
Abstract
Despite a robust health care system in the United States, many Americans experience health care disparities as a result of poor access to medical care. Academic medicine plays an important role in addressing health care disparities by providing primary and specialty care for the poor and uninsured. In South Carolina, 43 of its 46 counties are designated as fully or partially Medically Underserved Areas (MUAs), defined as areas with a shortage of medical providers, high infant mortality, and either high elderly population or high poverty rates. To address these health care disparities, an academic medical center in South Carolina created a hub-and-spoke specialty care model using telemedicine in partnership with primary care providers across community settings. Initial private foundation grant funding enabled the development and dissemination of technology to provide remote teleconsultations by physicians at the academic medical center (hub) to patients in their primary care offices (spoke). This model, now supported by recurring state funding and professional billing, provides much-needed services, including psychiatry, nutrition counseling, and various surgical and medical subspecialties, to rural and underserved populations in the state. This manuscript provides a narrative review of the development of this statewide telemedicine service, with an emphasis on identification of stakeholders, technology issues, barriers to implementation, and future directions.
Introduction
Patients in rural, medically underserved areas often lack access to high-quality specialty health care services. Nearly 75 million Americans live in designated Health Professional Shortage Areas. 1 In addition to primary care shortages, the majority of rural Americans face severe shortages of specialty medical services, particularly mental health care, with more than 110 million Americans living in areas without an adequate mental health professional workforce. Poor access to care is evidenced by inability to pay, lack of insurance, large distance from tertiary care facilities, advanced age, inadequate knowledge, limited transportation resources, and time constraints, especially for working families. 2
Available research also suggests that medically vulnerable populations are more likely to experience inferior outcomes, more likely to have fewer health care choices, and less likely to see a specialist. 3 Rural counties, in particular, typically have dramatic shortages of nurses, therapists, and nutritionists, as well as half the number of physicians needed, resulting in lower access to needed care for patients. 4
Access to specialty care is particularly difficult for uninsured and underinsured patients. Low Medicaid payment rates typically are the main barrier, although nonmedical challenges, such as administrative burden, lack of transportation, and adhering to treatment plans also are major issues. 5 Lack of specialty care access can result in suboptimal medical outcomes and potential for higher cost resulting in greater utilization of emergency care services and hospitalization. 6
Improving care for these populations falls to primary care providers, community health centers, state Medicaid programs, and academic medical centers (AMCs). A key component to addressing these barriers to care is the utilization of telehealth, bringing specialists to primary care sites through the use of technology. 7 The resources needed to implement a statewide program aimed at meeting these needs typically are found at a tertiary care AMC with a statewide referral base.
Patients in South Carolina face significant multifactorial challenges regarding access to specialty health care providers. Forty-three of South Carolina's 46 counties are designated as fully or partially Medically Underserved Areas (MUAs), defined as areas with a shortage of primary care providers, high infant mortality, and either high elderly population and/or high poverty rates. 8 Extensive areas of South Carolina are classified as rural, with 33.7% of the population residing in a rural area compared to 19.3% nationally. 9 In addition, South Carolina has relatively few tertiary care facilities, and even counties that are in relatively close proximity to tertiary health care exhibit burdensome health care disparities. 10
As outlined by the World Health Organization, South Carolina's social, economic, and political factors related to health systems are exacerbated by the rural nature of many areas of the state and create accessibility problems that are not unique to other populations. 11 Providing access to specialty consultation services in the patient's own community improves health equity. Engaging the primary care physician (PCP) and patient through telemedicine decreases the distance between AMC and the patient, addressing some of the components of social determinants of health, particularly those associated with poverty and health care access.
Intervention history and development
In May 2009, the health care needs of rural South Carolina were assessed and researchers found that a significant gap existed between scarce specialty provider resources and the needs of those patients who require specialty care. 12 The idea for a virtual network to provide specialty services in patients' hometowns came to one member of the research team (SF), a surgeon, as he watched his once computer-averse wife use videoconferencing software from her smartphone to communicate with her new granddaughter. Drawing on the experience of this surgeon's own postoperative patients, the process of accessing postoperative services from outside the study academic health system was weighted with multiple inefficiencies as detailed below.
To evaluate a patient during a 10-minute follow-up visit, that visit required the patient to take a day off from work, find a companion to accompany her or him (who also had to take time off from work), drive up to 4 hours to Charleston, find parking and locate the treatment clinic, and then drive back home – all for a visit that lasted only 10 minutes. Convinced that patients would welcome and soon demand such expanded access to their physicians via telemedicine, the idea for the program was born. 13 The program was designed with the intention to handle such specialty consultations via simple teleconferencing software, sparing patients inconvenience and saving them time and money without sacrificing quality of care.
Dr. Fakhry and his team at the Medical University of South Carolina (MUSC) designed a demonstration program to introduce an innovative approach using relatively simple, cost-effective telemedicine technology to link patients and their local community physician resources with specialists at the AMC. The long-term goal of this work was to bring simplified, sustainable access to specialty health care to patients in underserved rural areas. The project, known as the Virtual TeleConsultation Clinic (VTC), also sought to obtain perspectives from patients and clinicians on the feasibility of using telemedicine technology to link patients and their local community physician resources with specialists at MUSC as a long-term solution for the underserved areas of the state.
Gathering expertise from several areas at the academic institution, a project team was formed with expertise in telehealth, rural health, technology, and survey research methodology. This interdisciplinary demonstration project combined the resources and expertise of a tertiary AMC (MUSC) and its large network of specialists, the insight from an established statewide regional education consortium, the South Carolina Area Healthcare Education Center, with long-standing experience and involvement in rural regions, and with community-based PCPs. The AMC's information technology (IT) group was included in the collaboration to provide expertise and access to software, hardware, and networking infrastructure.
In 2011, The Duke Endowment awarded Dr. Fakhry 2 years of demonstration funding for a project to address the need for specialty consultative services. As part of the project, the plan was to develop a low-cost technology solution to connect rural primary care practices to specialists at MUSC. A simple software technology was selected, called Jabber (Cisco Systems, San Jose, CA), which was similar to other popular consumer video communication applications with the added benefits of security and privacy required to ensure Health Insurance Portability and Accountability Act compliance. At the time of the application review and selection processes, it was one of the few cost-effective solutions that worked across a variety of hardware and software devices. Jabber would be installed on a desktop computer and provided to the primary care facility along with a high-definition camera. The software would connect with MUSC specialists over a standard internet connection.
Methods
Pilot project implementation
Implementation of the pilot VTC program occurred in 2 stages over the course of the demonstration project (Table 1). The project team was formulated with leaders at MUSC in the areas of clinical medicine, IT, population health, and administration. Initial identification of the target population included medically underserved counties within a 2–3 hour driving distance of the MUSC campus. This 5-county region included the counties of Allendale, Bamberg, Georgetown, Florence, and Barnwell. More than 90% of the area of these counties is designated as (MUAs). 8 The demographic composition of this region is 43% African American, 55% white, and 2% other. As part of the initial project phase, 2 needs assessments were conducted. This process confirmed that patients in rural areas of South Carolina were likely to seek specialty care outside their region, frequently traveling significant distances at substantial cost.
Stages of Virtual Teleconsultation Clinic Development
This table outlines the stages of VTC program and service development.
MUSC, Medical University of South Carolina; VTC, Virtual TeleConsultation Clinic.
An IT needs assessment was administered with each future participant primary provider to determine their current IT equipment and educational needs. An interim technology assessment was planned for 1 month after project implementation to ensure that any earlier unmet needs had been met. Otherwise, further steps were taken to meet them and prevent clinical disruption.
Patient educational materials were developed with a detailed explanation of the consultation steps. The project initially started with existing PCP sites covering 5 MUA counties (Figure 1). These sites were recruited by a former multicenter National Institutes of Health-sponsored trial of CREST (Critical Care Excellence in Sepsis and Trauma) patients. Training of sites and PCPs was done in person through Cisco Jabber software installed on laptops and through mock interviews conducted using the VTC equipment.
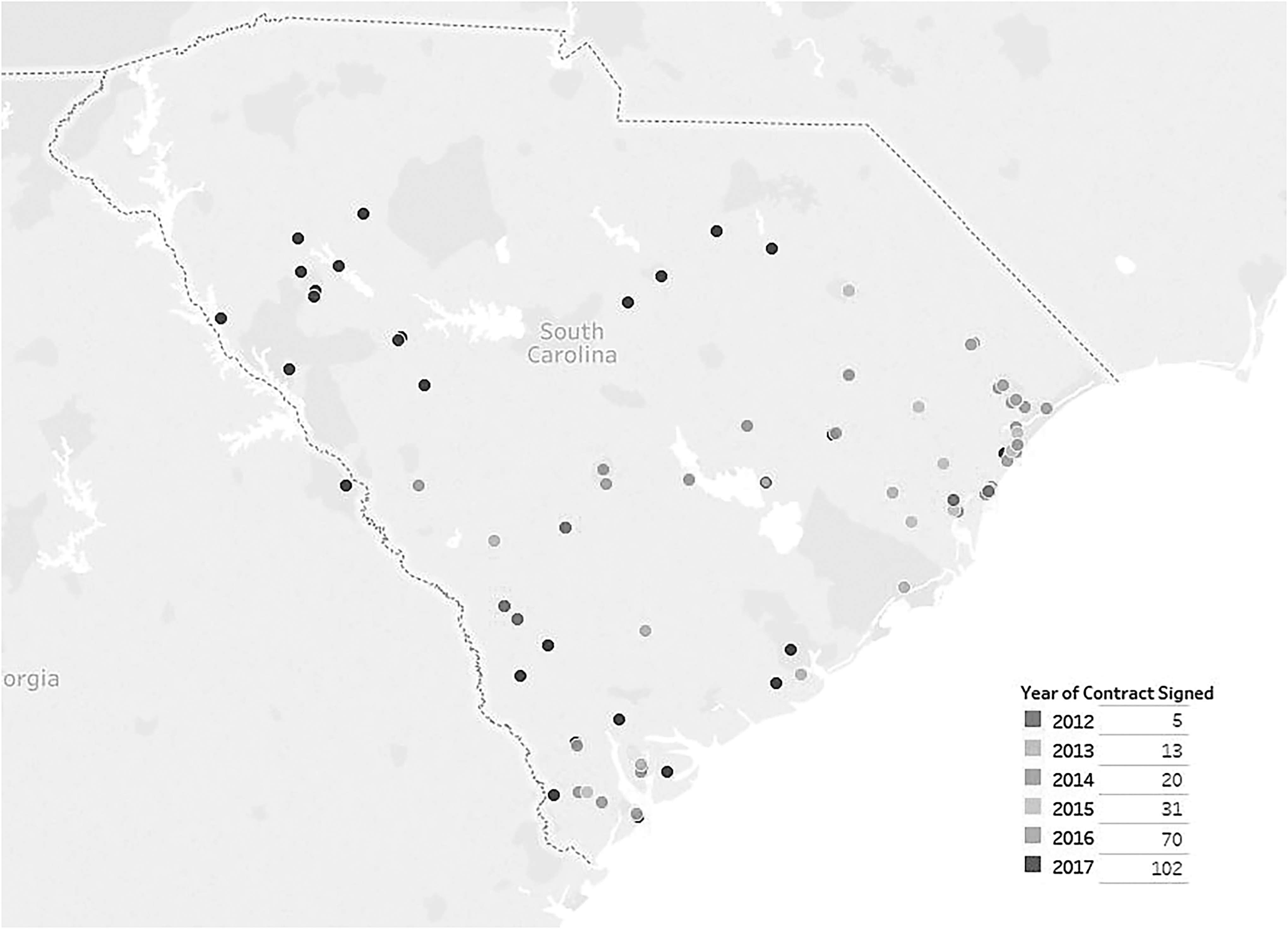
Map of service locations 2012–2017. This figure reflects the development of clinical sites across the state from 2012–2017.
Coordination of scheduling consultations, including PCP site, MUSC physician, and patient, was done on paper. The program coordinator was present for the initial consultations to ensure that connectivity was smooth. Patients were seen as part of the normal daily operations of the PCP site through the use of their medical staff to schedule and check in patients, launch the video consults, and serve as telepresenters, if needed. Movable technology and on-site PCP providers were integrated as appropriate throughout the consultations. All technology issues were addressed over the phone by a dedicated IT team at the AMC. From the AMC physician point of view, 2 models were employed, depending on subspecialty.
For high-volume services, such as psychiatry or nutrition, scheduled clinic blocks were formed and managed. For lower volume medical or surgical subspecialties, consultations were scheduled during regular clinic hours and the physician would use telemedicine carts stationed in their clinics in an ad hoc manner. Dedicated IT staff were employed to maintain connectivity. As these services grew, dedicated telemedicine consultation rooms were built to house AMC physicians.
Stage 2 was implemented during the second year. The focus was on slow growth in PCP practices and recruitment of specialty providers in order to prove that the program was scalable. Recruitment of PCP sites to participate was done in person by the program coordinator and physician liaisons. Recruitment of subspecialty providers at MUSC was done by word of mouth and through previous clinical relationships. A key component of Stage 2 was measurement of satisfaction data on the part of patients, PCPs, and specialists. The surveys were completed on hand-delivered paper surveys, were faxed to MUSC, and compiled in a Redcap database. Lastly, the research team began tracking patient-level data, including county of residence, in order to calculate patient time and cost metrics.
Results
Intervention evaluation
As part of the demonstration project, the VTC team sought to measure stakeholder satisfaction as a primary end point. These data were utilized to facilitate program development and track progress toward program goals. First, anonymous surveys of specialists, referring providers, and patients were conducted pre- and post-consult to determine program satisfaction. These surveys were developed by a biostatistician on the project team using on a 5-point Likert scale. Survey items included an assessment of perceived provider access to the specialist consult via the VTC, the timeliness of access to the specialist consult, appropriateness of patient selection for specialist consult, and patient/provider adherence with follow-up.
Patient surveys collected information related to potential barriers to care, perceived benefits of telehealth, and satisfaction and comfort with the telehealth experience. Specifically, 97% of patients surveyed agreed or strongly agreed that they felt comfortable with the health care visit being conducted through the teleconsult system, and 99% perceived that the teleconsult was easier than driving to Charleston to see the provider in person. Overall, 97% of patients were satisfied with the teleconsult, and 96% would be willing to take part in another teleconsult visit.
Provider surveys assessed the provider's satisfaction and experience with the telehealth encounter. One hundred percent of providers felt they could understand the patient's problem to make an appropriate recommendation and agreed it was easy to communicate with the patient through the teleconsult system. In addition, 100% responded that the virtual consult clinic met their expectations and agreed that the virtual format could increase the number of referrals to their specialty. Overall, 89% of providers agreed that they would be willing to participate in additional virtual consults.
Interviews with PCPs and AMC physician providers were conducted at 3 time points. First, 2 focus group interviews, including PCP physicians, MUSC providers, and patients who had completed a consultation, were held to identify expectations and potential barriers to VTC. Midway through the program, an interim assessment was conducted to determine potential obstacles and solutions. Finally, program administration tracked numerous program process outcomes including: the number and type of consultations, and the number and location of primary care practice locations. In addition, the research team tracked the potential patient miles saved by calculating the distance between the primary care office and the specialist location. This information is used to calculate patient cost savings metrics, such as drive time saved, gallons of gas saved, and auto maintenance avoided.
Access to specialty care services
As the network of PCP providers grew throughout the state, a gradual process of adding specialty services was underway at the AMC. The PCP offices included both pediatric and adult services, in a variety of settings, including family medicine, internal medicine, general pediatric practices, and federally funded health clinics. An informal survey of the PCPs was performed as the VTC enrollment of their offices evolved. Nutrition and adult surgery services were the initial enrollees with providers from the AMC. Program personnel then systematically met with physician champions from departments in the AMC to determine which services were suitable for teleconsultation. Another early adopter was psychiatry. Under the leadership of both telemedicine champions and the department of psychiatry, a significant effort was put forth to increase psychiatric consultations to rural areas. Today, this is the highest volume service of the VTC.
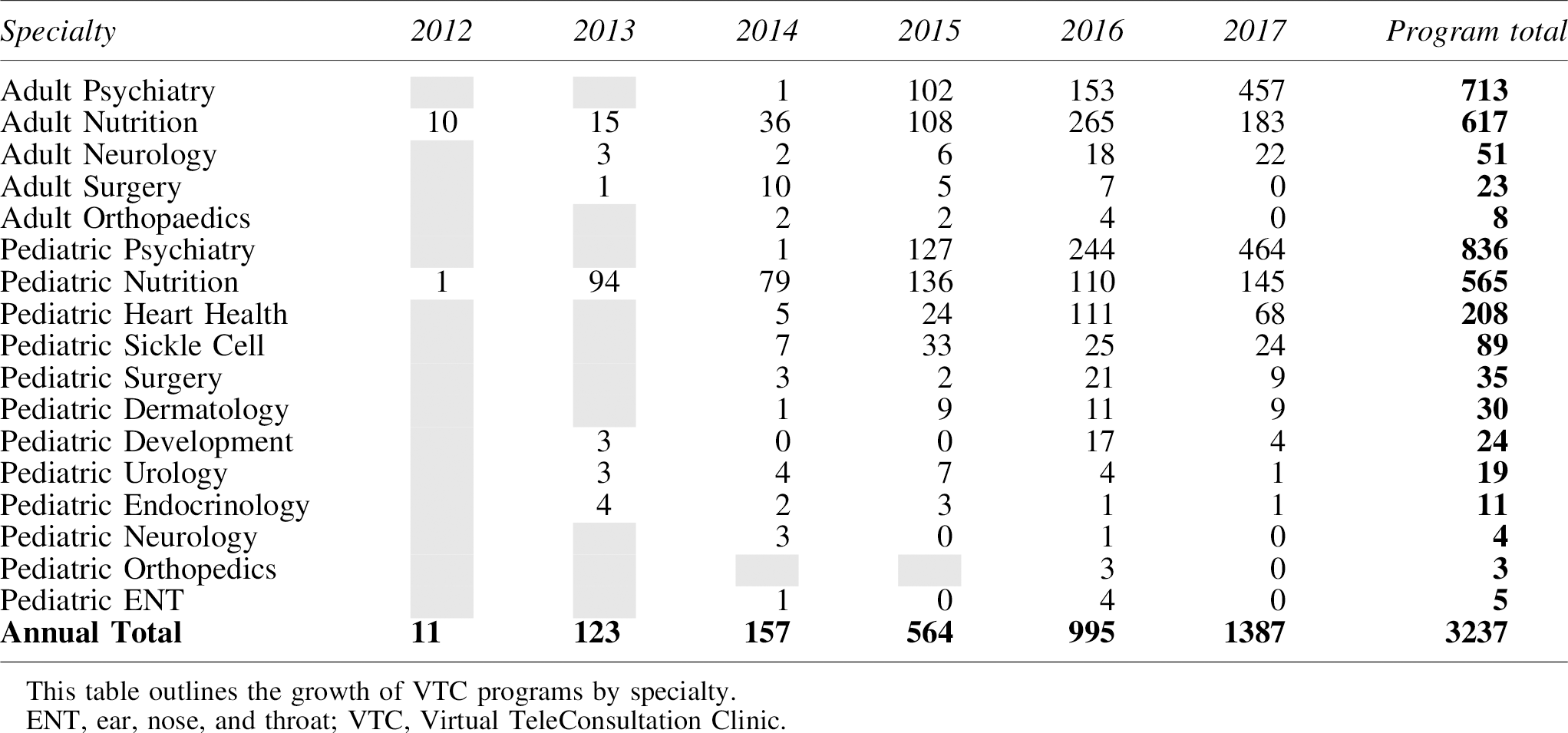
Gradual growth of various surgical and medical subspecialties has been achieved. The VTC currently provides teleconsultations in 23 different specialties. Although some services provide fewer than 10 consultations a year, others, such as psychiatry and nutrition, continue to grow in volume and outreach (Table 2).
Virtual Teleconsultation Clinic Service Expansion
Program growth
In 2012, the program conducted 11 patient consultations in the fields of pediatric and adult nutrition and adult surgery. The most frequent consultations to date are in the adult and pediatric psychiatry services (Figure 2). Over time, continued growth has been demonstrated in both the number of consults performed and the number of practices contracted (Figure 3). Between 2014–2015, during rapid addition of PCP practices and specialist resources, 193% growth was observed. A critical mass of programs, both subspecialty consultation services as well as PCP referral practices, has led to steady gains in virtual teleconsultations.
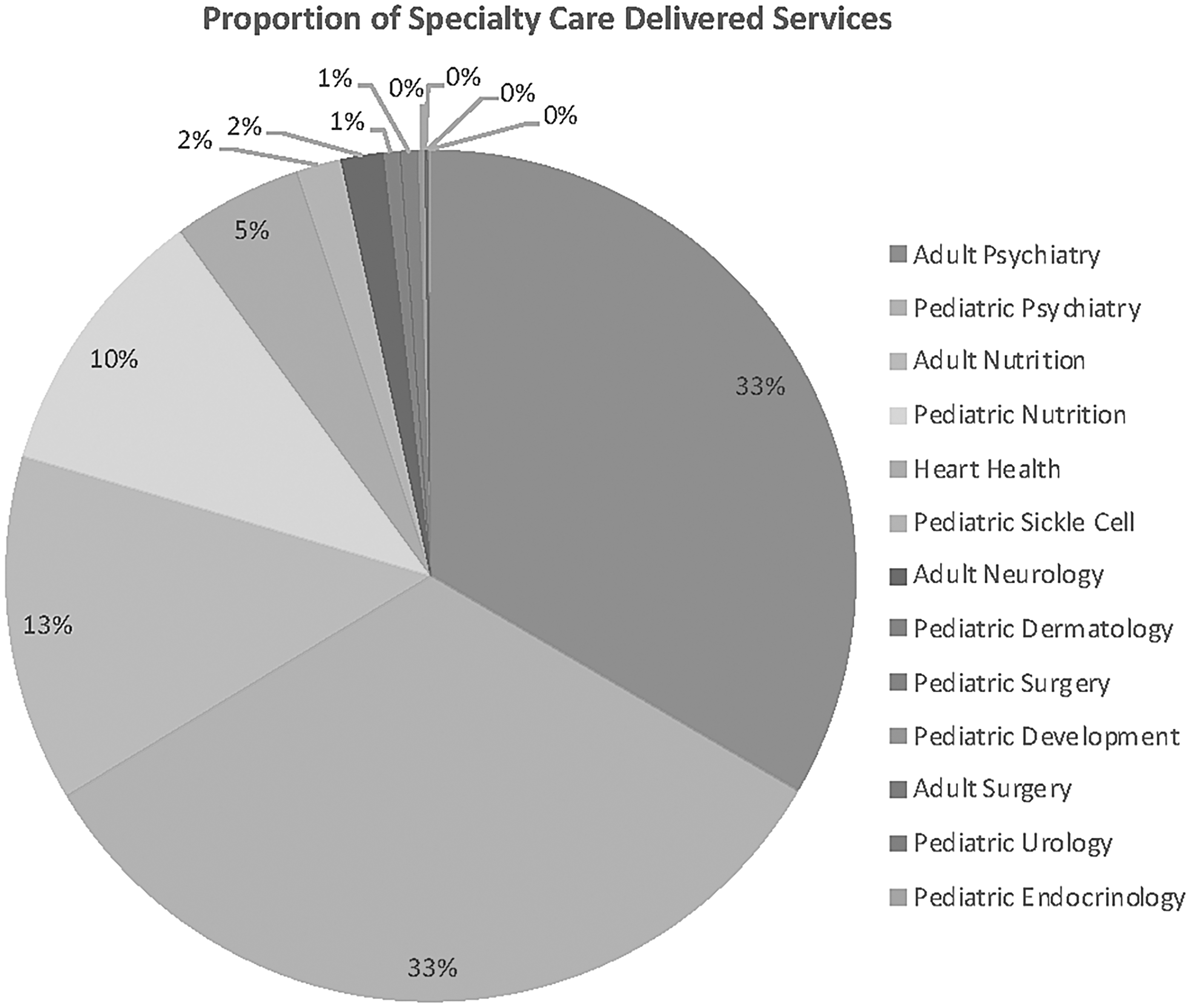
Proportion of specialty care delivered services. This figure presents the percentage of specialty services delivered through the Virtual TeleConsultation Clinic program.
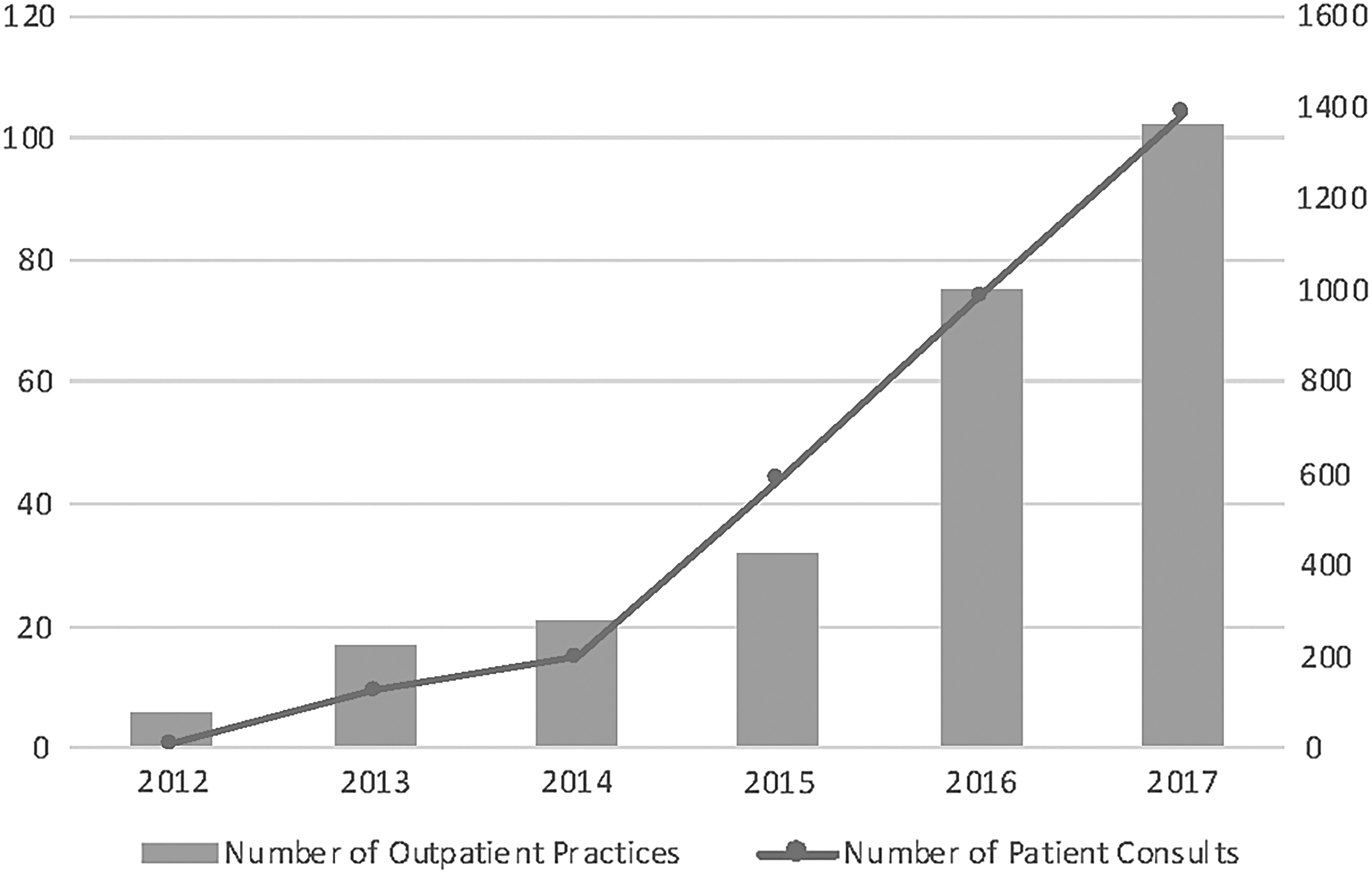
Annual number of outpatient consultations and participating outpatient practices. This figure shows the growth in clinical consultations and practices for a 5-year period.
In 2017, the VTC program provided more than 1300 consultations across 102 practices throughout the state, demonstrating a year-to-year growth of 39%. The program reaches PCP practices in 19 counties across South Carolina. Also of note is the type of patient visit. Since November 2014, the majority of VTC consultations were for ongoing visits (54.1%), with less than half of consultations completed (45.9%) for new patients.
Program growth also was facilitated by the ability of PCP offices to bill for each encounter through a facility fee. The facility fee pays for exam room maintenance and ambulatory nursing care. Telepresenters, such as physicians, nurses, or clinical nurse assistants in the PCP office, are used for more complex encounters, typically encounters that require a physical exam. These exams were led by the consulting physicians, often through coaching during the teleconsultation. More complex exams were required by surgical and medical subspecialists. For high-volume services, specifically psychiatry and nutrition, there is no need for telepresentation because the majority of consults are facilitated through simple video communication without the need for additional diagnostic peripherals (ie, cameras, scopes).
VTC patient savings
By eliminating the need for patients to travel to the AMC, it is estimated that the VTC program resulted in saving more than 642,000 travel miles for patients and their caregivers. This is based on 13,000 hours of driving time and $71,000 in fuel costs (Figure 4). These savings also were perceived by patients; survey results showed that 90% of patients agreed the telehealth program “made it easier than having to drive to Charleston to see the specialist.”

Travel and cost avoidance for rural patients treated by VTC since the beginning of the program. This figure represents the various cost savings generated for patients and their families. Calculations based on a total of 4087 completed appointments conducted from September 2012 through May 2018. The average round trip mileage saved per patient visit was 157 miles, with a range of 0–1838 miles. The time savings for travel are calculated at a speed of 50 miles per hour. Fuel costs are based on $2.50 per gallon with a 22.5 mile per gallon average fuel consumption. Auto costs are based on a maintenance rate of $0.565 per mile. VTC, Virtual TeleConsultation Clinic.
Technology costs
Initial grant funding was used to cover the costs of starting the VTC over a 2-year period. Direct technology costs for year 1 totaled approximately $75,000, including the provision of cameras and microphones to PCPs, broadband connections for local primary care offices, and computers and software. Initial teleconsultations were performed on laptops provided through in-kind contributions.
As the program grew and funding moved to a statewide effort, it became necessary to improve the quality and functionality of the telehealth consults. The VTC provides a cart integrated with equipment, delivered to and set up at site at a cost of $4500, covered by MUSC initially and later through state funding administered by the South Carolina Telehealth Alliance. These funds cover the cart components, assembly, testing, and delivery. The cart consists of a mobile cart, teleconference kit, computer processor, 24” monitor, and video camera. These are separate components that are assembled by a third party, who also delivers and tests the equipment. There are no costs to the PCP offices.
Discussion
Lessons learned
The “hub and spoke” model has been a rather ideal schematic for the VTC network with the hub residing at the AMC and the spokes at primary care offices. Although specialty care was available in South Carolina, not everyone had ready access to such services. 14 The conceptual framework captures a spectrum of specialized care offered at the AMC and brings those specialties to the various PCPs, providing enhanced access with substantial opportunities for streamlined cost-effective care, particularly for rural patients. Similar solutions can be applied using other local or regional health care systems that can leverage workforce and technology resources to scale. As telehealth delivery costs decrease, patients may gain more access to remote specialist services without the need for the resources of an AMC.
Several key lessons have been learned in developing this statewide referral network. First, the most measurable benefit is directly to patients who are receiving these medical services. The use of an approach that could expand access while reducing patient travel burden was an effective and welcome approach. For example, one specialty the VTC program offers is adult and pediatric nutritional services. Rural residents of South Carolina have high rates of obesity, hypertension, and diabetes but have poor access to dietitians trained to help them manage these diseases. Dietitians participating with the VTC are able to provide nutritional counseling to patients at physicians' offices in rural areas of the state.
The first teleconsult was for Adult Nutrition and was conducted in September 2012 with a patient whose medical home was in the rural community of Bamberg, SC. The practice's managing physician stated, “We are in a very rural town. Our hospital closed the end of April 2012. Telehealth seemed like the up-and-coming thing and I felt like it would be a great advantage to my patients.” These one-on-one nutrition and behavior counseling consultations helped these children, adolescents, and adults learn ways to manage their weight, reduce obesity, and improve overall fitness.
The second lesson learned is that community PCP offices are willing partners with the AMC in order to help their patients. As evidenced by the year-to-year growth demonstrated in the number of PCP offices and patient encounters, community practices were excited about offering telehealth with MUSC. Christina Vaughan, MD, a MUSC neurology specialist, conducted a telehealth consult with a patient at South Strand Internists & Urgent Care in Pawleys Island, SC. Following, the PCP, Tom Howard, MD stated,
“I am impressed with the live video consulting! This is going to be revolutionary for patient care going forward!!! I don't think that I can accurately quantify the improvement in both continuity of care and level of service this will add to the patients experience and care! The possibilities are endless!!! I'm stoked!!!”
Early on, the value of the program was evident despite the PCP having to commit some resources. PCP offices have demonstrated a willingness to participate despite some perceived barriers, including the use of an exam room and the potential need for a telepresenter. To meet the needs of more complex cases, such as with several pediatric sickle cell patients, several clinics made special arrangements and committed human resources to help with the advanced care coordination required to provide improved care for these patients. Simply by using a collaborative care model connecting the patient, the specialist at the AMC, and the PCP, patients are able to receive services that are not available locally, to have additional follow-up more frequently with the specialist, and to benefit from the social service resources that are available locally. Additionally, there are opportunities within VTC visits to include other clinical activities that support well-child visits, assist with medication refills, and ensure ongoing communication with the PCP team.
The third lesson learned is that there is significant reluctance on the part of the AMC consulting provider to disrupt their workflow to participate in telemedicine efforts. In the era of fee-for-service physician reimbursement, every minute of the physician's time can be viewed as billable time. The initial consultations performed in the VTC pilot phase were performed pro bono, without reimbursement for the physician's time. As volume increased, PCP offices demonstrated need for specific services, specifically psychiatry and nutrition.
In order to meet demand, agreements to support AMC physician time for the high number of referral services were made. In the research team's experience, the need for this dedicated full-time employee (FTE) time may be a common, or even essential, element for a telehealth consultative program to grow to scale until professional billing revenues and clinical efficiencies are established through streamlined workflows. Although efficiencies are seen in improved care coordination for the patient, reduced travel time, and closer consultative support to PCP partners, AMC provider satisfaction and workflow are important considerations.
In initial provider surveys during program development, it was found that providers were very satisfied with the communication quality during teleconsultations and were likely to perform more consults in the future. However, as volume increased, providers reported additional time requirements for pre-consult preparation, conducting the telehealth consults, and documentation and post-consultation coordination. These same provider sentiments have been borne out in the literature, 15 although robust provider satisfaction data is poorly reported.
In dealing with these issues, it was found that financial support for physician time for telemedicine has been a key driver of physician participation. As hospital systems deploy telemedicine consultation services that rely on physician or other advanced practice providers, serious consideration must be given to support professional time. Program management continues to assess consultation volume and is able to add FTE capacity as consultation volumes increase.
The fourth lesson learned is that implementation of the VTC practice requires an efficiently functioning, multiskilled team. 16 The project team must be cognitively diverse and have the requisite skill sets for the establishment of the telehealth infrastructure as well as the skills necessary for the management of both physician and patient needs. The team must address and implement hardware and software issues, training of providers and presenters, installation of the infrastructure, and the fiduciary issues that are common to all of medicine.
The fifth lesson is that the actual technology platform and its price tag may have less to do with the success of the program than the other variables described. In fact, given the continued improvement and dissemination of cost-effective telecommunication technology, there may be a point in the not-too-distant future when the technology that patients use for their personal communication needs may be the preferred tool for accessing specialty care at remote locations. This concept should inform purchasing and budget decisions for similar programs and help keep the technology costs of the program low. Commercial vendors of telehealth have already seized on this concept and established successful care delivery models using technology that patients already possess (eg,
As the direct-to-consumer capabilities of the study institution's services grow, the VTC program is committed to supporting patients in the communities where they live and work while continuing to engage local PCPs for improved population health outcomes. Unfortunately, health care reimbursement models in telemedicine still require an originating site that does not include the patient's home in most states. As originating site restrictions are lifted, new models of teleconsultation will be created. The current practice that has been outlined is an evolving model based on continuous feedback from all partners.
Barriers to implementation
Barriers to patient telemedicine adoption have been well documented in the literature and include the fear of losing a relevant therapeutic relationship with their physician, unwillingness to participate in a virtual visit, and inherent distrust of the technology and sequela of virtual health care information security. 17 It remains incumbent upon the developers of telemedicine programs to methodically facilitate the secure, accurate, and reliable sharing of health information and therapeutic service options between providers and patient populations that will continue to expand.
Perhaps the greatest impediment to the successful implementation of a VTC platform lies in the minds of those who will provide the service. Physician acceptance and adoption of the VTC model is fundamental for any measure of success or sustainability. 18 The internal barriers were a reticence on the part of tertiary specialists to adopt telemedicine related to the novel practice changes inherent in teleconsultation, the uncertain reimbursement structure for consultation services, and the perception that this innovation requires a significant time commitment for implementation. 19 The introduction of a telemedicine model into a rural setting represents an authentically disruptive innovation with the perceptions of unwanted competition, malevolent observation, and omniscient censure proving all too formidable as barriers to local adoption. The continuous education of specialists has and will continue to ameliorate these concerns.
This paper demonstrates that a video-based telehealth consultative service between an academic health system and independent primary care sites is feasible and demand is increasing. A point of further exploration is that the overwhelming majority of consultation requests were for nutrition and psychiatric services, as the cognitive evaluation may be more feasible. The reasons for this may be multifactorial but certainly are anchored in the needs and realities of the primary care clinics. One hypothesis is that nutrition and psychiatric services are core to the primary care mission and part of the everyday care provided in this setting.
Although collaborative care with specialists also is certainly a key element in primary care, it typically is outside the scope and resource allocation of an individual PCP office. It should be noted here that although facility fees were billable for the primary care sites, in South Carolina they typically have been relatively low compared to other states (approximately $15 versus $25 based on Medicaid fee schedules). This reality also provides insight into how to direct the program in the future. A focus on the value case of supporting a PCP's traditional mission versus one of extending specialty services is worth considering. Such a shift in focus alters the staffing and sustainability implications for the service.
Exploring bundled payment models or collaborative care payment approaches may provide opportunities for future telehealth reimbursement and sustainability. True collaborative care payment structures, specifically the Behavioral Health Integration model, will pay for care coordinator personnel, which will allow more seamless communication between the multidisciplinary team and patient. 20
Conversely, the need for specialty extension to underserved areas persists. The establishment of regionally-placed, telehealth-based outpatient clinics with added staffing to facilitate complex evaluations may be synergistic, rather than competitive, to the medical home connections based on the research team's experience. Another exciting development in telehealth is the use of e-consults, or asynchronous messaging between referring and consulting providers. It is exciting to see the potential of combining multiple telehealth models to meet the needs of underserved populations.
Future Directions
The potential for telemedicine as a disruptive technology is staggering, especially in the realm of provider and specialist scarcity. The VTC platform has the potential to extend consultative practice model capabilities in an unprecedented fashion while increasing access to previously underserved populations. Payment models are evolving to incentivize this modality for the delivery of clinical care. The education of future clinicians should include a curriculum encompassing the essential competencies in telemedicine care. 21 Additionally, a patient education campaign funded and initiated by various professional associations would offer the information necessary to move public adoption in a manner that will lead to more widespread acceptance and adoption.
The VTC framework is a viable construct for increasing patient access while providing downstream cost savings and demonstrating reasoned equivalence to the inpatient visit. The cost savings to the patient is well documented in this report as well as others. Cost savings to the parent institution are less clear. Cost analysis research that factors in initial infrastructure, personnel costs, and technology investments while accounting for provider payment models is essential to supporting increased telehealth services in community settings. Additional research is needed to better understand the implications of increased specialty care access through telehealth on health outcomes, ways to expand efficiencies within the clinical practice domain, and how the relationships of primary and specialty care practices can be strengthened to improve population health metrics. In conclusion, sustainable partnership models should be explored as the shift continues from fee-for-service reimbursements to better management of populations through managed care agreements.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The authors received no financial support for this article. The project was supported by a grant from The Duke Endowment (S. Fakhry PI), Award Number 6310-SP, awarded June 9, 2011.