
Abstract
The objective was to assess the association of Medicaid coverage gaps with health care resource utilization (HRU) and costs of patients with schizophrenia. Patients with schizophrenia were identified from the Medicaid database. The beginning of the first eligible gap was defined as the index date. Per-patient per-month (PPPM) HRU and costs before versus after a gap were assessed, and the association between gap duration and PPPM HRU and costs was examined up to 12 months post index. Together with 95% confidence intervals, HRU differences were reported in rate ratios (RRs), and cost differences were reported in 2016 US dollars. A subgroup of males with substance use disorder (SUD; risk factors for incarceration) also was analyzed. Total PPPM health care costs increased significantly by $711.04 following a coverage gap (P < 0.001). Gaps of 180–365 days were associated with a significant increase in inpatient visits (RR = 1.27; P < 0.001) relative to gaps of <90 days. Gaps of 90–179 days were associated with significantly more PPPM inpatient visits (RR = 1.14; P = 0.024) relative to a gap of <90 days. Inpatient costs were particularly increased for gaps of 180–365 days versus those of <90 days (cost difference = $101.81 PPPM; P = 0.0008). Similar results were found in male patients with SUD, in whom HRU and cost differences appeared larger. In patients with schizophrenia, longer Medicaid coverage gaps were associated with increases in inpatient admissions, emergency room visits, and inpatient costs, particularly among patients with risk factors for incarceration. These results support policies that aim to facilitate Medicaid reinstatement for patients with schizophrenia.
Introduction
Schizophrenia is a chronic mental disorder characterized by several psychological symptoms, including repetitive psychotic episodes during which the patient experiences hallucinations. 1,2 It has been shown that a larger proportion of Medicaid beneficiaries have schizophrenia compared to patients with other types of insurance coverage. 3 The prevalence of schizophrenia among Medicaid beneficiairies younger than age 65 has been estimated to be more than 12 times higher than that of privately-insured patients and twice as high as that of Medicare-insured patients. 3
Mentally ill patients are more likely to be arrested and incarcerated than the general population, presumably because they experience symptoms that may alter their behavior. 4 The prevalence of schizophrenia in correctional facilities is estimated at 2%–6.5% compared to less than 1% in the US general population. 5 –7 Jails and prisons might have limited resources to treat psychiatric illnesses, which can worsen the patient's condition. 8,9 Furthermore, incarceration leads to either termination or suspension of Medicaid coverage, depending on the policy in effect in a particular US state, and may be one of the key reasons that causes gaps in health insurance coverage for such mentally ill patients. In particular, in states where Medicaid coverage is terminated and without programs to facilitate reinstatement, coverage has to be reinstated by the released inmate. This administrative process can take 45 to 90 days, during which individuals are left without any health insurance. 10 These gaps may be even longer in inmates who may not have Medicaid reinstated until they have some health issue resulting in an emergency room (ER) visit or hospitalization.
In 2003, Harman et al demonstrated that gaps in Medicaid coverage were associated with significantly greater utilization of inpatient psychiatric services among patients with schizophrenia, based on data for the period of 1990–1994. 11 Besides these data being outdated, the study is also limited by the fact that it was restricted to the state of Utah, and changes in utilization of other medical services and health care costs related to Medicaid coverage gaps were not assesed. Thus, there is a need for a more comprehensive and updated assessment of the economic outcomes associated with Medicaid coverage gaps in US states where the termination policy is still in effect.
The present study aimed to address this research question by examining the association between gaps in Medicaid coverage with health care resource use (HRU) and costs for patients with schizophrenia using data from multiple state Medicaid programs that have a policy to terminate coverage upon incarceration. Because Medicaid claims data do not provide reasons for gaps in coverage, the primary objective examined the association of the presence and duration in coverage gap with HRU and costs by focusing on all Medicaid patients with schizophrenia with a coverage gap. The secondary objective attempted to further evaluate the association of gaps related to incarceration with HRU and costs by examining a subset of patients with schizophrenia who are at risk for incarceration (ie, males with substance use disorder [SUD]). 12 For both objectives, monthly HRU and costs incurred by patients were compared before and after the coverage gap; the association between the duration of the coverage gap and monthly HRU and costs also was examined.
Methods
Data source
Four states in which Medicaid coverage was terminated upon incarceration during the data period were included. For each state, the data periods evaluated (5 most recent years, depending on data availability) were selected such that only years during which the termination policy was in effect were considered. These states included Kansas (2012 quarter [Q]2-2017 Q1), Mississippi (2012 Q2-2017 Q1), Missouri (2012 Q2-2017 Q1), New Jersey (2009 Q2-2012 Q4), and Wisconsin (2009 Q1-2013 Q4). Medicaid data contain information on patient demographics, Medicaid enrollment history, prescription drug claims, and detailed medical claims (ie, physician visits, hospitalizations, long-term care [LTC], and other services reimbursed by Medicaid; diagnoses and procedures; dates of service; Medicaid payments; patient out-of-pocket costs, co-payments, and deductibles). In addition, the database contains information on Medicaid payments made under both the fee-for-service and managed care systems, patient out-of-pocket costs, and Medicare co-payments and deductibles. All available cost data reflect the Medicaid payers' perspective prior to any discounts or rebates paid by manufacturers. The claims data for specific individuals are encrypted and comply with the Health Insurance Portability and Accountability Act. Thus, institutional review board approval and informed consent were not needed for this study.
Study design and patient selection
A retrospective longitudinal cohort study was conducted to examine the impact of coverage gaps on subsequent health care outcomes (Figure 1). Monthly HRU and costs for patients with schizophrenia were compared before and after a coverage gap. Also examined was the association between the duration of the coverage gap and monthly HRU and costs. Thus, study outcomes were evaluated both during the baseline and observation periods.
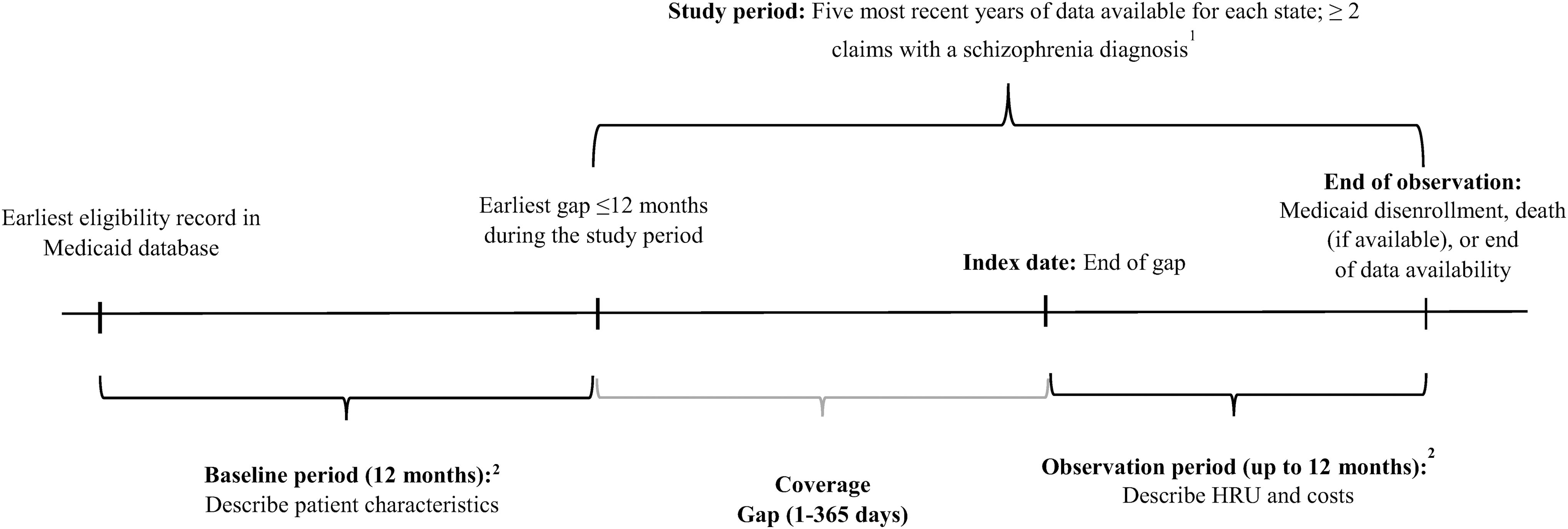
Study design scheme.
Patients included in the study were required to have ≥2 schizophrenia diagnoses (International Classification of Diseases, Ninth Revision, Clinical Modification code 295.xx [schizophrenic disorders] or International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] codes F20.xx [schizophrenia], F21 [schizotypal disorder], F25.x [schizoaffective disorders]) during the years of data available for a given state. Additional inclusion criteria were as follows: a gap in Medicaid coverage of ≤12 months, ≥12 months of continuous Medicaid coverage before the gap and after the index date (definition follows), and ≥18 years of age as of the date of the Medicaid re-enrollment record following the first eligible coverage gap (defined as the index date). The 12-month periods preceding and following the gap were defined as the baseline and observation periods, respectively. To examine the association between the duration of the Medicaid coverage gap and monthly HRU and costs, gaps were categorized by duration of 1–89 days, 90–179 days, and 180–365 days based on the frequency of the gap categories.
Because reasons for gaps in coverage are not available in Medicaid data, a subset of patients with schizophrenia who are at high risk of incarceration was selected. More specifically, given that male sex and SUD increase the risks of delinquency, 12 –14 a subsample of male schizophrenia patients with SUD (hereinafter referred to as the male-SUD subset) was analyzed separately. The definition of SUD included many alcohol-related and drug dependence-related diagnosis codes, among others (see Table 1 for more details).
Baseline Demographic and Clinical Characteristics in the Overall Population and in the Subset of Male Patients with Substance Use Disorder
1. SUD diagnosis included alcohol dependence syndrome; drug dependence; nondependent abuse of drugs; alcohol-induced mental disorders; drug-induced mental disorders; drug dependence complicating pregnancy, childbirth, or the puerperium; mental and behavioral disorders related to psychoactive substance use; abuse of nonpsychoactive substances; alcohol use complicating pregnancy, childbirth, and the puerperium; drug use complicating pregnancy, childbirth, and the puerperium; pharmacological therapy indicators (methadone; levo-alpha-acetyl-methadol [LAAM]; antabuse [disulfiram]; naltrexone; naloxone; clonidine; bupropion; psychiatric Medication; other replacement medication; buprenorphine); and nonpharmacological therapy indicators (SUD-related rehabilitation and detoxification; SUD-related psychotherapy and counselling).
2. Included typical agents (aripiprazole, aripiprazole lauroxil, asenapine, brexpiprazole, clozapine, cariprazine, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine, risperidone, ziprasidone) and atypical agents (acetophenazine, chlorpromazine, chlorprothixene, flupentixol, fluphenazine, haloperidol, levopromazine, loxapine, mesoridazine, methotrimeprazine, molindone, pericyazine, perphenazine, promazine, thioridazine, thiothixene, thioproperazine, trifluoperazine, triflupromazine, zuclopenthixol).
AP, antipsychotic; FGA, first-generation; LAI, long-acting injectable therapies; OAP, oral antipsychotic; Quan-CCI, Quan-Charlson comorbidity index; SD, standard deviation; SGA, second-generation; SUD, substance use disorder.
Study outcomes
All-cause per-patient per-month (PPPM) HRU was evaluated and included outpatient visits, inpatient visits, ER visits, mental health institute (MHI) admissions, and LTC admissions. Health care costs also were assessed and stratified into the same aforementioned categories. Costs were reported in 2016 US dollars using the medical care component of the consumer price index. 15
Data analytic procedures
Means and standard deviations (SDs) were used to describe continuous variables, frequencies and percentages were used to describe categorical variables. These descriptive statistics were used to assess the within-patient difference in health care costs between the baseline and observation periods in both the overall study population and in the male-SUD subset. A generalized estimating equation model with patient as a repeated measure was used to compare HRUs and costs within patient before and after a gap. Confidence intervals (CIs) and P values were estimated from a nonparametric bootstrap procedure (499 resamples).
In separate analyses, the association between the duration of the gap in coverage and outcomes was assessed with unadjusted and adjusted models. The duration of the gap was included in the models as a set of categorical variables: <90 days (reference), 90–179 days, and 180–365 days. Adjusted models controlled for the following baseline characteristics, including mental health-related variables: gap duration category (variable of interest), age, sex, race, state, region, index year, insurance type (ie, capitated; dual eligibility for Medicaid and Medicare), Quan-Charlson comorbidity index, 16 diagnosis of SUD, diagnosis of hypertension, diagnosis of depression, diagnosis of bipolar disorder, use of antipsychotics (any type), use of antipsychotics (any long-acting type), use of antidepressants, use of anxiolytics, use of mood stabilizers, numbers of baseline outpatient, baseline ER, and baseline inpatient visits, total baseline medical costs, and total baseline pharmacy costs.
The association of the duration of the gap with HRU was estimated using Poisson models with a log-link. Results were reported as rate ratios (RRs). CIs and P values were estimated from a nonparametric bootstrap procedure (499 resamples). The association of the duration of the gap with costs was estimated using 2-part generalized linear models (GLMs). The first part was a logistic regression estimating the probability of having a positive cost value on the outcome of interest. The second part estimated the cost difference among those with a positive cost value. The GLM model family (ie, Gaussian, Inverse Gaussian, continuous Poisson, Gamma) and link power function in the second part of the 2-part model were selected based on diagnostics, including the modified Park's test and the Akaike's Information Criterion. 17,18 CIs and P values were estimated from a nonparametric bootstrap procedure (499 resamples). All analyses were performed using SAS Enterprise Guide 7.11 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and clinical characteristics at baseline
Of 97,033 patients with ≥2 diagnoses of schizophrenia, 24,177 (24.9%) had a gap in Medicaid coverage of ≤12 months, and 6400 (6.6%) met the remaining study selection criteria. Most included patients were from Missouri (Table 1, Supplementary Table S1). The mean age was 42.5 years, and more than half of patients were male and white (Table 1). Overall, 37.3% of the patients had SUD during the baseline period. Nearly half of patients had a coverage gap of <90 days, and more than one quarter had a gap of 90–179 days or a gap of 180–365 days (Table 1). A total of 1443 patients were included in the male-SUD subset, representing 22.5% of the overall study population (Table 1). In this subset, baseline characteristics were similar to those in the overall sample with a few notable differences: mean age was lower, and the proportions of patients with a diagnosis of psychosis, depression, and use of any antipsychotic were higher (Table 1).
Health care costs before and after a gap in Medicaid coverage
In the overall population, total PPPM all-cause health care costs were $711.04 (95% CI = $625.24, $794.30) higher during the observation period (ie, following the gap) compared to the baseline period (P < 0.001; Table 2). Nearly 90% of the total cost difference could be attributed to institutional costs, which comprised inpatient, ER, MHI, and LTC costs (Table 2).
All-Cause Health Care Costs Per Patient Per Month During the 12-Month Observation Period Compared to the 12-Month Baseline Period 1
: P < 0.05
1. The within-patient difference (before and after gap in Medicaid coverage) was estimated using a generalized estimating equation model with patient as a repeated measure; confidence intervals and P values were estimated from a nonparametric bootstrap procedure (N = 499).
diff, difference; CI, confidence interval; ER, emergency room; IP, inpatient; LTC, long-term care admissions; MHI, mental health institute admissions; OP, outpatient; PPPM, per patient per month; SD, standard deviation; SUD, substance use disorder.
In the male-SUD subset, total baseline costs were numerically higher than those of the overall population (male-SUD = $1239, overall = $895; Table 2). Similar to the overall population, total costs also increased significantly from the baseline to the observation period (P < 0.001; Table 2). The most important driver of medical costs was institutional costs (P < 0.001), including inpatient (P = 0.188), ER (P = 0.004), MHI (P < 0.001), and LTC costs (P < 0.001; Table 2).
Association of gap in Medicaid coverage with HRU and health care costs
Unadjusted results for HRU and costs by the duration of the coverage gap for the main sample and SUD subsample are presented in Supplementary Tables S2, S3, S4. Adjusted models revealed that coverage gaps were associated with an increase in inpatient visits. Shorter gaps (90–179 days) were associated with a numerical increase (RR [95% CI] = 1.14 [1.00, 1.31], P = 0.056), while longer gaps (180–365 days) were associated with a statistically significant increase (P < 0.001; Figure 2) relative to gaps of <90 days. In terms of inpatient costs and still relative to gaps <90 days, gaps of 90–179 days were associated with numerically higher PPPM costs (cost difference [95% CI] = $53.02 [$-18.24, $126.11], P = 0.116), a difference further and significantly increased when gaps of 180–365 days were considered (P = 0.008; Figure 3).
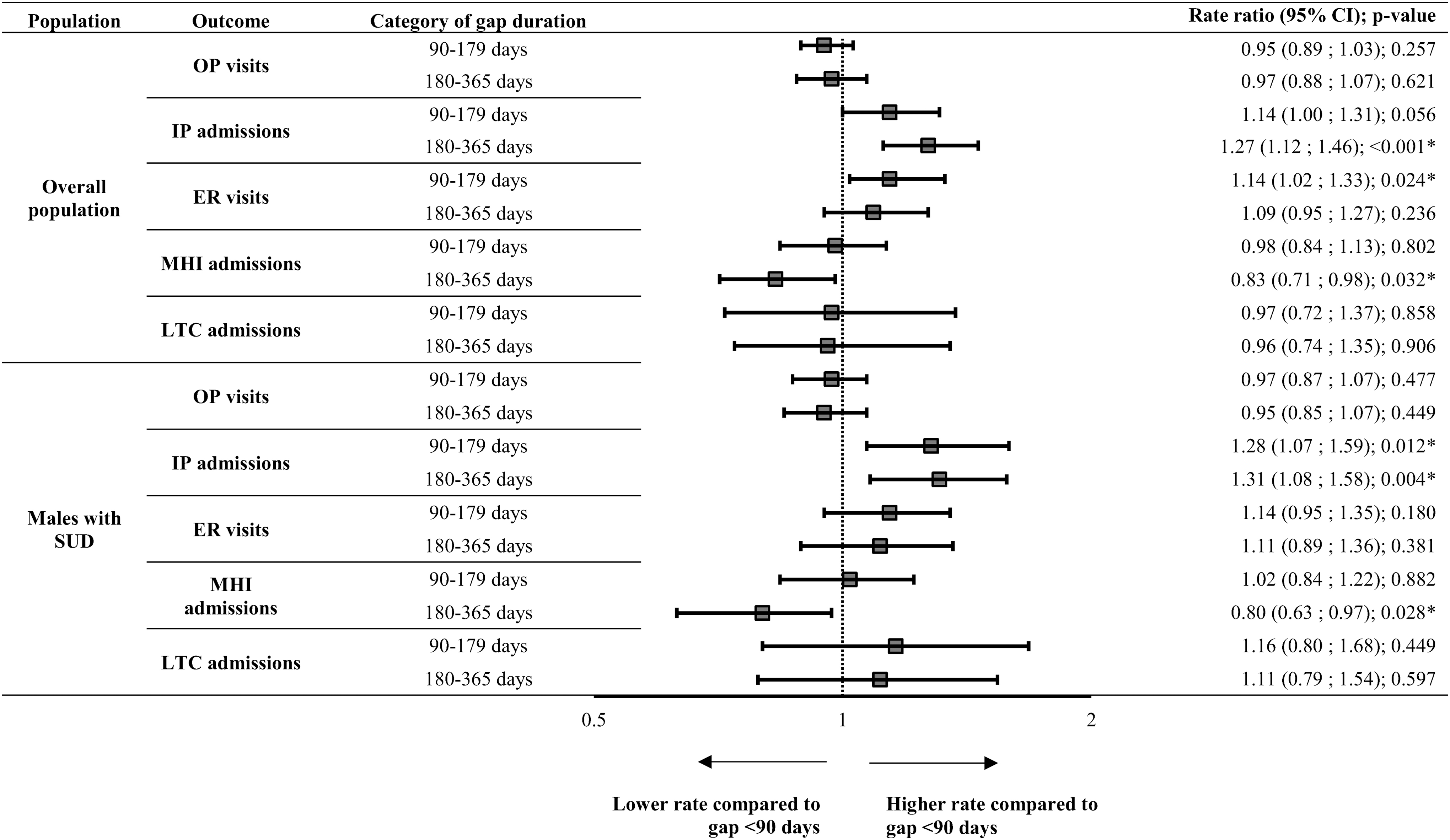
Association of Medicaid enrollment gap duration with health care resource utilization (number of visits PPPM) during the 12-month observation period for patients with schizophrenia (compared to gap <90 days, adjusted model 1 ).
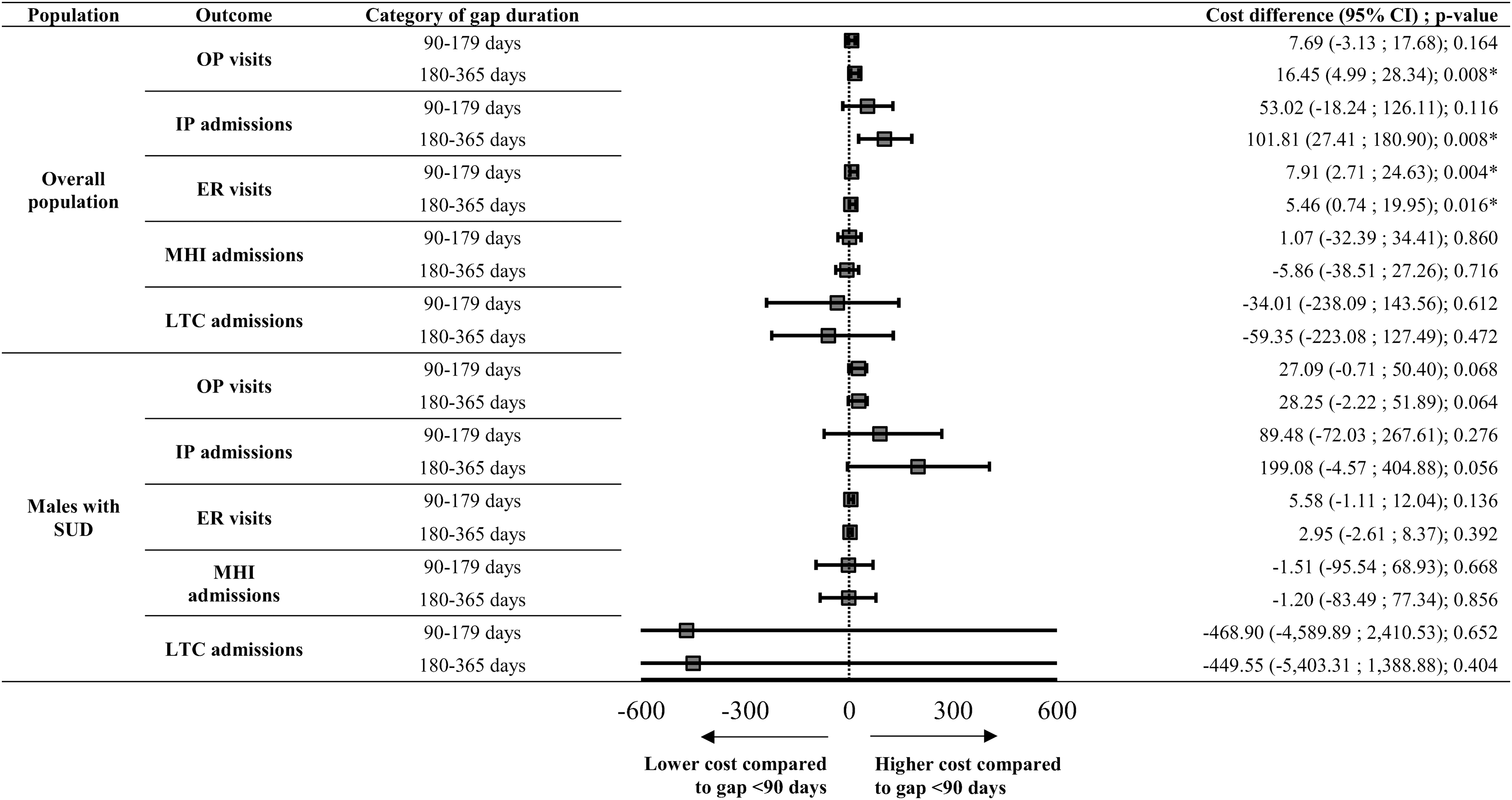
Association of Medicaid enrollment gap duration with health care costs PPPM during the 12-month observation period for patients with schizophrenia (compared to gap <90 days, adjusted model 1 ).
With respect to ER visits, a gap of 90–179 days was associated with significantly more ER visits PPPM (P = 0.024) relative to a gap of <90 days in the adjusted model (Figure 2). However, statistical significance was not reached when comparing gaps of 180–365 days versus <90 days (P = 0.236; Figure 2). A similar trend was observed for ER costs in adjusted models: gaps of 90–179 days (P = 0.004) and gaps of 180–365 days (P = 0.016) were associated with significantly higher ER costs relative to gaps of <90 days (Figure 3).
With regard to outpatient visits, there was no significant association between gap duration and the number of visits (Figure 2). Gaps of 90–179 days were associated with a numerical increase in outpatient costs as compared to gaps of <90 days. The increase was larger and statistically significant for gaps of 180–365 days (P = 0.008; Figure 3).
Relative to gaps of <90 days, gaps of 180–365 days (P = 0.032) were associated with significantly fewer MHI admissions; however, no association was found for gaps of 90–179 days (P = 0.802; Figure 2). Gap duration was not associated with statistically significant differences in MHI costs in adjusted analyses (Figure 3), whereas unadjusted analyses revealed a significant difference for gaps of 90–179 days (cost difference [95% CI] = -$95.76 [-$157.01, -$44.75], P = 0.004; Supplementary Table S2).
An increasing gap duration was not associated with a change in the number of LTC admissions (Figure 2). With respect to LTC costs, statistical significance was not reached (Figure 3), although adjusted analyses numerically trended toward longer gaps being associated with lower costs.
Subset of male patients with SUD
Similar results were generally found in the male-SUD subset, although a few statistically significant differences observed for the overall population were not found in this subpopulation (Figures 2–3; Supplementary Tables S2, S3, S4). Notwithstanding statistical significance, the magnitude of many differences generally appeared more pronounced when increasing gap duration in this subgroup as compared to the overall population (Figures 2–3; Supplementary Tables S2, S3, S4). Notably, gap durations of 90–179 days and 180–365 days were associated with a significantly higher use of inpatient visits compared to gaps of <90 days (Ps <0.05) in adjusted models (Figure 2). Furthermore, gap durations of 90–179 and 180–365 days were associated with higher PPPM inpatient costs compared to gaps of <90 days (Figure 3).
Discussion
In this retrospective claims-based study, changes in HRU and costs of patients with schizophrenia were evaluated, and the association between the duration of the Medicaid coverage gap and these outcomes was assessed. The results of the before–after analysis showed that total health care costs increased by $711.04 PPPM following a coverage gap in the overall population, with institutional visits – mostly LTC admissions – acting as a major driver of this cost difference. This result suggests that, after a gap in coverage, most of the increase in total health care costs is driven by higher costs related to LTC admissions.
In a separate analysis comparing patients with varying gap durations, coverage gaps of 90–179 days were associated with more ER visits as compared to gaps of <90 days. Longer gaps of 180–365 days were associated with more inpatient admissions, and less MHI admissions versus gaps of <90 days. The impact on costs appeared particularly pronounced for inpatient costs, as gaps of 180–365 days versus <90 days were associated with an increase in costs of $101.81 PPPM. In the subset of male patients with SUD, similar conclusions could be drawn, and an increasing duration of the coverage gaps appeared to have a more pronounced impact relative to that observed in the overall population.
In 2003, Harman et al showed that gaps in Medicaid coverage in the state of Utah were associated with greater use of inpatient psychiatric services among patients with schizophrenia based on data collected in 1990–1994. 11 Harman et al evaluated the impact of having versus not having gaps in Medicaid coverage of ≥2 months on hospital admissions and hospitalization days, whereas the present study evaluated patients before versus after they had a gap and also performed analyses to assess the impact of different gap durations. Even though Harman et al's data were collected more than 25 years ago and in spite of the aforementioned differences in study designs, the results presented here suggest these conclusions still hold true for contemporary patients with schizophrenia. Furthermore, by providing more granularity on HRU categories other than inpatient psychiatric services and cost data, the current study expands and updates the findings of Harman et al.
Although reasons for a gap in Medicaid coverage could not be determined using Medicaid claims data, a subset of patients with schizophrenia having 2 well-established risk factors for incarceration – male sex and SUD 12 –14 – was used to select patients at high risk of incarceration. In fact, the prevalence of substance use among incarcerated individuals with schizophrenia is about 70%, 19 and approximately 90% of inmates are male. 20 In this subset and for the analysis comparing patients with different gap duration, results were generally similar to those in the overall sample, but the magnitude of the differences appeared particularly more pronounced for inpatient HRU and inpatient costs. For example, the difference in PPPM inpatient costs associated with a gap of 180–365 days versus <90 days was almost double that observed in the male-SUD subset ($199.08) as compared to the overall population ($101.81). These results suggest longer coverage gaps may have a more important impact on HRU and costs among incarcerated patients with schizophrenia, although this constitutes preliminary evidence that would require further validation.
A clear pattern that emerged from the analyses performed in the current study was related to inpatient HRU and costs, which both increased with longer gap durations. This potentially signals barriers in access to routine specialized medical care related to an absence of coverage. An inpatient admission might trigger a renewal of Medicaid coverage, but these visits are associated with costs that are substantially higher than those of routine specialized care. 11 Administrative barriers in access to routine medical care have been shown to be associated with an increase in the odds of incarceration for patients with schizophrenia. 21 Jail detainees with severe mental illness (ie, schizophrenia, psychotic, delusional disorder) and without Medicaid enrollment also were shown to be at higher risk of subsequent detention than those with Medicaid enrollment. 22
This study suggests that implementation of policies that aim to facilitate the reintegration of mentally ill patients in the Medicaid system after disenrollment may be beneficial for both the patient and the health care system. The suspension (rather than termination) of Medicaid coverage following incarceration is one such policy that is already adopted by a majority of states. 23 Of note, some states, including Arizona, Massachusetts, and Connecticut, went even further by adopting other measures, such as the enrollment of incarcerated individuals prior to their release. 23 Anecdotal evidence suggests these policies translated into better access to health care and gains in administrative efficiency. 23
The current study provides the most recent evaluation of the economic impact of Medicaid coverage gaps in patients with schizophrenia, both overall and among patients with risk factors for incarceration. Previous estimates pertaining to this research question were outdated, restricted to 1 state, focused on inpatient HRU, and did not include a subset of patients at risk for incarceration. 11 The updated cost estimates provided herein should thus be valuable to inform policy makers on the impact of the termination policy on individuals with schizophrenia, particularly among those incarcerated.
Furthermore, the results presented herein may be useful in understanding the economic burden of different vulnerable patient populations. Indeed, in other populations who also are overrepresented in correctional facilities, 9,24 gaps in Medicaid coverage also may lead to additional distress and an increased economic burden. The applicability of these findings to such populations remains to be explored, but constitutes an interesting venue of future research.
Limitations
The present study is subject to some limitations. First, the reasons behind the gap in Medicaid coverage could not be determined and selecting male patients with SUD may be a suboptimal approximation of the risk of incarceration. Nonetheless, this was necessary as jail/prison records cannot be readily linked to Medicaid claims. Second, as the objective of the present study was to evaluate the impact of the duration of health insurance gaps (ie, not the total burden of coverage gaps), the study did not include a control group of patients without any coverage gaps when evaluating how HRU and costs differed before versus after a gap. Third, as with most claims-based studies making use of large databases, results of this retrospective study can be affected by coding entry errors, missing data in the database, and residual confounding. However, this is expected to impact all gap categories analyzed equally. Fourth, costs were based on Medicaid payers' perspectives and reflected amounts paid by state Medicaid programs; therefore, out-of-pocket and direct nonmedical costs from the patient's perspective were not evaluated. In addition, these amounts do not take into account discounts or rebates; therefore, pharmacy costs may have been overestimated. Finally, because of the observational nature of the current study, results should be interpreted as associations between different variables and not as causal relationships.
Conclusion
The results of this study show that total direct all-cause health care costs increased significantly by $711.04 PPPM after, compared to before, a gap in Medicaid coverage among patients with schizophrenia. In addition, increasing the duration of a coverage gap was associated with a significant increase in the number of inpatient admissions and ER visits. The impact on costs appeared particularly pronounced for inpatient costs, as gaps of 180–365 days versus <90 days were associated with an increase in costs of $101.81 PPPM. Similar conclusions were drawn in a subset of male patients with SUD, which was used to target individuals at high risk of incarceration. These results advocate the need for policies that aim to facilitate the reintegration of Medicaid coverage after temporary interruptions for patients with schizophrenia. More research is needed on the effect of terminating Medicaid coverage on incarcerated individuals with schizophrenia.
Footnotes
Acknowledgments
Assistance with preparation of tables and figures was provided by Kazi Ahmed, and medical writing assistance was provided by Samuel Rochette, both from Analysis Group, Inc., a consulting company that provided paid consulting services to Janssen Scientific Affairs, LLC. for the development and conduct of this study and manuscript.
Author Disclosure Statement
Mr. Pilon, Dr. Manceur, Ms. Zhdanava, and Mr. Lefebvre are employees of Analysis Group Inc., a consulting company that provided paid consulting services to Janssen Scientific Affairs, LLC for the development and conduct of this study and manuscript. Dr. El Khoury and Ms. Benson are employees of Janssen Scientific Affairs, LLC and Johnson & Johnson stockholders. Dr. Doshi served as a consultant to Janssen Scientific Affairs, LLC.
Funding Information
This research was funded by Janssen Scientific Affairs, LLC.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.