
Abstract
Hospital participation in stroke bundle programs presents financial risk. There are limited comparative data on the success of such programs. The authors aimed to assess the success of a management program in reducing the number of patients admitted to a skilled nursing facility (SNF), average length of stay, and the number of patients discharged to inpatient rehabilitation units. Three program metrics included reduction in number of stroke patients admitted to SNF, reduction in length of stay at SNFs, and reduced 90-day hospital readmission rates. The program was implemented during a 3-year period from October 1, 2015, through September 30, 2018, included 803 patients in the data, and demonstrated financial gain with positive patient outcomes. There was a 0.5% reduction in the number of stroke patients admitted to SNF. Sending patients home with a high-quality home care agency for rehabilitation and navigation assistance were the goals for this metric. A 1.65-day reduction in length of stay for overall SNF providers was noted. This was achieved by utilizing a preferred network of skilled facilities and community partners that the nurse navigator interfaced with weekly. The proportion of patients discharged to inpatient rehabilitee units was 2.2% less than in the baseline years. With the implementation of a stroke nurse navigator, hospital readmissions as a percentage of admissions for stroke decreased by 4%. Overall return on investment was greater than 400% after accounting for additional staffing and data/license fees.
Background
The Patient Protection and Affordable Care Act (ACA), enacted in 2010, was an instrumental catalyst for the Centers for Medicare & Medicaid Services (CMS) value-based programs. Hospital systems began to investigate different ways to provide quality patient care, increase efficient utilization of resources, and decrease health care expenditures. 1
In a traditional payment model, Medicare pays providers individually for services they render to beneficiaries, resulting in fragmentation and silos in the delivery of care.
The Center for Medicare & Medicaid Innovation launched the Bundled Payments of Care Improvement (BPCI) initiative in January 2013. Multiple payment models became available tying Medicare payment to value (Table 1). Bundled payments have the opportunity to align providers to deliver synchronous care for patients. The study hospital site chose Model 2. This model retrospectively focuses on the acute care hospital stay and includes post-acute care. There are incentives for providers for both cost and quality of care. Patients are included in the bundle program for 30–60–90 days as chosen by the acute care hospital. The acute care inpatient stay is the main trigger for the bundle and the 30–60–90-day count begins at hospital discharge. Stroke bundle patients are selected by Diagnosis-Related Groups (DRGs). Stroke was one of 48 clinical episodes to choose from for participation. 2
Centers for Medicare and Medicaid Services Bundled Payment Models
DRG, diagnosis-related group; MS-DRG, Medicare severity diagnosis-related group.
The aging population is not presenting new health care demands so much as it is presenting growing health care demands. From a population health perspective and in light of increasing health costs, the Institute for Healthcare Improvement (IHI) developed a structured framework (Triple Aim) to investigate new approaches that could be implemented in health care to optimize health (Figure 1). The Triple Aim consists of 3 dimensions: improve the patient experience, improve the health of populations, and reduce health care costs. 3
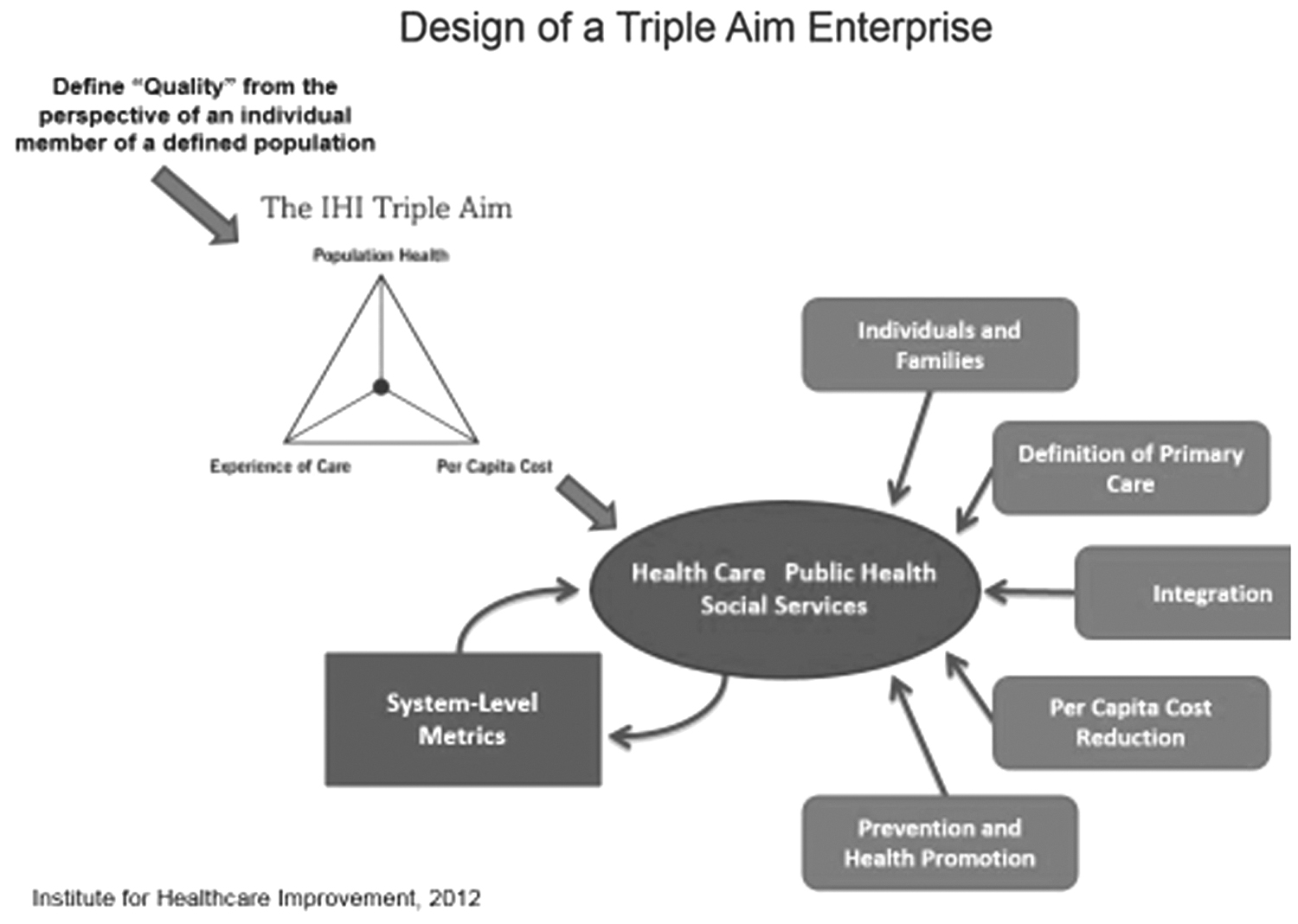
The IHI Triple Aim framework was developed by the Institute for Healthcare Improvement in Boston, Massachusetts (
The American Heart Association, Centers for Disease Control and Prevention, National Institutes of Health, and other government agencies such as CMS report the most up-to-date-statistics regarding heart disease, stroke, and cardiovascular diseases. Stroke affects approximately 795,000 people annually. 4
Benjamin et al 4 provide a succinct update on stroke statistics, financial burden, and socioeconomic loss. It is estimated that 7 million Americans aged ≥20 years self-report having had some type of stroke. Stroke remains the leading cause of serious long-term disability in the United States. Benjamin et al's projections demonstrate that by 2030, an additional 3.4 million US adults aged ≥18 years, reflecting 3.9% of the adult population, will have had a stroke. This is a 20.5% increase in prevalence from 2012 with the highest increase (29%) projected in white Hispanic males. 4
Direct and indirect cost of stroke includes direct medical costs. These costs encompass hospital inpatient and outpatient visits, office-based provider visits, emergency department visits, prescribed medicines, and home health care needs post discharge. According to Benjamin et al, total direct medical stroke-related costs are projected to more than double, growing from $36.7 billion in 2015 to $94.3 billion in 2035. 4
The aim of this study was to investigate the magnitude of success achieved during transition of care processes that used a stroke management program and concepts of the Triple Aim. As noted by Lichkus et al, this type of venture consisted of unknown financial risk and challenge. 5 The stroke bundle program was implemented at a comprehensive stroke center (CSC). Participation in the stroke bundle program offered an opportunity to promote additional secondary stroke risk reduction in stroke patients discharged to home without services, home care, acute inpatient rehabilitation, and skilled nursing facility (SNF). The program supported a structured framework for seamless transitions of care from admission, discharge, and post discharge. The program offered an opportunity to decrease hospital and SNF length of stay and readmission rates.
Methods
The CSC contracted with the CMS Stroke BPCI utilizing Model 2 in July 2015. Six skilled nursing facilities and the CSC team members collaborated closely on fostering strong cohesive teams, and developing stroke education programs, care transition protocols, and stroke clinical practice guidelines for SNF utilization. Three initiatives were incorporated into organizational strategic goals: reduction of the number of stroke patients who are admitted to a SNF by 5% (baseline 27.9%), reduction of preferred provider SNF average length of stay days for stroke patients by 10% (baseline 32.20%), and reduction of hospital 90-day readmission rate for stroke by 5% (baseline 31.5%).
Study population and study site
This project included all patients admitted to the CSC with stroke DRGs 61, 62, 63, 64, 65, and 66 over a 3-year period from October 1, 2015, through September 30, 2018; 803 patients were included in the data. The study site selected was a 604-bed acute care hospital that included a CSC, located in Abington, PA. The stroke center admits approximately 1000 patients a year. Medicare criteria were used for patient screening at the time of inpatient index admission. Clarification of a stroke bundle patient occurred post discharge, after confirmation of the primary DRG code.
Statistical analysis
Prior to the inception of the program, a strong process needed to occur to identify the correct population of patients. The hospital's neuroscience department has a dedicated stroke coordinator who manages all acute stroke admissions. Developing a methodology to identify the stroke bundle population upon hospital admission was challenging. The process relies on the stroke coordinator reviewing admitted patients who have had a neurology consult, the primary diagnosis of patients admitted to the neuroscience units, and a working DRG list that comes from the hospital clinical documentation team. The coordinator cohorts these patients using the stroke quality health indicator list and passes this information on to the stroke nurse navigator. The navigator uses this list to determine which patients are on Medicare, inputs their information into an Excel spreadsheet, and waits for final DRG coding to be assigned. Within the first few months of the program, the stroke nurse navigator recognized that patients who had a procedure while in the hospital were not assigned DRGs 61–66. This was a disappointment to stroke leadership as these patients would not have the benefit of a nurse navigator for 90 days post hospitalization. Reviewing the metrics after 1 year and then again annually for 3 years allowed the stroke team to gauge what processes were working and what needed improvement. It was clear that there was a fluctuation in patients admitted to SNFs and an increase in non-preferred provider SNF utilization post discharge. Comprehensive assessment of the data showed that these patients were admitted to the study hospital from various continuing care retirement communities and returned to the skilled portion of the community. Pre and post stroke bundle implementation data analysis was completed by using t tests and statistical control charts. Stroke bundle metrics and outcomes were very transparent and reviewed with all CSC team members and SNF leadership each month by the bundle program manager.
Interventions
A stroke bundle framework was necessary for developing processes and operations. The stroke bundle team collaboratively developed a program charter that included several components such as SMART (specific, measurable, achievable, realistic, and timely) goals, action plans, and outcome metrics. Daily communication processes were outlined in a flowchart format. SNF leadership meetings were refined and implemented on a monthly basis. One key factor identified to support this program was the requirement to hire a stroke nurse navigator. A “Kick Off” Stroke BPCI program took place on August 19, 2015 to educate and engage the CSC's multidisciplinary teams.
A stroke educational program – Care of the Stroke Patient: Key Concepts – was developed and presented to SNF multidisciplinary teams including senior leadership. In order to ensure ongoing stroke education at these facilities, the program was recorded and copied; each SNF received 5 DVDs. Standardization of stroke care was imperative to achieve SMART goals so a stroke clinical practice guideline was developed and initiated at the SNFs. Implementation of the BPCI program occurred October 1, 2015, and ended on September 30, 2018.
The stroke bundle team identified several key processes to support the concept of patient-centered care. Initiation of daily stroke rounds, consistent communication prior to discharge among the CSC, post-acute facilities, and home health care agencies was imperative. Ongoing conference calls among CSC and SNF teams was coordinated to review monthly metrics, discuss patient outcomes, and identify opportunities for improvement.
A full-time stroke nurse navigator was hired in October 2015. The stroke nurse navigator reports directly to the bundle program manager, providing clinical oversight to assure safe and effective transitions of the patient to the next level of care throughout the 90-day period following hospital discharge. The navigator coordinates care and works with physicians and all levels of acute and post-acute care providers, ensuring improved health status and positive patient outcomes while controlling health care expenditures across the continuum. This includes but is not limited to inpatient care, rehabilitation, skilled and assisted living facilities, outpatient programs, and home health agencies.
The stroke navigator meets patients prior to discharge to set the stage for follow-up discharge phone calls. Patients receive a 1-time postdischarge call while waiting for the final DRG code. Once this code is determined, further phone calls are made weekly for 90 days. Patient and caregiver are engaged to develop strategies to guide positive change and self-responsibility for managing the disease process. Goal setting, teach-back technique, and motivational interviewing are used as part of the discussion when speaking to patients. A color-coded zone management plan is developed and individualized to each patient's needs. If the patient is in the green zone, no action is needed at this time. If the patient is displaying signs and symptoms in the yellow zone, action is required that day which may involve a call to the homecare nurse, nurse navigator or physician. If patient symptoms are in the red zone, action is required immediately; the patient is instructed to call the physician or 911.
The key initiatives focused on during follow-up phone calls are: medication reconciliation and medication acquisition; review of hospital or facility discharge instructions; clinical assessment of the patient; and the ability to schedule and make primary and specialist physician follow-up appointments. The nurse navigator's outreach encompasses each patient in a holistic manner and initiates referrals to community agencies and services for patients to receive additional services. The handoff process occurs between the nurse navigator and post-acute teams. Effective and efficient communication is exchanged weekly and as needed during the 90-day bundle period. The patient is the central focus during transitions from one level of care to the next.
Tracking of metrics is completed in a designated electronic medical record and reports are pulled monthly and quarterly. Patient disposition, length of stay, as well as readmissions are SMART goals tracked for the purposes of the bundle program. Readmissions are reviewed in a prompt manner and patterns are considered. The navigator keeps ongoing documentation of “good saves,” which are shared with the stroke and senior leadership teams to create awareness and change current processes.
Results
The stroke bundle program improved clinical outcomes, patient engagement, and sustained financial value. A significant reduction in the number of stroke patients admitted to a SNF, reduction in length of stay at a SNF, and 90-day hospital readmissions were demonstrated (Table 2).
Stroke Bundle Dashboard
CMS, Centers for Medicare & Medicaid Services; NP, non preferred provider; PP, preferred provider; SNF, skilled nursing facility.
The stroke bundle program links payments for the acute stay and all post-acute services during an episode of care with financial and performance accountability. CMS established a baseline target price for all care during an episode based on the 2009–2012 actual experience for a provider. Improving post-acute readmission rates and SNF length of stay (ie, decreasing the cost borne by CMS and improving outcomes) are 2 of the main drivers that will generate savings to the bundle program. The program is designed to share the savings with providers or, conversely, to recoup a portion of the costs when costs exceed the target price (Table 3). Overall return on investment: >400%. Abington – Jefferson Health's results for the stoke bundle program have shown an average decrease of 9.3% in cost of care compared to the baseline target price over the life of the BPCI program.
Financial Investment
CMS, Centers for Medicare & Medicaid Services; NA, not applicable.
Discussion
Strong leadership and dedication in the acute care setting and SNFs closed the gaps that occur between patient care, communication processes, and patient follow-up. Clear and concise communication processes continue to foster strong and trusting relationships for all interrelated inpatient and community partners in the bundle program. Standardization of stroke care guidelines reflected decreased variation of patient care and improved patient outcomes. Inclusiveness of all team members and openness to operational transparency transformed a culture that worked in silos to a culture that works as a team. Positive patient feedback notes appreciation of the stroke nurse navigator's ongoing phone calls and follow-up.
SNF patient care processes and operational improvement contributed to the success of the stroke bundle program. Implementation of postdischarge monitoring tools (ie, readmission), standardization of care (clinical practice guidelines), and assessment of day and time of hospital admission and discharge supported all stroke bundle goals. Standardized handoff processes among physicians and nurses and concise documentation in the medical record supported a collaborative communication process. It is important to note that one of the SNFs realized the positive impact of advanced practice nurses and invested in hiring more practitioners to support the bundle program.
Limitations
The stroke bundle program only incorporated DRGs 61–66, omitting 67–69. In addition, primary stroke diagnosis was not considered; those patients who had procedures related to a stroke were not coded for the stroke bundle. The DRG was assigned the procedural code, not the stroke code.
Conclusion
A stroke bundle program positively affected transitions of care at 6 SNFs through standardization of care at SNFs, hiring a stroke nurse navigator, stroke education, and ongoing team communication. A BPCI Stroke Bundle Program has the opportunity to improve clinical outcomes, patient engagement, and sustained financial value: reduction in the number of stroke patients admitted to a SNF, reduction of preferred provider SNF days, and reduction in number of hospital readmissions for stroke. This program transformed Abington – Jefferson Health from a volume-based fee-for-service institution to an organization capable of managing the health and wellness of select populations.
Footnotes
Acknowledgment
We acknowledge and thank Lisa Clauson, Abington Hospital – Jefferson Health, for all graphic and file support.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.