
Abstract
Understanding the relationships between discharge disposition, readmissions, and cost of care is an important strategy for Accountable Care Organizations (ACOs) with aspirations to achieve shared savings. The purpose of this retrospective cohort study is to examine whether there is an association between the discharge dispositions of home with home health (HH) compared to skilled nursing facility (SNF) and the readmission rate and cost of care for Medicare ACO patients discharged from the hospital. The authors studied the variables associated with readmission rates and cost of care, including discharge disposition and risk score for 1151 patients attributed to an ACO. In multivariate logistic regression analysis, variables associated with increased risk for 30-day readmission were the Centers for Medicare & Medicaid Services Hierarchical Condition Category risk score and the discharge setting. Discharges to SNF were almost 5 times more likely to be readmitted to the hospital at 30 days compared to patients discharged to the HH setting. The cost of care is lower for the HH discharge disposition, with an $8678 per patient difference between the cost of care for patients discharged to HH and SNF levels of care. Findings from this study suggest that employing a transitional care planning approach that prioritizes discharging patients to the least restrictive next site of care, shifting patients from SNF disposition to HH as appropriate, is an effective strategy to improve readmission rates and cost of care.
Introduction
Understanding the relationships between discharge disposition, readmissions, and cost of care is an important strategy for Accountable Care Organizations (ACOs) with aspirations to achieve shared savings. Health care reform has driven a paradigm shift that centers on accountability for both cost and quality of care, appealing to ACOs to improve population health management approaches. 1 The purpose of this study is to examine whether there is an association between the discharge dispositions of home with home health (HH) compared to skilled nursing facility (SNF) and the readmission rate and cost of care for Medicare ACO patients discharged from the hospital. Prior research has suggested that post-acute care disposition and readmissions drive variance in Medicare spending post hospitalization. This study adds to emerging evidence that supports the advantages of discharging to the least restrictive next site of care following hospitalization.
Health care reform was introduced by the Patient Protection and Affordable Care Act (PPACA) in 2010, incorporating the ACO framework and Hospital Readmissions Reduction Program as 2 of the fundamental elements. 2 This framework created the opportunity for ACOs to share in savings resulting from the provision of high-quality care for a population at a total cost that is below a defined target.
Readmission prevention continues to be an area of focus to reduce avoidable cost, as readmissions account for a significant portion of the total cost of care for some conditions. 3 In the Healthcare Cost and Utilization Project Statistical Debrief, Medicare beneficiaries represented 55.9% of total readmissions in the United States and all-cause 30-day readmissions accounted for an estimated $24 billion in Medicare cost. 4 The Hospital Readmissions Reduction Program affects reimbursement to hospitals for care provided, adjusting compensation based on the occurrence of readmissions compared to the anticipated rate. 5 ACOs and hospitals are motivated by PPACA programs to analyze readmission-related data to understand the variables that correlate with increased readmission rates and subsequent total cost of care.
ACOs endeavor to ensure that patients receive the right care at the right time while supporting the prudent use of Medicare benefits, in alignment with the value-based aims of health care reform. There has been a significant shift in post-acute care utilization in recent years, contributing to a considerable increase in Medicare post-acute care spending on services provided in the SNF level of care. Between the years 2006 and 2014, SNF payments contributed to 5% of total Medicare cost. 6 This is reflective of the increased rate of discharge to post-acute facilities, as there were approximately 1.2 million more discharges to post-acute care facilities in 2010 compared to 1996. 7
The reasons for this trend are multifaceted. Hospitals are enticed by financial incentives to discharge patients early through the prospective payment system. 8 Prior research has shown that patients with a briefer index hospital length of stay are more likely to be discharged to a post-acute facility. 7 Confounding this issue is a lack of standardized criteria to guide discharge disposition decisions, resulting in variability in rates of referrals to post-acute services for similar conditions. 9 This study explores the association between discharge dispositions of home with home health (HH) compared to skilled nursing facility (SNF) and the readmission rate and cost of care for Medicare ACO patients discharged from the hospital.
Methods
This retrospective cohort study analyzed Medicare Shared Savings Plan Part A and Part B beneficiary claims data paid through January 20, 2019. The research team identified all acute SNF and HH claims within 0 or 1 day after an acute hospital stay for dates of service between December 1, 2017 to November 30, 2018. Outcome variables were defined as cost of care and readmission rates within 30-, 60-, and 90-day increments of time post hospitalization. The team examined whether there is an association with ≥1 previously occurring independent variable(s) including discharge disposition, risk level, and diagnosis.
The Centers for Medicare & Medicaid Services (CMS) Hierarchical Condition Category (HCC) risk-adjustment model was leveraged to compute the risk scores for the analysis. HCC score considers diagnoses and demographic information to modify the monthly capitation rate to reflect the anticipated cost. The CMS-HCC risk model generates risk scores to forecast medical expenses and adjust reimbursement. 10 For this study, the diagnoses and demographics for the population over the 12-month period were entered into the CMS 2016 version 22 SAS program to calculate risk scores.
Descriptive statistics were used to assess demographics and clinical characteristics. Continuous variables are presented with the mean and standard deviation (SD). Differences between groups on continuous variables were measured by Student t test or the Mann-Whitney U test, based on the variables' distribution. Chi-square was performed for categorical variables. All P values were derived from 2-sided tests, and results were considered as statistically significant at P <0.05.
The research team included patient-level covariates in regression analyses, including age, sex, race/ethnicity, and risk score. Factors that reached the level of statistical significance in univariate analysis were included in exploratory multivariate logistic regression using stepwise regression analysis. The main outcome in regression analysis was readmission at 30-days post hospitalization. Data were analyzed using SPSS software version 25 (IBM Corp., Armonk, NY). The study received ProMedica Institutional Review Board approval.
Results
Patient demographics
The analyses included 1151 patients, of whom 734 (64%) were discharged to HH and 417 to SNF levels of care. Total number of index hospitalizations for the patient population included in the analysis was 1297. Patient demographics, including sex, ethnicity, and age, were similar for both groups. For patients discharged to HH, 336 (46%) were male, 658 (90%) were white, 53 (7%) were African American, and average age was 75 years (SD
Risk score
For all patients included in the analysis, the median CMS-HCC risk score was 3.09 (SD
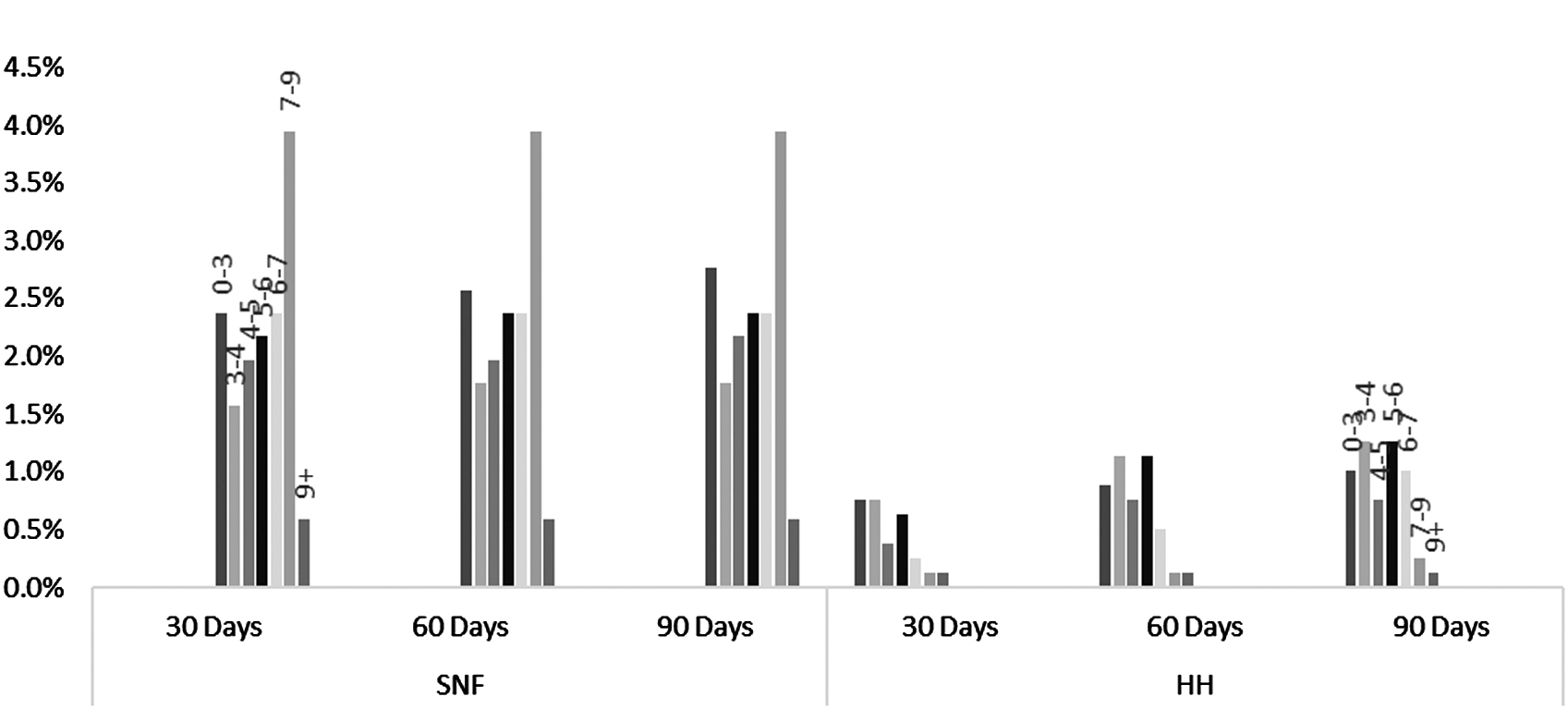
Readmission rates by Centers for Medicare & Medicaid Services Hierarchical Condition Category risk score for HH and SNF at 30, 60, and 90 days. HH, home health; SNF, skilled nursing facility.
Hospital readmissions
The distribution of all the 30-, 60-, and 90-day readmissions for the 2 groups is presented in Figure 2; discharges to SNF are more likely to be readmitted to the hospital within each time frame. The difference between readmission rates for patients in the HH compared to SNF level of care was only statistically significant at the 30-day time frame, chi-square = 63.078, P < 0.000. This is likely related to the smaller numbers of readmissions at 60 and 90 days.
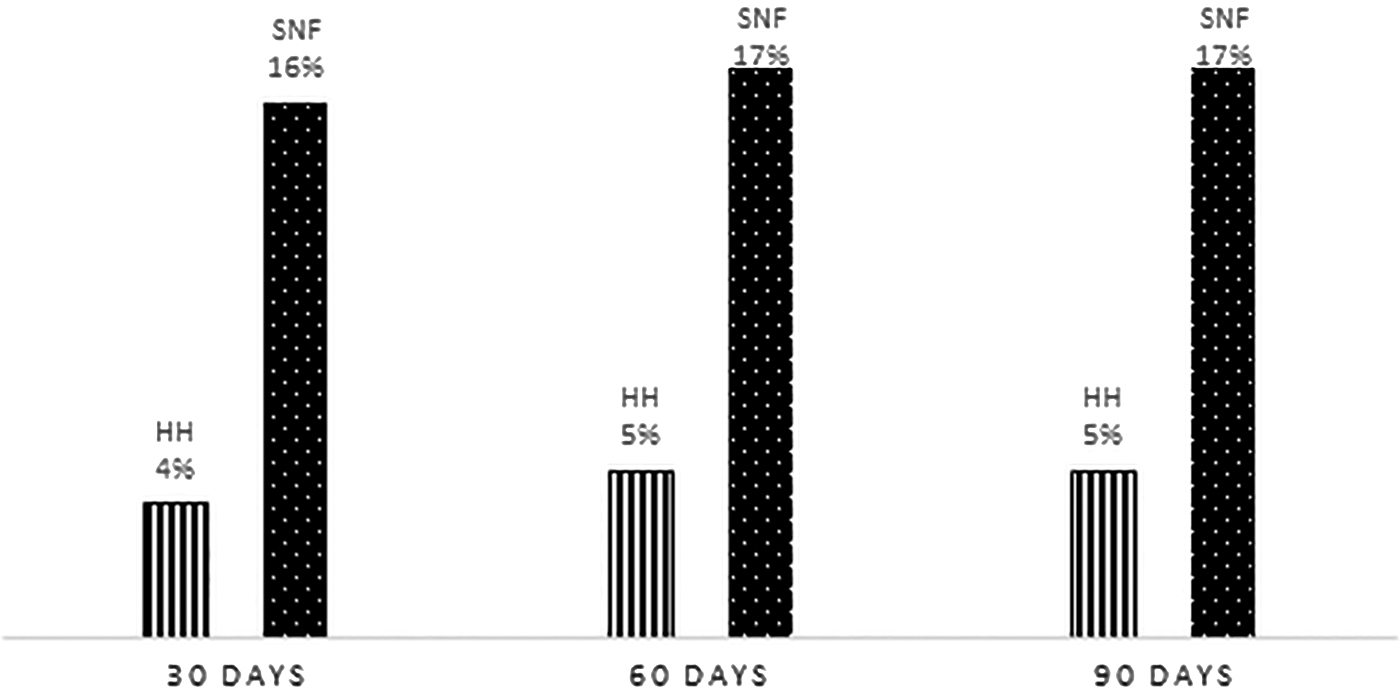
Readmission rates for HH and SNF at 30, 60, and 90 days. HH, home health; SNF, skilled nursing facility.
Regarding sex, males usually have worse outcomes regardless of SNF or HH, as presented in Figure 3, but the differences did not reach statistical significance. In general, patients who use SNF have much higher 30-day readmission rates than those who use HH overall and stratified by sex.
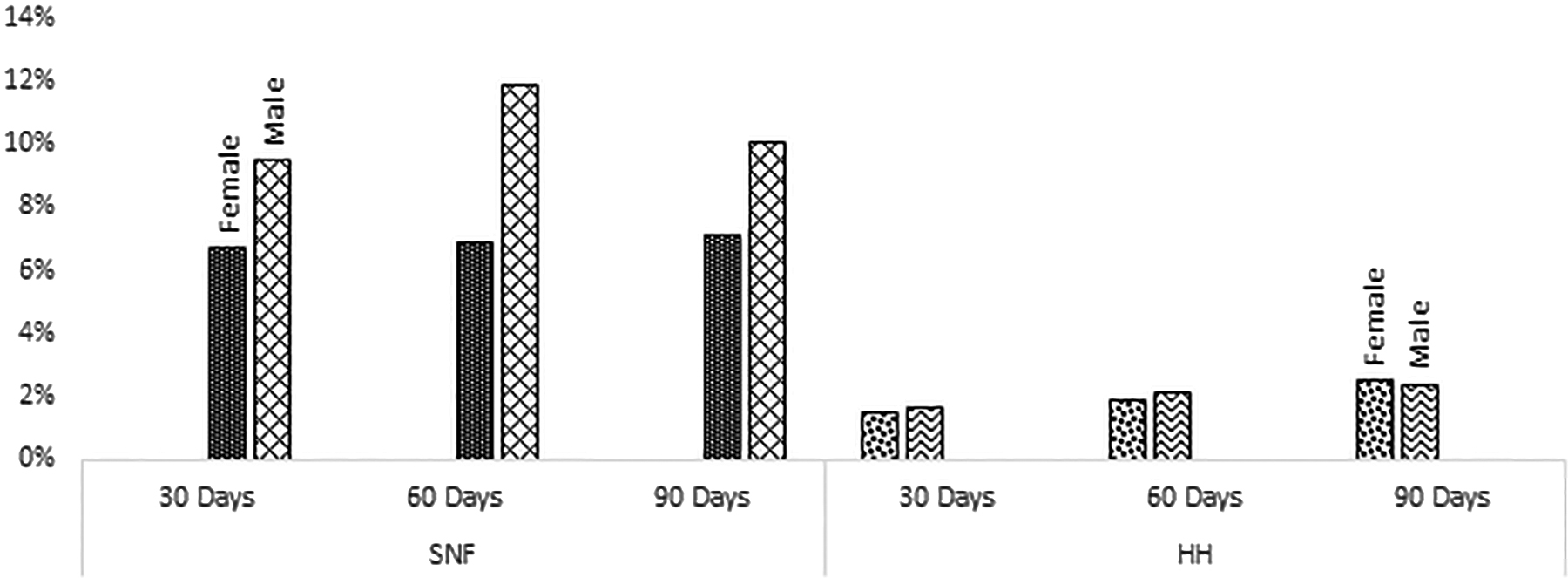
Readmission rates by sex for HH and SNF at 30, 60, and 90 days. HH, home health; SNF, skilled nursing facility.
When reviewing specific diagnoses, including joint replacement, pneumonia, and urinary tract infections, it was noticeable that SNF discharges have higher 30-day, 60-day, and 90-day readmission rates (Figure 4). It should be noted that patients discharged to the SNF level of care had higher risk scores when compared to patients discharged to HH.
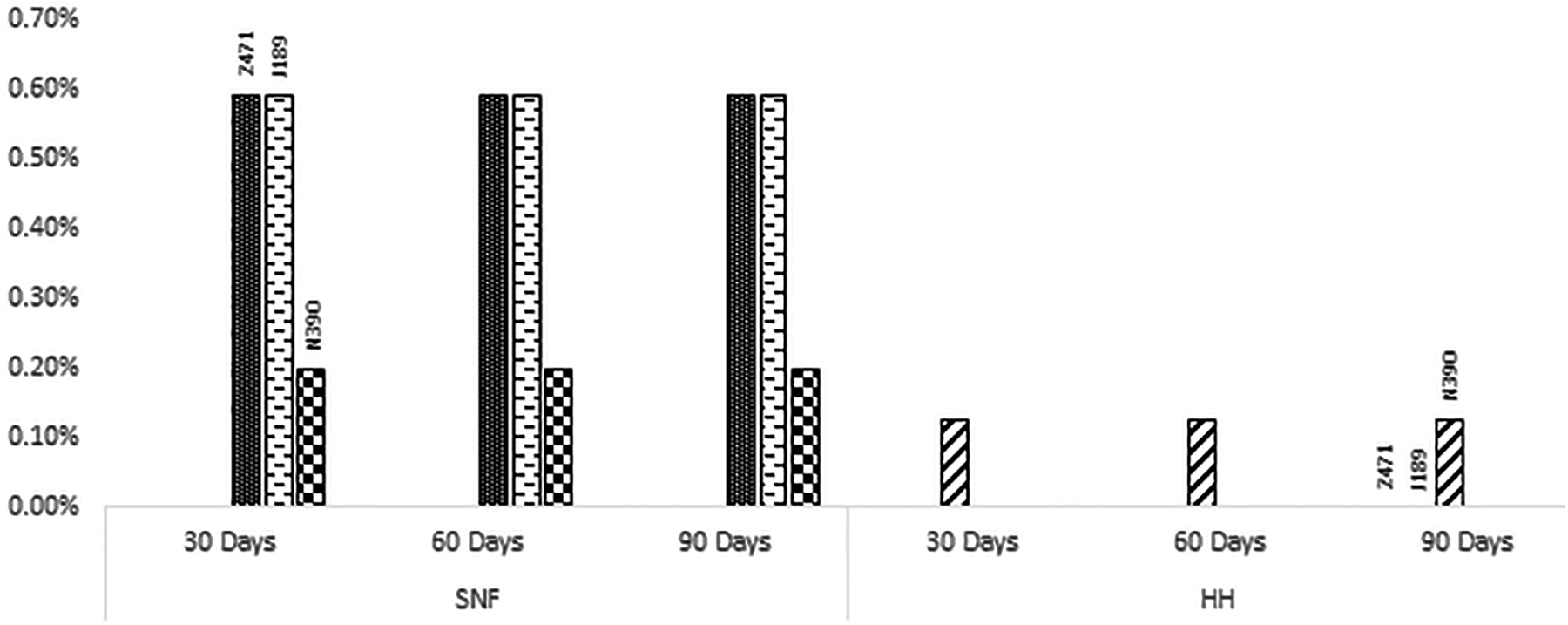
Readmission rates by diagnosis for HH and SNF at 30, 60, and 90 days. HH, home health; SNF, skilled nursing facility.
In multivariate logistic regression analysis, variables associated with increased risk for 30-day readmission were CMS-HCC risk score and discharge setting. Discharges to SNF were almost 5 times more likely to be readmitted to the hospital at 30 days compared to patients discharged to the HH setting (odds ratio [OR] = 4.868 with 95% confidence interval [CI] = 2.972–7.973, P < 0.000). The OR for the risk score was 1.359 with 95% CI = 1.250–1.477, P < 0.000.
Financial impact
When comparing the cost of care for patients discharged to SNF and HH care settings, it was found that SNF stays are more costly than HH. The differences between cost per patient and per discharge are statistically significant between the 2 groups (P < 0.000). The distribution of the average cost per patient discharged to either the HH or SNF setting is presented in Figures 5 and 6 for the 30-, 60-, and 90-day time periods. This confirms the anticipated finding that discharge to the least restrictive next site of care is the less costly disposition.

Average cost per SNF admission, by risk score, at 30, 60, and 90 days.

Average cost per home health admission, by risk score, at 30, 60, and 90 days.
Discussion
ACOs and hospital systems are incentivized to engage in value-based care delivery models and strategies that are supported by evidence. Findings from this study suggest that employing a transitional care planning approach that prioritizes discharging patients to the least restrictive next site of care, shifting patients from SNF disposition to HH as appropriate, is an effective strategy to improve readmission rates and cost of care.
Because there was an overall statistically significant difference between CMS-HCC risk score for the 2 populations, which could be related to provider discharge practices, the analyses were stratified further and it was found that the readmission incidence for patients discharging to HH was lower than SNF for every risk score range and time period studied. The research team confirmed the anticipated outcome that the cost of care is lower for HH discharge disposition, with an $8678 per patient difference between the cost of care for patients discharged to HH and SNF levels of care.
Outcomes from this study are translatable to practice by informing transitional care planning approaches that aim to consider and address the cause of variability in discharge disposition decisions for patients with similar risk scores, with a focus on ensuring that patients receive care in the least restrictive setting.
Transitional care planning encompasses activities and interventions that are completed in preparation for the discharge and transfer of care from the acute care setting. Results of this study suggest implications for enhanced transitional care planning to support the assessment and mitigation of risk for adverse outcomes, within the context of the current health care landscape.
The Transitional Care Model (TCM) provides a theoretical foundation for discharge planning that is conducive to the translation of the best available evidence into practice. 11 The central components of TCM highlight the importance of identifying patients at high risk for adverse outcomes through a comprehensive assessment and engaging them in the development of the plan of care to moderate the risk. 11 Case managers are well positioned to lead the development of the transitional care planning process, facilitating collaboration between the patient, caregivers, and interprofessional team members across the care continuum. The Commission for Case Manager Certification defines case management as a collaborative process of assessing, planning, implementing, coordinating, monitoring, and evaluating options to meet the individual's health and human service needs. 12
In alignment with TCM, the case manager facilitates provision of patient education that is tailored to the individual's health-related goals, with the aim of enhancing the patient's self-care agency. Leveraging technology-driven insights, including predictive analytics and criteria-led discharge tools, can enhance the identification of high-risk patients and assist with defining milestones that pertain to discharge readiness and appropriate next site of care disposition. 13 Further research into the efficacy of these tools in the reduction of variability of referrals to post-acute services is warranted for the continued advancement of transitional care planning models. Appropriate next level of care selection is best coordinated from a least restrictive approach that considers individualized risk factors, goals of care, and health care needs.
Prior research resulted in conclusions and implications for improved transitional care management that are in alignment with suggestions made in the present study. A study comparing inpatient and home-based care for joint replacement patients found no significant difference in satisfaction, pain management, or functional outcomes for either discharge disposition at 3 months or 12 months, despite a significant difference in cost. 14 Variation and subjectivity in provider discharge practices may contribute to increased SNF discharges, as demonstrated by a study that found that 61% of participants discharged to SNF were able to be matched to a patient with similar clinical and demographic attributes in the population who was discharged to HH. 15 Another study involved the analysis of readmission rates for patients after a spinal fusion following the reduction of discharges to SNF from 49% to 34%, resulting in no change to readmission rates. 16
Results from the present study and prior research suggest that there is improved overall health and better financial outcomes when patients discharge to HH compared to the SNF level of care. This establishes an evidence base with compelling implications for an ACO to adopt value-based strategies aimed at avoiding variation in transitional care management practices and the promotion of hospital discharge approaches that give precedence to the least restrictive next site of care.
There are some methodological limitations to this analysis. This is a retrospective analysis that involved adjustment for certain variables, including demographics and risk score, but no adjustment for other possible confounders as factors related to the initial patient hospitalization. The analysis did not consider other outcomes such as mortality, quality of life, patient satisfaction, or functional status post discharge, which merit further investigation.
Another limitation of the study is that the CMS-HCC Risk Model does not consider social determinants of health (SDOH) and associated barriers to safe and successful transitions of care when assigning risk scores. A study by Joynt Maddox et al found that accounting for SDOH can have an economic impact on safety net hospitals. 17 Based on retrospective analyses, under the Medicare Hospital Readmissions Reduction Program safety net hospitals had higher readmission ratios (acute myocardial infarction, 1.020 vs 0.986 for the most affluent hospitals; pneumonia, 1.031 vs 0.984; and congestive heart failure, 1.037 vs 0.977). After adjusting for certain SDOH factors, the penalties declined for more than 50% of the hospitals, and there was a $17 million reduction in penalties for safety net hospitals. 17 Further research into the impact that the independent variables housing, socioeconomic status, and hunger have on readmission rates and total cost of care in the post-acute period is warranted.
Conclusions
Alternative payment models and health care reform drive health systems to align with the value-based aims of quality and safety agendas, considering implications for adopting strategies that promote positive patient outcomes and decreased cost of care. Incentives for health systems include increased revenue potential through Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores and ACO shared savings and the avoidance of cost through readmission and other financial penalties. Implications for further research include the development and implementation of standardized criteria or pathways for specific diagnoses or patient populations to guide discharge disposition decisions and reduce inconsistency, and to further examine the impact that SDOH variables have on patient outcomes and cost of care following a hospitalization.
This study provides strong evidence that discharging to the least restrictive next site of care through enhanced transitional care planning is a viable strategy for hospitals and ACOs in the value-based health care setting.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.