takes priority over access to sufficient healthy food. For some, other social determinants of health (eg, housing, transportation) were either a priority or interfered with the ability to access available community resources. This suggests that screening for food insecurity should not be assessed independently from other social determinants of health, and asking each patient to prioritize needs will help create appropriate individual care plans.
A subset of patients reported having difficulty completing forms or understanding the instructions provided, which is indicative of low health literacy. Health literacy – the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions – has been shown to be associated with poor health outcomes, higher rates of hospitalization, and higher health care costs. 25 Populations most likely to experience low health literacy are older adults, racial and ethnic minorities, people with less than a high school degree or general equivalency diploma, people with low income levels, non-native speakers of English, and people with compromised health status – all factors that are prevalent in this study population. 26 The addition of a brief screening tool for low health literacy coupled with evidence-based strategies to address low health literacy would aide communication between health providers and patients.
This study has several limitations. First, the study was conducted at 1 health system to gain insight into how the food insecurity program could be redesigned to better meet the needs of patients. As such, it is not generalizable, but offers insight for other organizations that are addressing this social determinant of health and the patient and system barriers that should be considered as part of their program. Secondly, the quantitative strand of the study was a convenience sample of patients the study team was able to reach after discharge. As such, the selection process is biased and may not reflect the results of the entire population. Finally, patient interviews were brief, semi-structured interviews. Although the team collected informative data, subsequent studies that include in-depth discussions to elicit more information about patient experiences and perspectives are indicated.
Conclusion
Food insecurity is a serious problem in impoverished neighborhoods. Many patients continue to be food insecure despite receiving government-sponsored food supplementation, and there are system- and patient-related factors that must be addressed in order to optimize access to a sufficient amount of healthy food. Systematically addressing the social determinants of health is relatively new for most health care organizations. In this study, screening for food insecurity was easily incorporated into the hospital's postdischarge follow-up process. However, successfully linking patients to community resources often was challenging in this high-risk population. This study showed that a referral coupled with a customized action plan tailored to patients' priorities and perceived needs may produce improved results. Future research is needed to better understand which interventions within the action plan are most effective for patients and positively impact health outcomes. The specific research areas may include health systems redesign, screening for and addressing low health literacy, employing techniques to improve self-efficacy, patient navigation, and addressing other social determinants of health.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The authors received no financial support for this article.