
Abstract
Opioid use disorder (OUD) is a national crisis. Health care must achieve greater success than it has to date in helping opioid users achieve recovery. Integration of comprehensive primary care with treatment for OUD has the potential to increase care access among the substance-using population, improve outcomes, and reduce costs. However, little is known about the effectiveness of such care models. The Comprehensive Care Practice (CCP), a primary care practice located in Maryland, implemented a care model that blends buprenorphine treatment for OUD with attention to primary care needs. This study evaluates the model by comparing patients with OUD treated in CCP and other Maryland facilities in a large state Medicaid program. Compared to the non-CCP patient group (n = 867), the CCP group (n = 131) had a higher 6-month buprenorphine treatment retention rate (79% vs. 61%, adjusted average marginal effect (AME) = 0.17, P < 0.001). CCP patients also had fewer hospital stays in the 12-month follow-up period (0.22 vs. 0.41, AME = -0.17, P = 0.005), and lower total cost (US$10,942 vs. $13,097, AME = -$4554, P < 0.001) and hospital stay cost (US$1448 vs. $4265, AME = -$2609, P = 0.001), but higher buprenorphine pharmacy cost (US$3867 vs. $2781, AME = $987, P < 0.001). Other measures, including emergency department utilization and cost, substance abuse cost, and non-buprenorphine pharmacy cost, were not statistically different between the 2 groups. Results suggested that patients, as well as the health care system, can benefit from an integrated model of buprenorphine treatment and primary care for OUD with better treatment retention, fewer hospital stays, and lower costs.
Introduction
Costs related to substance use disorder in the United States have soared over the past decade with the dramatic increase in the prevalence of opioid use disorder (OUD). 1 The Centers for Disease Control and Prevention estimated that prescription OUD costs $23 billion a year. 2 Patients with OUD have high rates of concurrent chronic comorbidities contributing to cost 3,4 and the economic impact related to these patients is magnified when considering the costs associated with more than 80,000 Americans incarcerated for reasons related to OUD. 5 It is postulated that treatment of OUD saves more money for the criminal justice system than for health care. 6,7
In the past 15 years, many studies have shown the cost-effectiveness of substance use treatment. 8 –11 Both buprenorphine and methadone treatment for OUD have been shown to decrease health care expenditures. 12 –14 In a cost analysis model for Medicaid patients, the use of buprenorphine increased outpatient costs related to visits and the cost of the prescription, but was postulated to generate savings in emergency care and hospitalizations. 15 In Massachusetts, higher costs among Medicaid members with OUD were found in individuals in behavioral substance use disorder treatment without the use of buprenorphine or methadone as compared to those receiving buprenorphine or methadone. 16
There also is evidence to support the notion that integrating primary care with OUD treatment can improve care for patients with OUD. For example, the provision of medical care services in drug treatment clinics is associated with lower emergency department (ED) use. 17 Similarly, methadone maintenance patients linked to primary care have decreased ED utilization. 18
There is a dire need to address the demand for treatment of OUD, with only a minority of patients in treatment. 19,20 The Drug Addiction Treatment Act of 2000 allowed office-based treatment with buprenorphine and increased the ability of individual health care providers to treat OUD. Previously, treatment of OUD was available only in specially licensed and regulated methadone clinics. These clinics have legal barriers to fully coordinating care with patients' primary care physicians and frequently are unable to meet patients' other medical needs. Access to methadone has been and continues to be limited by insurance coverage, geographic availability, as well as strict prescribing guidelines.
Primary care is being recognized as an ideal entry point of care for individuals with substance use disorder. Historically, primary care and treatment of substance use disorder have rarely occurred in the same physical setting. The integration of care for substance use disorder into primary care has been recommended as an evidence-based goal of health care delivery, 21 as substance use disorder has been associated with increased risk for physical illness, increased mortality, and higher health care costs. 22 Compared to the general patient population, this patient group has a high prevalence of comorbid conditions, including chronic pain, hepatitis, pancreatitis, cirrhosis, and HIV. 23,24 The Affordable Care Act increased access to health care for low-income individuals through Medicaid expansion and greatly increased access to medical care for substance use disorder. 25,26 In the United States, individuals with substance use disorder are more willing to enter treatment in a primary care setting than in a specialty drug treatment center, pointing to the need to increase the availability of primary care-based substance use disorder treatment. 27 Despite the need, the provision of fully integrated care for OUD has seen limited implementation. Only 3% of primary care physicians obtain waivers from the Drug Enforcement Administration (DEA) to prescribe buprenorphine-naloxone. 28 Based on an early survey, primary care physicians in Maryland are much more willing to refer their patients to a separate substance use disorder provider for either buprenorphine or methadone treatment, rather than obtaining the DEA waiver and prescribing themselves. 29 Even in community health centers, a separate substance use disorder provider is often seen for prescribing buprenorphine.
Although integrated care is hypothesized to improve treatment outcomes of substance use disorder and comorbid medical conditions, little is known about the effectiveness of such a care model on patient outcomes, including retention rates, disease outcomes, utilization, and cost of health care services. The Comprehensive Care Practice (CCP), a primary care practice located on the campus of the Johns Hopkins Bayview Medical Center in Baltimore, Maryland, has implemented a unique care model of buprenorphine treatment for OUD in the context of primary care to enable care for all of a patient's medical problems. Preliminary assessment showed a 12-month retention rate of 57% for patients receiving buprenorphine in this model. 30 Using insurance claims data from a large Medicaid Managed Care Organization (MCO), the study team aimed to evaluate the comparative effectiveness of this integrated model by comparing outcomes of Medicaid patients with OUD treated with buprenorphine as part of integrated care at CCP versus those treated with buprenorphine elsewhere in Maryland.
Methods
CCP care model
All practitioners in CCP provide primary care with a focus on caring for patients with substance use disorders. There are 5 physicians and 1 nurse practitioner in CCP. Treatment of OUD with buprenorphine is integrated with primary care to address medical needs, including HIV, hepatitis C, hypertension, diabetes mellitus, and preventive services (eg, vaccination, screening).
The practice does not have a standardized protocol for prescribing buprenorphine. Instead, providers decide which patients to treat with buprenorphine, titrate buprenorphine dose levels, and develop care plans for office visit frequency based on patients' needs and the providers' own discretion. Typically, initiation of treatment happens in the patient's home, followed by weekly 15-minute regular office visits that focus on supportive interventions and other primary care issues patients have. In addition, CCP encourages patients to attend self-help groups and may refer them to community resources. Office visits are reduced to monthly after the condition is judged stable. Follow-up visits are more frequent for patients who continue to use illicit opioids or other substances, as evidenced by self-report or urine drug testing.
Study design and patients
This comparative effectiveness study compared patient outcomes between 2 groups of Medicaid patients: buprenorphine patients treated at CCP, and buprenorphine patients treated at other outpatient practices in Maryland. The setting of treatment for non-CCP patients was heterogeneous and included outpatient drug treatment programs and community health centers that provided buprenorphine treatment in the same setting as primary care, but most often with a separate substance use disorder provider. The study used administrative claims data from the Priority Partners MCO, one of the 7 Medicaid MCOs authorized by the State of Maryland. Priority Partners MCO is jointly owned by Johns Hopkins Healthcare LLC and the Maryland Community Health System, a group of Federally Qualified Health Centers. It is the second largest MCO in Maryland and manages approximately 25% of the Medicaid population in the state. It contracts for health care services through a statewide network of providers primarily based on fee-for-service reimbursement.
The study included adult patients aged 18–64 years who began a new episode of OUD treatment with buprenorphine between January 1, 2008, and July 31, 2012. As there was a subsequent carve-out for coverage of buprenorphine from Priority Partners MCO to a state contracted behavioral health entity starting in August, 2013, the study time frame was defined to allow for an accurate 12-month follow-up of all patients' buprenorphine prescriptions. Specifically, a new episode was defined using identification of buprenorphine prescription between January 1, 2008, and July 31, 2012 with no prior prescription of buprenorphine for 3 months. If multiple new episodes were identified for a patient, only the first one was included in the analysis. Patients in the CCP group were considered to be confirmed if a patient had an office visit with an identified CCP provider in the same month that the patient started his/her new episode of buprenorphine treatment. Other patients were assigned to the comparison group.
Outcome measures
The study examined 3 types of patient outcomes: buprenorphine treatment retention, utilization of hospital and ED services, and health care costs. Treatment retention was followed for 6 months, and utilization and costs for 12 months. Treatment retention was a yes/no dichotomous variable indicating whether a patient was still in treatment 6 months after initiation of the treatment episode during which there was no gap longer than 2 months. Health care utilization was defined by acute hospital admissions and ED visits cumulatively during the 12-month follow-up period. Health care costs were calculated from medical and pharmacy claims data and are reported by overall total cost as well as categories of cost: inpatient hospital stays, ED visits, substance use treatment cost, pharmacy costs related to buprenorphine cost prescriptions, and pharmacy costs related to other non-buprenorphine prescriptions. The study team also sourced patients' demographic variables, including age, sex, and race, from eligibility data received from the state Medicaid program. Patients' zip codes were used to link to Area Health Resource Files to obtain median household income of the county in which a patient resides. Two variables, count of chronic conditions and risk of high expenditure, were generated to represent patients' health conditions.
Statistical analysis
To compare the 2 groups, the study team first compared patient characteristics using Wilcoxon rank-sum tests for continuous variables and chi-square tests or Fisher exact tests for categorical variables. Then logistic regression models were constructed for dichotomous outcome variables (eg, treatment retention, use of acute hospital stay, ED visit), adjusting for patient demographics (ie, age, sex, race, residing in a county with median household income <US$40,000) and their health conditions (ie, count of chronic conditions, risk of high expenditure). For cost outcomes, because of their skewness, excess zeros, and multimodality, the team first examined the proportion of zeros for each cost measure, and then performed Box-Cox and Park tests to determine the appropriate link functions and models. The team used a zero-inflated negative binomial model to analyze number of acute hospital stays and number of ED visits, 2-part models for hospital stay costs and ED visit costs, and a generalized linear model (GLM) with log link for other cost measures. The 2-part models used a logit model to predict cost/no-cost and GLM with log link to predict cost amounts above zero.
For regression models comparing the 2 groups, adjusted average marginal effects (AMEs) are presented, rather than parameter estimates (ie, odds ratios, coefficients) because parameter estimates from the regression models with log link and 2-part modeling are not directly interpretable. The marginal effects are the difference in the outcome measure associated with a study subject being in one group as compared to being in the other group, holding his/her other characteristics fixed. The average of these differences across all of the study subjects is the AME.
Results
The study team identified 131 Medicaid patients in the CCP group and 867 in the non-CCP group (Table 1). On average, CCP patients had 9 months during the 12-month follow-up with at least 1 office visit at the CCP, while approximately 96% of the patients in the non-CCP group never had a visit at CCP during the 12-month follow-up. This result confirmed that the definitions for categorizing the 2 groups are appropriate.
Characteristics of the Study Groups
From chi-square tests or Fisher exact tests for categorical variables and Wilcoxon rank sum tests for continuous variables.
CCP, Comprehensive Care Practice; SD, standard deviation.
More than two thirds of study patients were female and white (Table 1). Their average age was 33.5 years with a standard deviation of 10.3 years. There were no statistical differences between the 2 groups in their age, sex, and race. However, CCP patients were likely to be sicker and poorer − more CCP patients, compared with non-CCP patients, lived in a county with a median annual household income <US$40,000 (39% vs. 23%, P < 0.001). Moreover, CCP patients on average had more chronic conditions compared to the non-CCP patients (P < 0.001). The risk of high expenditure between the 2 groups was not statistically different (P = 0.163).
Table 2 describes study outcomes with frequencies and percentages for binary variables, and means, standard deviations, medians, and interquartile ranges for count and continuous variables by study group. Figures 1 –3 provide predicted outcomes by group to display the differences visually. Compared to the non-CCP group, CCP patients were more likely to be retained in buprenorphine treatment for 6 months. The retention rate was 79% in the CCP group and 61% in the non-CCP group (AME = 0.17, P < 0.001). On average, number of acute hospital stays was lower in the CCP group during the 12-month follow-up (P = 0.005). However, the proportion of patients who had at least 1 acute hospital stay and the marginal effects of ED utilization (measured by proportion of patients with at least 1 ED visit and number of ED visits) were not statistically different between the 2 groups (Table 2).
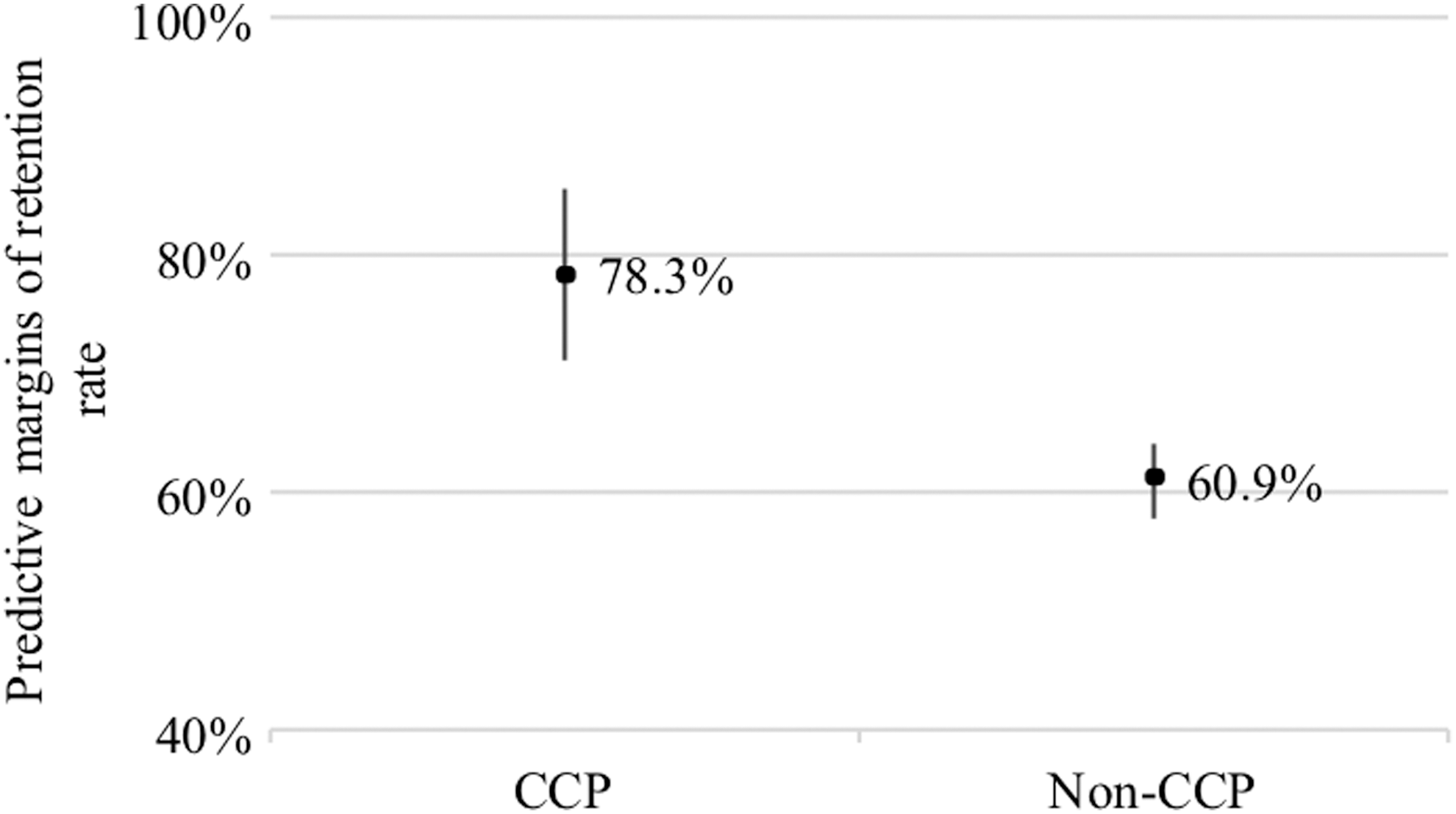
Buprenorphine treatment retention rates by Comprehensive Care Practice and Non-Comprehensive Care Practice Groups. Predictive margins with 95% confidence interval adjusted patient demographics (ie, age, sex, race, residing in a county with median household income <US$40,000) and health conditions (ie, count of chronic conditions, risk of high expenditure). CCP, Comprehensive Care Practice
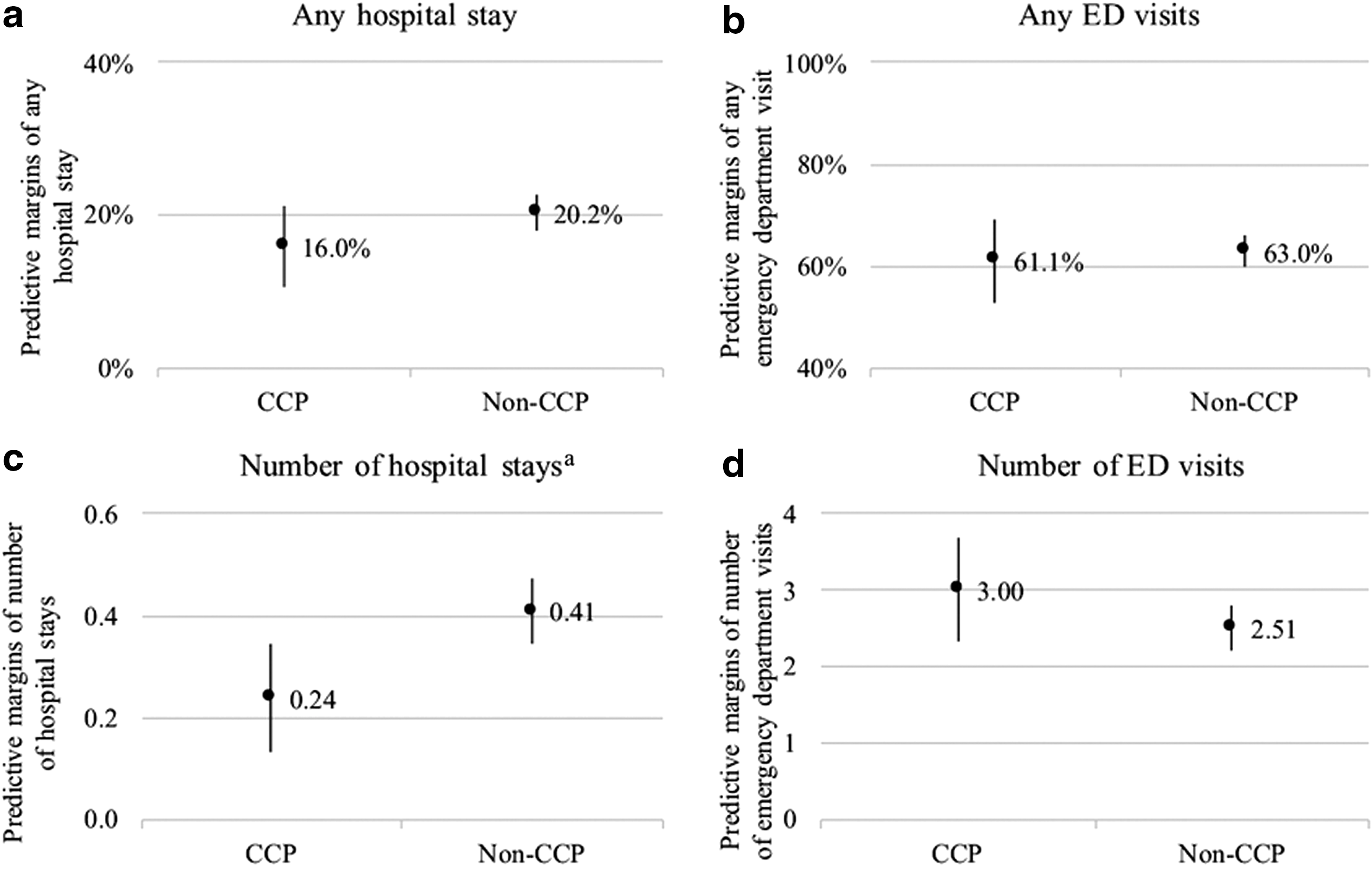
Hospital stay and emergency department utilization by Comprehensive Care Practice and Non-Comprehensive Care Practice groups. Predictive margins with 95% confidence interval adjusted patient demographics (ie, age, sex, race, residing in a county with median household income <US$40,000) and health conditions (ie, count of chronic conditions, risk of high expenditure). aThe difference between the 2 groups is statistically significant. CCP, Comprehensive Care Practice; ED, emergency department
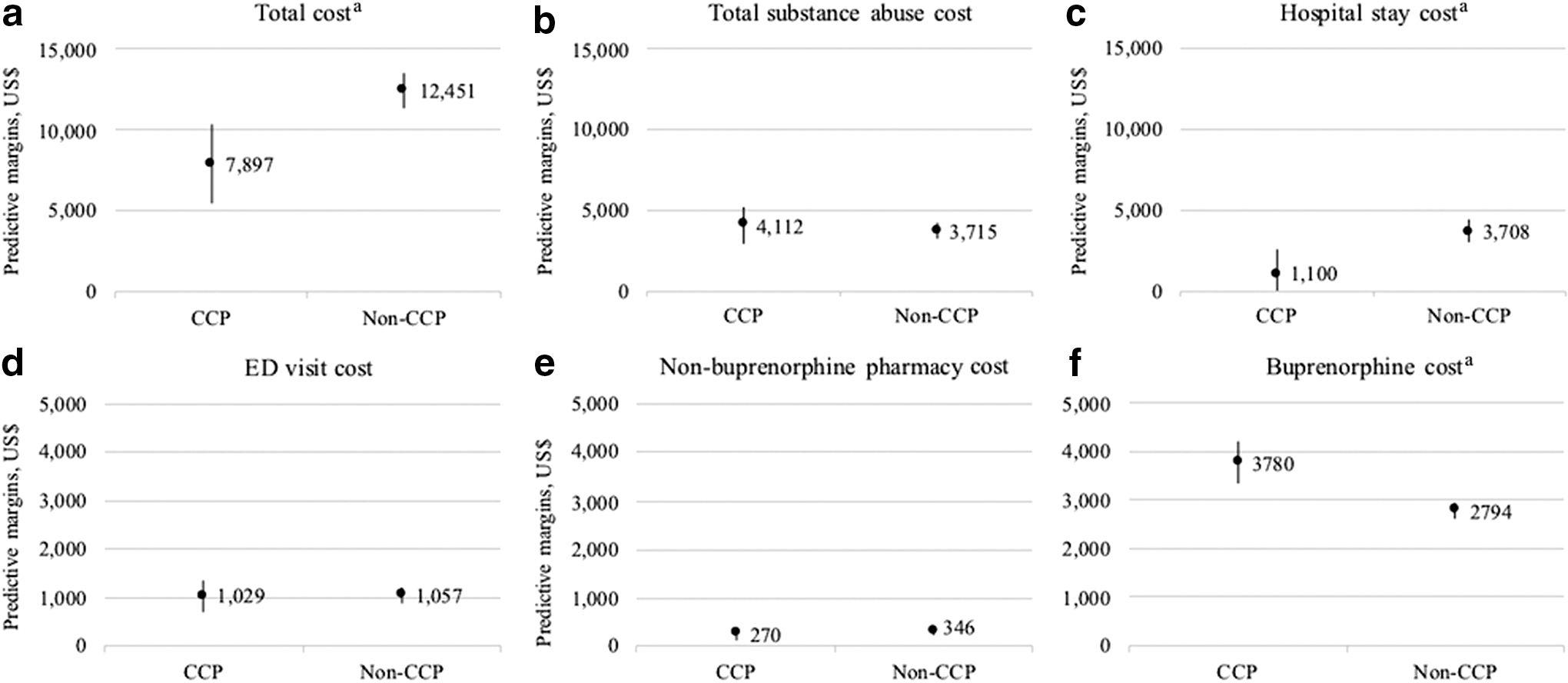
Predictive margins of cost measures by Comprehensive Care Practice and Non-Comprehensive Care Practice groups. Predictive margins with 95% confidence interval adjusted patient demographics (ie, age, sex, race, residing in a county with median household income <US$40,000) and health conditions (ie, count of chronic conditions, risk of high expenditure). aThe difference between the 2 groups is statistically significant. CCP, Comprehensive Care Practice; ED, emergency department.
Follow-Up Outcomes in Comprehensive Care Practice and Non-Comprehensive Care Practice Groups
Regression models adjust for patient demographics (ie, age, sex, race, residing in a county with median household income <US$40,000) and health conditions (ie, count of chronic conditions, risk of high expenditure).
CCP, Comprehensive Care Practice; SD, standard deviation; ED, emergency department.
Mean total annual health care cost was lower in the CCP group than in the non-CCP group; the AME indicates that the CCP group had $4554 lower annual total cost as compared to the non-CCP group (P < 0.001) (Table 2). Hospital stay cost also was lower in the CCP group (P = 0.001). The marginal effects for ED visit cost, substance abuse cost, and non-buprenorphine pharmacy cost were not statistically different between the 2 groups. The CCP group, however, had higher buprenorphine medication cost compared to the non-CCP group (P < 0.001), which is consistent with the results of observed higher retention rate in the CCP group, that is, longer duration of use (Table 2).
Discussion
Using data from a large state Medicaid program, this study evaluated an innovative care model that integrates buprenorphine treatment for OUDs with primary care. Other studies have demonstrated cost saving related to medication treatment for OUD, 8 –14,31,32 but the present study uniquely shows cost savings are greater when treatment is integrated with primary care, as the CCP care model was associated with higher buprenorphine treatment retention rate, fewer acute hospital stays, lower hospital stay costs and lower total health care costs. The patient retention rate of 79% was significantly higher than the non-CCP group rate of 61%, with other studies reporting similar retention rates to the non-CCP group. 33 –36 Retention rate is perhaps the best measure of patients remaining in treatment and working toward recovery while preventing overdose death. In addition, the cost benefits of the CCP care model are especially impactful considering that CCP patients had significantly lower income and more chronic conditions. Moreover, each 15-minute patient visit in the CCP model was spent covering primary care and OUD, making the total time spent with patients in the CCP model likely lower than in non-CCP care. Pharmacy costs for the CCP group were higher, largely as a result of the cost of the longer course of buprenorphine treatment.
The study team only analyzed costs during the first year of buprenorphine treatment, which likely limits the true cost saving impact. Certainly, health care cost savings were related to preventing costs of continued drug use − ED visits related to overdose, withdrawal, and infections from injection drug use. The team hypothesizes that the cost savings increase as patients stay in treatment and engage in primary care for other conditions and needs. Additionally, during the first year of integrated buprenorphine treatment in primary care, the costs related to medical care are likely higher than future years because initially, patients are seen more often and medical problems that are newly identified have higher initial costs to evaluate and treat, at least until the provider can work through the backlog of a patient's unmet needs. Patients engaged in primary care also will have higher pharmacy costs as they are reliably treated for chronic medical conditions, such as hypertension and diabetes mellitus, that they may ignore if not seeing a primary care clinician regularly. Engagement in primary care allows for preventive health measures that are cost saving in the future, but add cost in the present, as patients have screenings (eg, for cancers of the cervix, breast, and colon). 37 The CCP integrated care model also treats hepatitis C, adding present cost, while preventing costs related to the future incidence of cirrhosis and liver failure.
The study is subject to several limitations. First, the data source is claims data from the Priority Partners MCO. Therefore, study findings may not apply directly to other Medicaid or non-Medicaid populations, although there is no reason to suspect that Priority Partners MCO patients are significantly different from those in other Medicaid plans. Also, the study team analyzed data between 2008 to 2013. Additional research is needed to understand practice in recent years. The topic is especially important, when treatment of OUD has been falling behind the increasing diagnoses of OUD and discontinuation of OUD treatment is common. 38 Second, there might have been limited “contamination” in the study groups. Approximately 4% of the non-CCP patients had made at least 1 visit to CCP in the past. However, the contamination would bias the study against finding a positive effect of the integrated model at CCP, and thus the team concludes that the study results are conservative. Third, the team did not have data that measure to what extent the buprenorphine treatment was integrated with primary care outside of the CCP practice in the control group. However, based on the low rate of buprenorphine prescription waivers among primary care physicians, 28 the integration seems limited.
Conclusions
There have been reports on primary care models for the treatment of OUD that are descriptive and demonstrate feasibility and acceptability, 39 but generally, economic analyses have been based on modeling rather than actual cost data. 40 However, present study findings using actual claims data for a Medicaid population show that buprenorphine treatment for OUD can be incorporated successfully into primary care practice, and patients as well as the health care system benefit from this integration model with better treatment retention, fewer hospital stays, and lower health care costs.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The authors received no financial support for this article.