
Abstract
Understanding the health care system's ability to move patients through the hepatitis C virus (HCV) care cascade from screening to treatment is essential for HCV elimination. This retrospective study describes real-world HCV screening rates and care cascade steps to identify gaps in care for patients with HCV in the United States. Eligible patients were aged ≥18 years as of the measurement year (calendar year between January 1, 2010—December 31, 2016) and were commercial and Medicare Advantage with Part D members in the Optum Research database with continuous health plan enrollment 5 years prior to and during the measurement year. Incident and prevalent screening rates were calculated for each measurement year. Care cascade steps were analyzed via Kaplan-Meier analysis and logistic regression among patients with a positive HCV ribonucleic acid test. Cohorts were selected based on birth year (pre-1945 birth cohort, 1945–1965 birth cohort, post-1965 birth cohort). Among the 1945–1965 birth cohort, incident and prevalent screening rates increased from 1.6% to 4.7% and 10% to 18%, respectively, from 2010 to 2016. The proportion of patients attaining each independent cascade step within 1 year of screening increased significantly over time for genotype testing (P = 0.0283) and receipt of treatment (P < 0.0001). Median time from screening to treatment decreased from 1627 days (95% CI 1335–1871) in 2010 to 282 days (95% CI 223–498) in 2015. HCV screening and completion of the care cascade has improved for certain patient populations; however, gaps remain, highlighting the urgent need to address barriers to meeting HCV elimination goals.
Background
An estimated 4.29
HCV treatment is just one of many steps in the care cascade and HCV elimination will require addressing key steps upstream of treatment, such as screening, diagnosis, and linkage to care. Previous studies published before the introduction of DAAs have estimated that only 5% −13% of patients with HCV complete the care cascade and ultimately achieve sustained virologic response (SVR). 3 –5
In 2012 and 2013, the Centers for Disease Control and Prevention (CDC) and the US Preventive Services Task Force (USPSTF) issued new recommendations for a 1-time screening for HCV infection in all adults born between 1945 and 1965, in addition to screening high-risk patients (eg, patients with injection drug use, long-term hemodialysis, incarceration, blood transfusion prior to 1992). 6,7 Patients born between 1945 and 1965 have a 5-fold higher HCV prevalence rate and the highest risk of developing HCV-related complications, accounting for 75% of all HCV infections in the United States and 73% of HCV-related mortality. 6,8
More recent estimates of the care cascade would aid policy makers and other health care stakeholders in identifying gaps in care and monitoring progress toward HCV elimination in the context of the updated screening recommendations and the anticipated arrival of DAAs. This study used observational data from a large real-world US population to estimate rates of screening and other steps in the HCV care cascade over time.
Methods
Study design and data source
This was a retrospective analysis of commercial and Medicare Advantage with Part D (MAPD) enrollees conducted from January 1, 2005, through December 31, 2016 (study period) using administrative claims with linked laboratory data from the Optum Research Database (ORD), a proprietary US health insurance database that contains fully de-identified medical, pharmacy, and enrollment information from 1993 to the present, covering 60 million lives. Medical claims included diagnosis and procedure codes from the 9th and 10th revisions of the International Classification of Diseases, Clinical Modification (ICD-9-CM and ICD-10-CM); Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) codes; and other information. Outpatient pharmacy claims included National Drug Codes for dispensed medications, quantity dispensed, dose, dosage form, and number of days' supply. Institutional review board approval or waiver of authorization was not required for this study because no identifiable protected health information was extracted or accessed.
Study population
Each calendar year (between January 1 and December 31) during the period from January 1, 2010, through December 31, 2016 (screening period) was considered a measurement year. Inclusion and exclusion criteria for study eligibility were assessed independently each measurement year. For inclusion in a given measurement year, patients were required to be ≥18 years of age as of the measurement year and to have continuous health plan enrollment with medical and pharmacy benefits for 5 years prior to January 1 of the measurement year (baseline period) and during the measurement year.
Patients with evidence of HCV Ab screening (CPT codes 80074, 86803, 86804; HCPCS code G0472), HCV ribonucleic acid (RNA) or genotype testing (CPT codes 87520, 87521, 87522, 87902; HCPCS code 3265F), HCV diagnosis (ICD-9-CM codes: V02.62, 070.41, 070.44, 070.51, 070.54, 070.70, 070.71; ICD-10-CM codes: B1710, B1711, B182, B1920, B1921, Z2252), or HCV treatment (pharmacy claim for interferon and ribavirin, telaprevir, boceprevir, sofosbuvir, simeprevir, ledipasvir/sofosbuvir, ombitasvir/paritaprevir/ritonavir/dasabuvir, elbasavir/grazoprevir, daclatasvir, ombitasvir/paritaprevir/ritonavir, or sofosbuvir/velpatasvir) during the baseline period were excluded from the measurement year.
To be eligible for the care cascade analysis during a given measurement year, patients also were required to have evidence of an HCV Ab or RNA test during the measurement year (earliest date set as index date) and at least 1 year of continuous health plan enrollment following the date of the test. Evidence of a positive HCV RNA test between index date and through the end of the follow-up period also was required. Follow-up ended at the earliest of health plan disenrollment or September 30, 2016 (date chosen as a result of claims adjudication lag at the time data were initially pulled).
Cohorts
Cohorts were created based on birth year and included the pre-1945 birth cohort (patients born prior to January 1, 1945); the 1945–1965 birth cohort (patients born between January 1, 1945 and December 31, 1965); and the post-1965 birth cohort (patients born after December 31, 1965).
Study measures
Patient characteristics
Demographics and the Charlson comorbidity index among screened patients were measured during the baseline period and included patient age, sex, race/ethnicity, geographic density (rural or urban), geographic region, and insurance type (commercial or MAPD).
Screening
Prevalent screening rates
Prevalent screening rates were calculated for each calendar year from 2010 to 2016 by dividing the year-specific prevalence numerator by the year-specific prevalence denominator. The year-specific prevalence numerator was the number of patients screened during that year plus the number of patients who had any screening, treatment, or diagnosis during the 5-year baseline period. The year-specific prevalence denominator was the number of patients eligible for screening that year plus the number of patients who had any screening, treatment, or diagnosis during the 5-year baseline period.
Incident screening rates
Incident HCV screening rates were calculated for each calendar year from 2010 to 2016 by dividing the number of patients with an HCV Ab or RNA test performed during the measurement year by all patients meeting the inclusion and exclusion criteria for the measurement year. Patients screened were removed from study eligibility in subsequent measurement years.
Care cascade
Steps in the care cascade were measured with the following variables captured during the follow-up period: a new HCV diagnosis in any position on the medical claim (not including claims on index date), at least 1 visit to a HCV specialist (hepatologist, gastroenterologist, infectious disease specialist, or other HCV-related specialties) within 1 year, evidence of genotype testing, and any HCV treatment. Additionally, the time from screening to each of these steps was recorded. Steps in the HCV care cascade were analyzed independently and inclusion in subsequent steps was not based on completion of those prior.
Statistical analyses
Patient characteristics were analyzed descriptively and stratified by measurement year. Incident screening rates were reported by measurement year and stratified by birth cohort, insurance type, sex, and race. The proportion of patients with any screening in the 5-year baseline period or the measurement year also was calculated (prevalent screening rate). Kaplan-Meier analyses were used to describe each step of the care cascade. Logistic regression with linear measurement year was used to test for a time trend in the proportion of patients reaching each cascade step within 1 year.
Results
Baseline demographic characteristics
Patient sample selection is shown in Table 1. Among patients with evidence of HCV Ab screening or an RNA test during any measurement year, the majority were female, white, commercially insured, and between the ages of 30 and 59 years (Table 2).
Patient Selection
For the 2015 measurement year, based on the available data at the time of the data extraction, only screened patients between January 1, 2015, and September 30, 2015 (n = 34,188) were included in the care cascade analysis in order to allow for a full 1-year follow-up.
HCV, hepatitis C virus.
Patient Demographics by Measurement Year of Screened Patients
SD, standard deviation.
Screening
The overall annual incident HCV screening rate increased 1.4 percentage points between 2010 and 2016. In the 1945–1965 birth cohort, annual incident HCV screening rates increased 3.1 percentage points between 2010 and 2016, with the largest increase occurring after 2012 (2.2 percentage points between 2013 and 2016) (Figure 1). Incident screening rates in patients with MAPD coverage were higher than rates among commercially-insured patients in 6 of the 7 measurement years and increased 4.1 percentage points between 2010 and 2016 (Figure 2A). Annual incident screening rates were similar among males and females (Figure 2B) and appeared consistently higher in Asians, African Americans, and Hispanics relative to whites over the 7-year study period (Supplementary Fig S1).
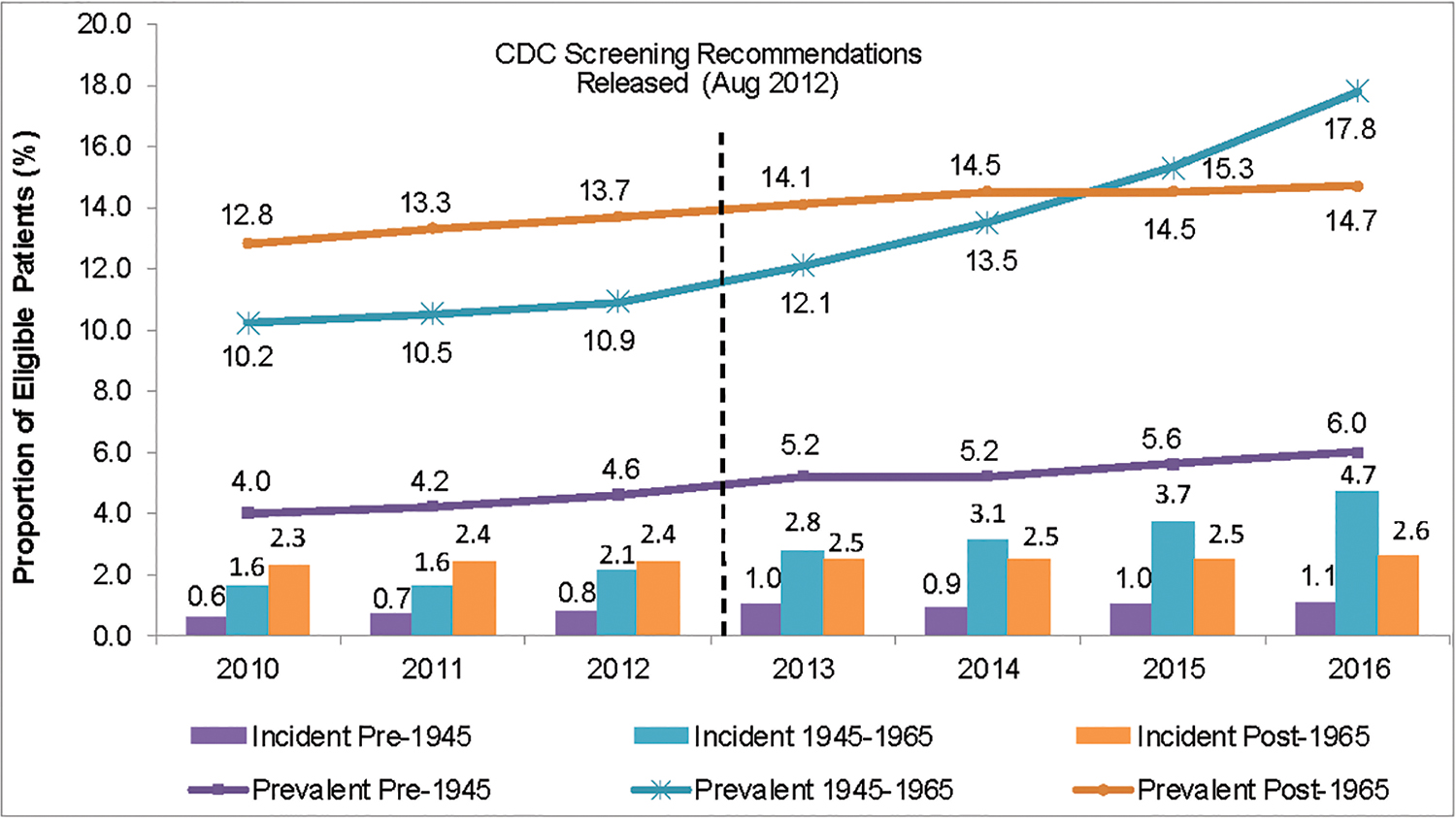
Annual incident and prevalent screening rates over time by birth cohort. CDC, Centers for Disease Control and Prevention. Color images are available online.

Incident and prevalent screening rates over time among patients in the 1945–1965 birth cohort stratified by demographic characteristics.
In the 1945–1965 birth cohort, prevalent screening rates increased only slightly (.7 percentage points) from 2010 to 2012, but increased 6.9 percentage points from 2012 to 2016, following the CDC recommendations for screening in this cohort (Figure 1). Patients in the pre-1945 birth cohort had the lowest prevalent screening rates. Younger patients in the post-1965 birth cohort had higher prevalent screening rates that remained relatively constant over the 7-year time period (Figure 1).
Care cascade
Among the 2724 patients with available HCV RNA test results during the follow-up period, 832 patients (30.5%) had a positive HCV RNA test and were included in the care cascade analysis. Among these patients, 39% were female and the majority were white (66%), lived in the South (69%), and had commercial insurance (86%) (Supplementary Table 1). The proportion of patients who attained each cascade step within 1 year of screening increased for genotype testing and HCV treatment over the 6-year period (Figure 3).
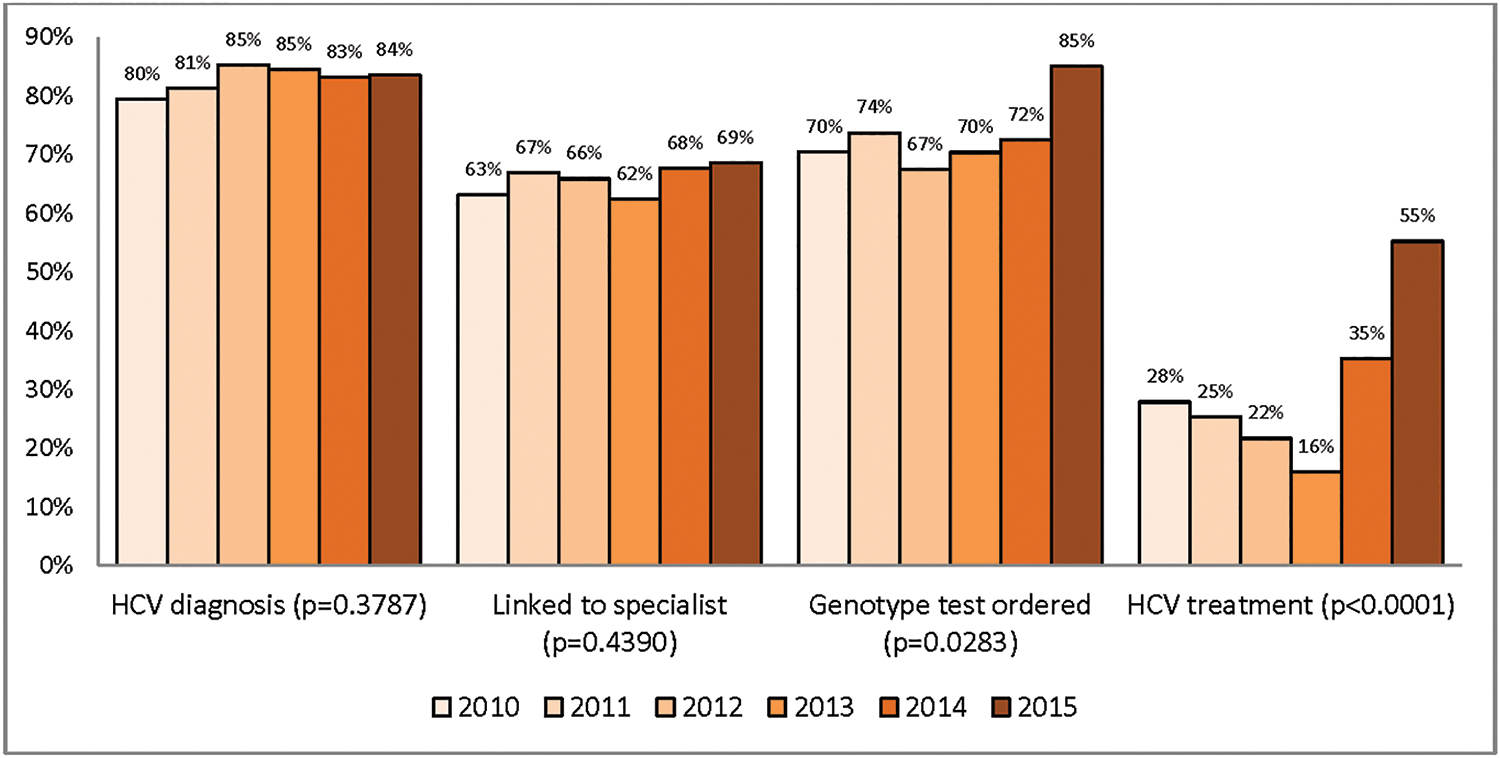
Cumulative proportion of patients reaching each cascade step within 1 year of screening. Note: These results were among patients with a positive HCV RNA test. P value based on logistic regression with linear measurement year. HCV, hepatitis C virus; RNA, ribonucleic acid. Color images are available online.
The proportion of patients who received an HCV diagnosis and/or were linked to specialist care were similar each year over the 6-year follow-up period. In contrast, the proportion of patients who received HCV genotype testing increased significantly from 70.5% in 2010 to 85.1% in 2015 (p = 0.0283) and the proportion of patients receiving HCV treatment increased significantly from 27.9% in 2010 to 55.2% in 2015 (P < 0.0001). The increase in the proportion of patients treated was seen across insurance plan types (commercial, P = 0.0012; MAPD, P < 0.0001) and sex (female, P = 0.0439; male, P < 0.0001) (data not shown).
There was a large decrease in median time from screening to HCV treatment from 1627 days in 2010 to 282 days in 2015 (Figure 4A). Between 2010 and 2015, the median time from screening to HCV diagnosis ranged from 31 to 63 days, linkage to a specialist within 1 year ranged from a median of 78 to 122 days, and receipt of a HCV genotype test ranged from 44 to 71 days (Figure 4B).
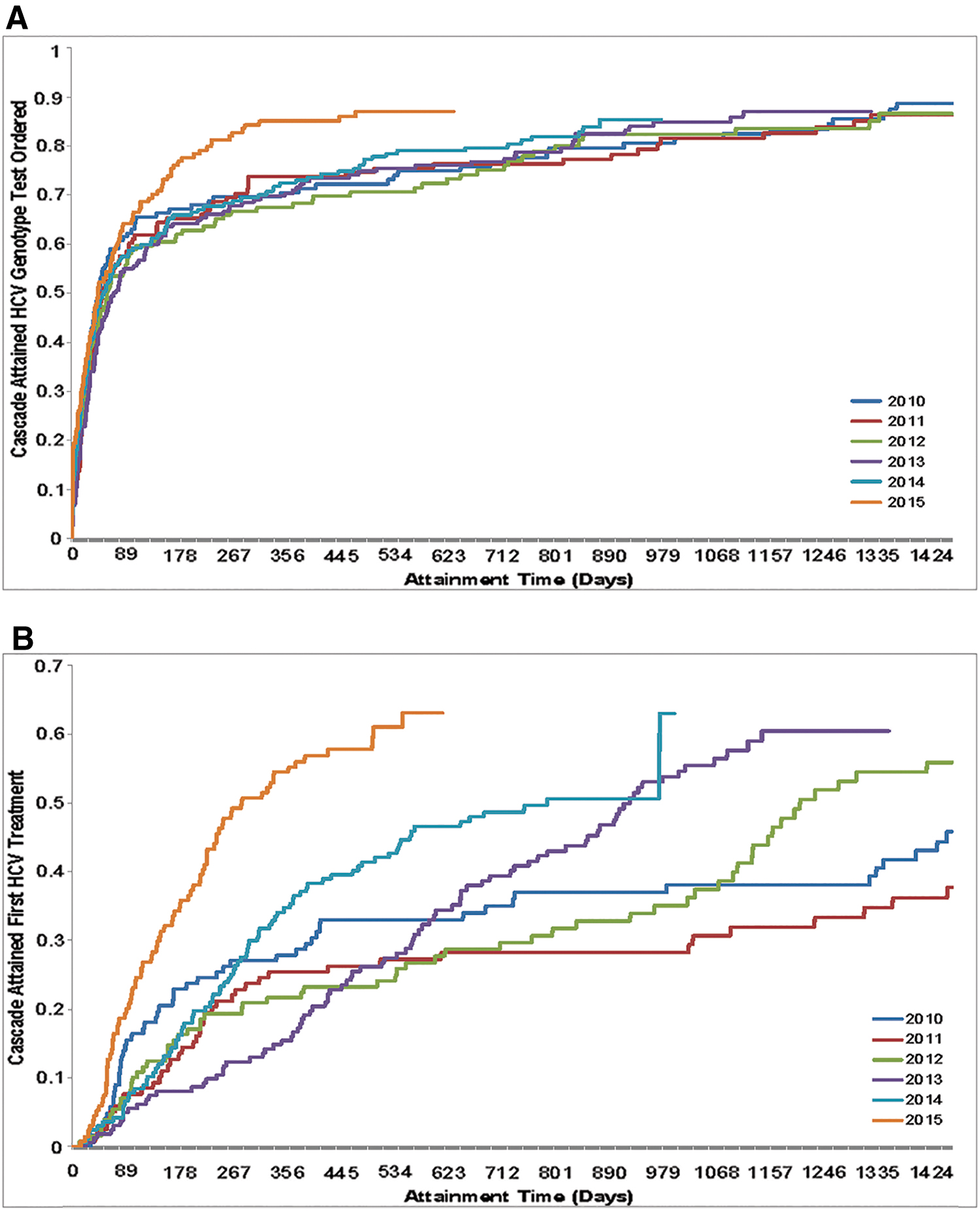
Proportion of patients reaching HCV care cascade steps: genotype testing and treatment receipt among patients with positive RNA tests
Discussion
Continuing to understand and identify gaps in the HCV care continuum is important for the development of programs to improve screening, diagnosis, linkage to care, and HCV treatment. This study provides a more recent understanding of HCV screening rates in a large, geographically diverse US insured population and progress made in the cascade of care provided to these patients. This study found that although screening rates have increased over time, particularly in the 1945–1965 birth cohort, rates remain lower than desired with prevalent screening rates of less than 20% in 2016.
Patients in the 1945–1965 birth cohort experienced the largest increase in incident HCV screening rates (increasing 194% from 2010 to 2016), with the greatest increase following the CDC's recommendation in August 2012 for 1-time HCV screening in this birth cohort. The results for the 1945–1965 birth cohort are consistent with trends seen in previous studies based on data between 2011 and 2014. 9,10 In contrast, rates in the pre-1945 birth cohort and the post-1965 birth cohort remained relatively unchanged following publication of the CDC guidelines in 2012, as they continued with risk-based screening only. Despite the recent increases, national HCV screening rates among the 1945–1965 birth cohort remain low with only 17.8% of patients in this cohort screened by 2016. Furthermore, although this descriptive study did show that increases in incident HCV screening rates were higher among patients with Medicare relative to commercial health plans, and Asians, African Americans, and Hispanics relative to whites, additional research is needed to determine if these trends still hold after controlling for potential confounders using multivariate analyses.
Although low screening rates are a major barrier, this study also found that movement through other steps in the care cascade has not changed dramatically over time among HCV RNA positive patients. Linkage to care has not improved for patients with HCV; however, treatment rates have improved, increasing from 27.9% in 2010 to 55.2% in 2015. Improvement in treatment rates during the study period may have been exaggerated by warehousing—intentional treatment delay among patients diagnosed in earlier years in expectation of new and better future treatments. This is further supported by fact that the median time to treatment decreased from 1627 days in 2010 to 282 days in 2015. Despite improvements in treatment rates, it remains the biggest gap in the care cascade with only 55% of HCV RNA positive patients achieving this step in 2015.
This analysis showed that gaps in screening and access to care exist even with the rapid advancements in treatment and care between 2010 and 2016. Since 2016, the cost of HCV medications has decreased, which likely increased treatment rates. It is thought that most patients who remain untreated today are those who are harder to reach, such as intravenous drug users, the homeless, or the incarcerated. There are still at-risk patients who have not been screened or treated and more work needs to be done to identify those gaps, broadly or among certain at-risk populations.
As the incidence of HCV increases, especially among the younger population affected by the opioid epidemic, it is possible that patients are more routinely treated and managed for HCV by their primary care providers, 11,12 which was not included in this study's definition of linkage to care. This underestimation of true linkage may be why a large increase in treatment occurred in the later years, but that same increase in linkage was not seen.
A key provision of the Affordable Care Act (ACA) is the requirement that private insurance plans cover recommended preventive services without patient cost sharing. Coverage for screening for HCV in adults at high risk for HCV infection and 1-time screening for HCV infection in adults born between 1945 and 1965 are recommended with a grade B by the USPSTF. 7 This analysis shows that even with this coverage, additional work is needed to increase the number of patients screened.
Numerous pilot studies have shown promising results in increasing screening rates, resulting in increases of 36% −1482% in HCV screening among patients in the 1945–1965 birth cohort. 13 –20 Most of these studies centered around the use of electronic health record (EHR) best practice alert prompts to remind primary care providers to screen patients in the 1945–1965 birth cohort seen in the clinic who lacked prior HCV screening or diagnosis, and with linkage to specialist care among those who tested positive. Maclean et al found that implementing EHR prompts for primary care patients increased HCV screening rates by 25 percentage points. 20 Similarly, Konerman et al reported that anti-HCV testing was ordered in 47% of eligible patients after implementation of an EHR prompt compared to only 4.6% prior to the prompt. 13 Emergency room-based screening programs have been developed to meet the needs of patients who have poor access to preventive care services but have higher prevalence of disease. Anderson et al found that among HCV antibody-reactive patients screened in the emergency room, 82% completed viral load testing. Among patients who tested RNA positive, 52% had follow-up appointments arranged with 61% actually attending their appointment. Twenty-five percent of patients who attended their appointment began treatment, with 79% of them achieving SVR. 21 Although these pilot studies have found great success, the screening gaps that remain may disproportionately affect more vulnerable patients, including those who lack health insurance/access to care, use illicit drugs, are incarcerated, or are homeless. Unique targeting of patients, such as those seeking emergency care, may be successful in getting these patients into the system.
Limitations
The intrinsic limitations of claims data should be considered when interpreting the results of this study. Patients' medical history and screening information prior to the 5-year baseline period was unobserved; thus prevalent screening rates may be underestimated. Additionally, the research team was unable to capture behavioral risk factors to accurately assess adherence to CDC recommendations for risk-based screening.
In the care cascade analysis, this study only measured linkage to a specialist, not primary care provider-based or internist-based linkage. As a result, true linkage may be underestimated. Fibrosis staging is an important step in the care cascade for patients with HCV to identify cirrhosis and guide treatment strategy; however, this study did not assess the percentage of patients who received fibrosis staging because of claims data limitations. Because of the coverage of the health plan, almost half of study patients resided in the South; however, racial/ethnic data of the sample population closely followed that of the 2012 census data collected for the United States by the US Census Bureau. Lastly, ≥6 years of continuous health plan enrollment was required to identify patients with a likely history of screening or diagnosis; thus patients included in this study may not be generalizable to patients who more frequently change health plans or patients outside a stable managed care setting. Although screening and linkage to care among the uninsured, homeless, or incarcerated patient populations were not examined in this study, it can be expected that the need for better screening and linkage to care are even greater in these vulnerable populations.
Conclusions
Annual HCV screening rates trended upward in the United States in more recent study years; however, they remained low in the 1945–1965 birth cohort despite age-based HCV screening recommendations from the CDC in 2012 and the availability of effective HCV treatment options. This highlights the need to implement practical methods, such as use of EHR alert prompts to enhance screening in this population. Although reduced time to treatment was an encouraging trend, only half of patients diagnosed with HCV were found to be treated within 1 year of screening and more programs need to be developed to increase access to treatments. Study findings suggest that in order to achieve HCV elimination in the United States, improvements are needed in care, particularly in ensuring timely diagnoses and treatment. Future studies should be replicated and repeated regularly in the United States and elsewhere to assess progress toward global HCV elimination.
Footnotes
Author Disclosure Statement
Drs. Lee and Ting were employees of Gilead Sciences, Inc. at the time the study was conducted. Dr. Lee is currently employed by Optum. Drs. Bancroft and Tran, and Ms Buikema were employees of Optum at the time this study was conducted and were funded by Gilead Sciences, Inc. to conduct the study. Dr. Tran is currently employed by United Healthcare. Dr. Wong was a consultant for Gilead Sciences, Inc., has served on advisory boards and speakers bureaus for Gilead Sciences, Inc., and participated in research grants for Gilead Sciences, Inc. and AbbVie, Inc. Dr. Terrault has received institutional grant support from Gilead Sciences, Inc. No funding was received for the medical writing of this manuscript.
Funding Information
This study was funded by Gilead Sciences, Inc. Medical writing assistance was provided by Deja Scott-Shemon, MPH, an employee of Optum. The authors would like to thank Yiyu Fang, Bret Gitar, and Jeff McPheeters (all of Optum) for data programming, verification, and cleaning, and Susan Peckous, MA (Optum) for project management.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.