
Abstract
The objective was to evaluate the long-term impact that the University of Rochester Employee Wellness program has made in reducing cardiovascular disease risk. The authors conducted a 5-year retrospective study to measure change in health outcomes for more than 16,000 employees who participated in the program for more than 1 year between January 2013 and December 2017. A logistic regression model was applied to estimate the impact of participation on improvement in cardiovascular disease risk. Statistically significant improvement was found in the health of participants. Almost 50% of all program participants, having moderate-to-high risk at baseline, improved their 10-year cardiovascular disease risk. Moreover, about a third of participants improved by a full risk category. Engagement in a condition management program also was found to increase the odds of improvement by 36%. The integrated approach to wellness can improve the long-term health of participants and reduce their risk of developing cardiovascular disease by achieving long-term improved lifestyle behaviors. Employers, employee benefits brokers, and insurance companies need to assess wellness programs by their performance and by their design, specifically as it relates to long-term outcomes.
Introduction
Cardiovascular disease (CVD) remains the leading cause of death in the United States, accounting for more than one third of all deaths in recent years. 1 Although there has been progress with a reduction, overall, in the prevalence of CVD, and its associated mortality, 2 current data suggest that the increased incidence of certain risk factors in recent years may account for a reversal in this trend. 1 Risk factors for CVD include high blood pressure, high cholesterol, uncontrolled diabetes, obesity, and smoking. 3,4 About 47% of the US population has at least 1 of the key risk factors for CVD. In addition to being tied to CVD, these 5 risk factors also are associated with other chronic conditions, such as cancer, chronic respiratory diseases, and diabetes, together accounting for almost 2 out of every 3 deaths globally. 5
It has been reported that the cumulative productivity losses associated with chronic conditions in 2003 totaled $1.1 trillion, although only $277 billion was spent on direct health care. 6 The total impact of these diseases on the economy was $1.3 trillion annually, and this has grown with the increased prevalence of chronic illness in the US population, with a predicted 42% increase in prevalence from 2003 to 2023. Preventable chronic conditions are responsible for three fourths of all health care spending. 7,8 The increased prevalence of chronic conditions and associated rise in health care costs have become even more significant to employers as they move toward cost sharing with health plans or self-insurance. 9
Keeping people healthy, preventing chronic conditions, and managing existing conditions is perhaps our nation's greatest gap in care. Chronic conditions in general and CVD in particular present significant challenges to individuals, families, providers, and employers. Effective self-management or prevention of chronic diseases improves function and quality of life for those potentially living with the condition, addresses the high cost and utilization often associated with chronic disease, and enhances satisfaction of individuals and their families. 10
Implementation of workplace wellness programs was included in the Department of Health and Human Services Healthy Workforce 2010 plan. 11 Employee workplace wellness programs can reduce health risks, improve quality of life, increase productivity, reduce absenteeism, and reduce the demand for medical services. 12 –14 In addition, workplace wellness programs can achieve a reduction in health care spending by reducing participants' 10-year predicted risk for developing CVD. 15 These programs require some financial investment for the employer but have the potential to mitigate rising health care costs and provide a positive return on investment. 16
Although many employee wellness programs are available to employers, there is limited information on their effectiveness and long-term outcomes. The purpose of this study was to evaluate the long-term impact that an employee wellness program has made on improving health by reducing risk of developing CVD.
Methods
Wellness program
The University of Rochester (UR) School of Nursing established a wellness program known as UR Medicine Employee Wellness Program (UR Wellness). The program was first offered to UR employees in 2012, and their outcomes were studied here. The program provides technical, operational, and clinical services that assure an integrated solution for organizations to enhance the health and well-being of their employees. The wellness platform was designed to improve access to services and results, provide pertinent information to the wellness provider and participant, enable several wellness initiatives to be offered under a single umbrella, and target intensive coaching resources to individuals at risk.
The UR Wellness program is organized around 3 key components: the Personal Health Assessment, Wellness Engagement Plan, and Wellness Coaching Programs. Figure 1 illustrates the flow between the 3 key components of the program. The Personal Health Assessment is focused on assessment of the participant's current state of health and risk factors. The Wellness Engagement Plan is focused on the transmission of knowledge to participants about their current health risks and steps that they can take to make meaningful changes to improve their health, including referral to Wellness Coaching Programs. The Wellness Coaching Programs include both individualized and group coaching programs, designed to address each client's specific health risks.

UR Wellness Program process. CVD, cardiovascular disease; PHA, Personal Health Assessment; UR, University of Rochester; WCP, Wellness Coaching Program; WEP, Wellness Engagement Plan.
The Personal Health Assessment consists of 2 parts, the first of which is completion of a web-based questionnaire assessing lifestyle and behavioral risks and motivation to change. The second part is a point-of-care biometric screening performed by a registered nurse, who collects data on total cholesterol, high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), triglycerides, blood pressure, blood glucose, height and weight, and abdominal girth. Blood samples were collected by a fingerstick and analyzed by PTS Diagnostics CardioChek Plus Analyzer (PTS Diagnositics, Whitestown, IN). Blood samples could be fasting or non-fasting, with different recommended ranges for each. Blood pressure, weight, and abdominal girth were all measured by the nurse at the biometric screening while height was self-reported.
The first opportunity to employ the Wellness Engagement Plan and Wellness Coaching Programs occurs at the time of biometric screening, during the face-to-face encounter with a registered nurse, dedicated to wellness. The nurse utilizes a web-based clinical dashboard (a summary of the participant's wellness profile, including immediate and past trended biometric screening results, lifestyle score, and 10-year CVD risk score) to inform and coach the participant in ways he/she can improve long-term health. The nurse further directs participants to Wellness Coaching Programs and other appropriate resources.
The second component of the Wellness Engagement Plan is a secure web-based wellness portal that is personalized for each participant. A wellness dashboard includes the individual's 10-year CVD risk score, lifestyle score, trended biometric values over time, customized recommendations for lifestyle improvements based on her/his reported behaviors, targeted referrals to Wellness Coaching Programs to improve health, and access to a health coach.
Wellness Coaching Programs include individual and group wellness coaching programs that are targeted to participants either living with chronic condition(s) or at risk of developing chronic conditions. Individual coaching programs are targeted to participants with a chronic condition and are provided in a one-to-one format. They are offered in person, telephonically or via telemedicine for maximum flexibility. The typical number of sessions ranges from 5 to 7. Individuals are assigned a wellness coach (typically a registered nurse) and have access to a multidisciplinary team including nutrition and fitness experts.
Group coaching programs vary in length and are offered for weight loss, fitness, nutrition, and other lifestyle behaviors. Both variations of Wellness Coaching Programs (individual and group setting) are evidence-based, utilizing current national guidelines (
Study design
The research team used a single-group pre-post quasi-experimental study design and analyzed individuals' self-reported data as well as biometric data, obtained by the wellness program nurses over a period of 5 years.
Program participants and data sources
The sample for this analysis was drawn from individuals who participated in the UR Wellness program. Inclusion criteria were all employees and spouses covered by a UR health plan who participated in the program for more than 1 year between January 2013 and December 2017. Participation was defined as completion of the Personal Health Assessment survey, biometric measures, and nurse coaching session. Eligible individuals were further referred to condition management and/or lifestyle management programs. Participation in the UR Wellness program was voluntary and small financial incentives were provided by the employer to reward completion of the Personal Health Assessment, and up to 2 Wellness Coaching Programs.
Figure 2 illustrates the final sample calculations and study participants. A total of 16,284 unique individuals participated in the UR Wellness program between January 2013-December 2017 at least 1 time. A subset of 9646 participated for more than 1 year; of these, 9116 participants had complete information. This is the sample used to describe the baseline demographics of participants. For this analysis, the first year of participation was considered to be the baseline and the most recent year of program participation as post program.
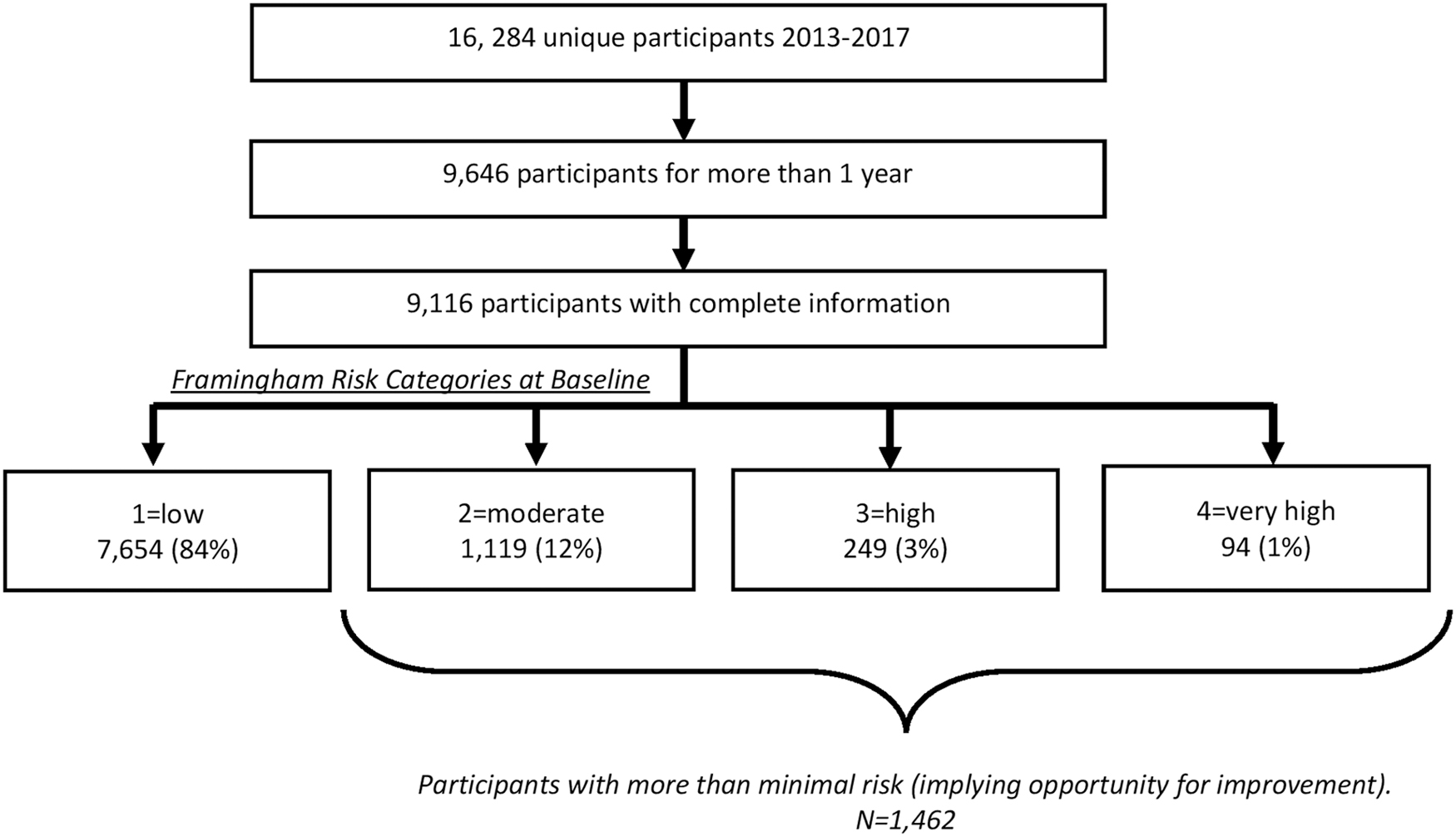
Program participants.
Demographic information was extracted from the Personal Health Assessment questionnaire. Additional information from the Personal Health Assessment questionnaire included self-reported disease state (eg, diabetes diagnosis, hypertension treatment), CVD history, and behavioral risk factors such as smoking. All biometric measures were taken by a registered nurse during the biometric screening process and included the following measures: total cholesterol, HDL, LDL, triglycerides, blood pressure, blood glucose, height and weight, and abdominal girth. This study was approved by the UR Office of Subject Protection.
Outcome variable
The Framingham CVD risk score was used to estimate each participant's 10-year risk of developing a CVD. 17,18 The score is based on the modifiable risk measures of smoking, total cholesterol, HDL cholesterol, and systolic blood pressure, as well as non-modifiable risk measures (age, sex, and hypertension medication treatment). These 10-year risk scores are coupled with additional factors (diabetes diagnosis, diastolic blood pressure, and CVD history) and mapped to 4 risk categories: 1 = minimal risk, 2 = moderate risk, 3 = high risk, 4 = very high risk.
Analysis
Descriptive statistics were used to describe the individuals' characteristics and risk factors. All health risk measures were classified into 2 categories of modifiable measures and non-modifiable measures. Modifiable risk measures were dichotomized into high risk or not. Individuals were considered to have high-risk measures if they were smokers, had total cholesterol ≥200, HDL <40, systolic blood pressure ≥140, and/or diastolic blood pressure ≥90. Two-tailed t tests and χ 2 analysis were performed to test the difference in modifiable risk measures between baseline and post-program periods at a statistical significance level of α = 0.05.
For each modifiable risk measure, the research team tested for a significant change in number of individuals who fell into a high-risk category before and after the program participation. In addition, the team performed a sensitivity analysis of change in modifiable risk factors by number of years of participation.
The Framingham CVD risk score and risk category also were calculated at baseline and post program. Baseline values were used to create a predicted post-program risk score based on a null hypothesis of no effect of the UR Wellness program, assuming no changes in individual behavior or other variables other than age. The predicted values were then compared with the individuals' actual risk scores post program participation. Change between predicted risk and actual risk also was examined by years of program participation.
The researchers further applied a logistic regression model to estimate the impact of participation in a condition management program and other factors on improvement of actual CVD risk over predicted risk based on Framingham scores. The multivariate analysis was restricted to only those participants who had greater than minimal CVD risk at baseline, because those with minimal risk at baseline had no opportunity to further decrease their risk category. SAS version 9.4 (SAS Institute Inc., Cary, NC) was used to manage and analyze the data.
Results
Table 1 describes the demographic characteristics of all individuals who participated in the UR Wellness program for more than 1 year and for whom there was complete information. The majority of study participants were white females who were married or living as married. Marital status and living arrangement is important here because being married or living as married has been linked to better health outcomes. 19 The vast majority of participants were not Hispanic and were highly educated, with almost 94% having a bachelor's degree or higher.
Demographic Characteristics of Program Participants
SD, standard deviation.
After applying the Framingham risk score calculations, individuals were classified into the 4 categories of CVD risk (low, moderate, high, or very high). Numbers of participants with greater than minimal risk at baseline are described in Table 2. Across all modifiable measures included in the Framingham score, there was a statistically significant decrease in the number of individuals in each high-risk category between baseline and post program participation. For example, the percentage of individuals who smoke decreased by 23.6% and the percentage of those with diastolic blood pressure ≥90 decreased by 41.7%. The sensitivity analysis by number of years of participation was not statistically significant because of insufficient sample size and therefore is not presented.
Health Risk Measures Comprising the Framingham Risk Score: At Baseline and Post Program *
Restricted to participants with CVD risk >1 at baseline (N = 1462).
CVD, cardiovascular disease; F, female; HDL, high-density lipoprotein cholesterol; M, male.
Table 3 shows the results of χ 2 analyses. First, the research team tested the difference between individuals' actual 10-year CVD risk score and their predicted risk score. Within each Framingham CVD risk category, the team found a statistically significant difference between the mean predicted 10-year risk score and the actual one. Overall, about 48% of participants with more than minimal risk improved their 10-year risk score over what was predicted without the program. Individuals originally in risk category 2 (moderate), 3 (high), and 4 (very high) achieved reductions in their actual risk of a cardiovascular event in the next 10 years of 14.7%, 19.9%, and 13.0%, respectively, over what had been predicted.
Change in 10-Year Cardiovascular Disease Risk Score and Category over Expected Risk After Program Participation
Statistically significant at P < .001, using a χ 2 test of independence.
CVD, cardiovascular disease.
Second, the team looked at the change in assignment to Framingham CVD risk categories and found that about one third of participants were able to reduce their Framingham CVD risk by a full category. These findings also were statistically significant. Similar to the previous sensitivity analysis, when the sample was split into groups by years of participation, the results were not statistically significant because of small sample size within the higher risk groups and are not presented.
In logistic regression, the relative influence of the program and other factors in addition to age on the actual 10-year CVD risk at the end of the program was examined. Multivariate analyses included 1462 individuals with baseline risk higher than minimal. The odds ratio estimates for statistically significant factors are shown in Table 4. Participation in a condition management program increased the odds of improving 10-year CVD risk by 36%, after controlling for other factors. In comparison to single males, being a married male increased the odds of improving CVD risk by 40%. Females (married or single) did not have a significant increase in odds of improvement as compared to single males. Models that included other demographic characteristics, such as race and education, also were estimated, but these factors were not statistically significant and therefore are not presented.
Logistic Regression Odds Ratio Estimates of Influences on 10-Year Cardiovascular Disease Risk Score Improvement over Predicted Risk (n = 1462)
Models that included other demographic characteristics, such as race and education, were estimated and were not found to be statistically significant.
Discussion
Reducing CVD risk is shown to improve health, reduce medical care spending, and increase quality of life. 15 Many employers offer wellness programs with the goal of improving the health of their employees and increasing productivity. 12,14,20 Measuring reduction in CVD risk is an effective method to evaluate program impact, particularly over time.
This study evaluated the long-term effects, over 1 year and up to 5 years, of the UR Wellness program on 10-year CVD risk. This study was able to demonstrate that participation in an employee wellness program with targeted engagement strategies and individualized coaching (during screening and subsequent condition management and lifestyle coaching) was associated with improvement in individuals' 10-year CVD risk score for almost half of participants who were at risk. Moreover, one third of all participants with more than minimal risk seemed to be able to reduce a full Framingham CVD risk category. The research team is not aware of any other program to date that had as large an apparent impact for so many individuals.
This study also provides insight into specific health risk measures that are modifiable and can be impacted by this type of program in order to reduce CVD risk. In fact, this wellness program appeared successful in reducing all modifiable risk factors, which included smoking status, total cholesterol, HDL, systolic blood pressure, and diastolic blood pressure. The Framingham CVD risk score consists of both modifiable and non-modifiable risk factors. This program was successful in not only targeting specific modifiable risk factors, but also in impacting overall CVD risk score, despite the presence of non-modifiable factors in the calculation of the score.
Although general engagement in a Personal Health Assessment and Wellness Engagement Plan appeared to have significant impact on individuals' CVD risk, deeper engagement in the program by participation in any condition management program increased the odds of improving the 10-year CVD risk. These findings are consistent with other studies in which participation in wellness programs reduced risk factors, especially among individuals who participated in more than 1 program. 21 It was interesting to find that marital status had a positive impact on CVD improvement for males, but not females. Being married or living as married increased the odds of reducing CVD risk for males. This reinforces the key role that spouses, especially women, play as caregivers and is consistent with previous studies. 22
Several studies have been conducted to evaluate whether worksite wellness programs are effective, including a recent article published by JAMA, in which the study conclusion suggests that a worksite wellness program is not effective in improving health outcomes or cost savings over 18 months. 23 An important distinction to consider is that there is no standard worksite wellness program design. In fact, the definition of what constitutes a wellness program is different for every employer and every wellness vendor.
The study published by JAMA described a program that delivered modular content that was educational but not customized to the individual health and lifestyle risk. In addition, realistic expectations of health- and cost-related outcomes need to be established when looking at programs over such a short period of time. Employers, employee benefits brokers, and insurance companies need to assess wellness programs by their performance and by their design. Clinically integrated, engaging, targeted interventions based on risk stratification have been demonstrated to be impactful in other studies. 16,24
Limitations
Several potential limitations of this study should be noted. First, several data elements were self-reported by the individuals. However, all health measures were obtained by a nurse during the biometric screening. Second, the sample included highly educated individuals (93% with college degree or above), who were mostly white (82%). Although this sample does not represent the general US population, distribution of their Framingham 10-year risk at baseline was comparable to those of the general population, as indicated in the Third National Health and Nutrition Examination Survey data. 25 The similarity in 10-year CVD risk between this study sample and the US adult population implies that present study findings may be generalizable to the US population if a similar program is administered.
Third, as with any quasi-experimental study design, this study was not able to control for any other interventions that individuals may have had during the time frame of study participation. The quasi-experimental design also may limit the generalizability of these results. However, this study design was found to be reflective of actual employees' responses to a wellness program and, therefore, very helpful when considered by employers, vendors, and payers. Fourth, individuals were followed for a maximum of 5 years, which may not be enough time to develop a CVD event. Further study is required to test the impact of this employee wellness program on reducing actual CVD events.
In addition, the Framingham CVD risk calculator itself, like all algorithms designed to estimate disease risk, has limitations. Although other risk calculators, such as the American College of Cardiology/American Heart Association (ACC/AHA), may have advantages over the Framingham calculator, they also have limitations, especially when applied to a working, healthy population. Elis et al found that the ACC/AHA risk score was significantly better at identifying high-risk patients; however, it was based on clinical presentation at the time of a first acute coronary event, which is not reflective of the population in the present study. They also found that none of the existing score algorithms was predictive of 5-year mortality. 26
The Framingham algorithm was selected for this study because it is widely used, often cited in the literature, and uses data elements that are able to be gathered during an employer-sponsored health screening (eg, this study's employer-based program cannot collect any family history data and does not measure kidney function or brain natriuretic peptide). Lastly, program participation was voluntary and individuals were provided a small financial incentive to participate. Voluntary participation may indicate higher engagement in health promotion activities.
The return on investment of different employee wellness programs is not yet clear. Although many studies show positive financial impact, many of them do not calculate return on investment. 24 Among those that calculate return on investment, there is a wide range of findings. As an example, while one team found a return on investment of $3.27 for every dollar spent on an employee wellness program, 16 another found the return on investment to be $1.65 for every dollar spent, 27 and a third study concluded that their reduction in individuals' annual health care spending was not enough to generate a positive return on investment. 28
Authors of a recent meta-analysis of 51 studies published over almost 30 years concluded that the size of the financial impact depends largely on the rigor of the study methods, and studies with higher methodological quality provided more modest evidence of return on investment. Future research should focus on return on investment from the payers' perspective.
Conclusion
The UR Wellness program seems to be effective in increasing employee wellness because of a combination of several factors. First, the program utilizes a multidisciplinary model; UR Wellness direct providers are a highly-skilled team of registered nurses, nutritionists, and fitness trainers dedicated to wellness. Second, the clinical program is based on a biopsychosocial framework that is supported by the UR Wellness web-based platform to enable individual coaching.
Additionally, being a clinically-integrated program, UR Wellness providers help participants establish a relationship with the health care system and provide bidirectional referrals and communications with primary care providers. The program also utilizes techniques that provide high rates of employee engagement and involves them as active participants in their own health and wellness. Third, founded in a School of Nursing, this UR Wellness program is evidence-based and theory driven. Lastly, the program is continually refined using outcomes and data analytics.
This study provides evidence from an employee wellness program that utilizes an integrated approach. The program was associated with statistically significant improvement in the cardiovascular health of participants. Almost half of all program participants with moderate-to-high risk at baseline improved their 10-year CVD risk, and about a third of participants improved by a full risk category. Engagement in a condition management program increased the odds of improvement by 36%.
Public health implications
An integrated approach to wellness improves the long-term health of participants and reduces their risk of developing CVD by achieving long-term improved lifestyle behaviors. Improved health increases quality of life and productivity, and reduces absenteeism and the demand for medical services, and hence, reduces overall health care spending. In addition, consideration should be given to adopting standard outcome measures that demonstrate program impact across the wellness industry, so that employers can compare and contrast different wellness programs based on their effectiveness. Further, employers and health benefits professionals should be able to evaluate wellness programs based on improved long-term health outcomes.
Footnotes
Author Disclosure Statement
The authors are all employed by the University of Rochester, which also funds the UR Wellness Program described in this study. However, their compensation was not dependent on the results obtained in this study, and the investigators retained full independence in the conduct of this research.
Funding Information
No funding was received for this article.