
Abstract
The Affordable Care Act became law 10 years ago, and it has been just over 10 years since academic institutions began using the term “Population Health” in department and college titles. Sixteen years ago, Kindig and Stoddart published the often-cited “What Is Population Health?” 1 that differentiates that term from public health: “Population Health: the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”
To the authors' credit, critiques and discussion of their proposed definition “that may lead to some consensus on this emerging concept” were welcomed. The concept continues to develop as US health care responds to new imperatives, and the debate continues about the definition of population health. 2,3 Is it just semantics?
As science discovered effective approaches to confront disease epidemics, the field of public health advanced in its work with populations. It is no surprise that public health leaders and practitioners would consider population health part of their discipline. Today, public health experts and health care practitioners address challenges across a continuum between public and population health. Figure 1 illustrates a spectrum of fluid issues that we address. It is a schematic that can promote discussion about where those issues lie across a continuum, how they are shifting, and how and by whom they could be most effectively addressed.
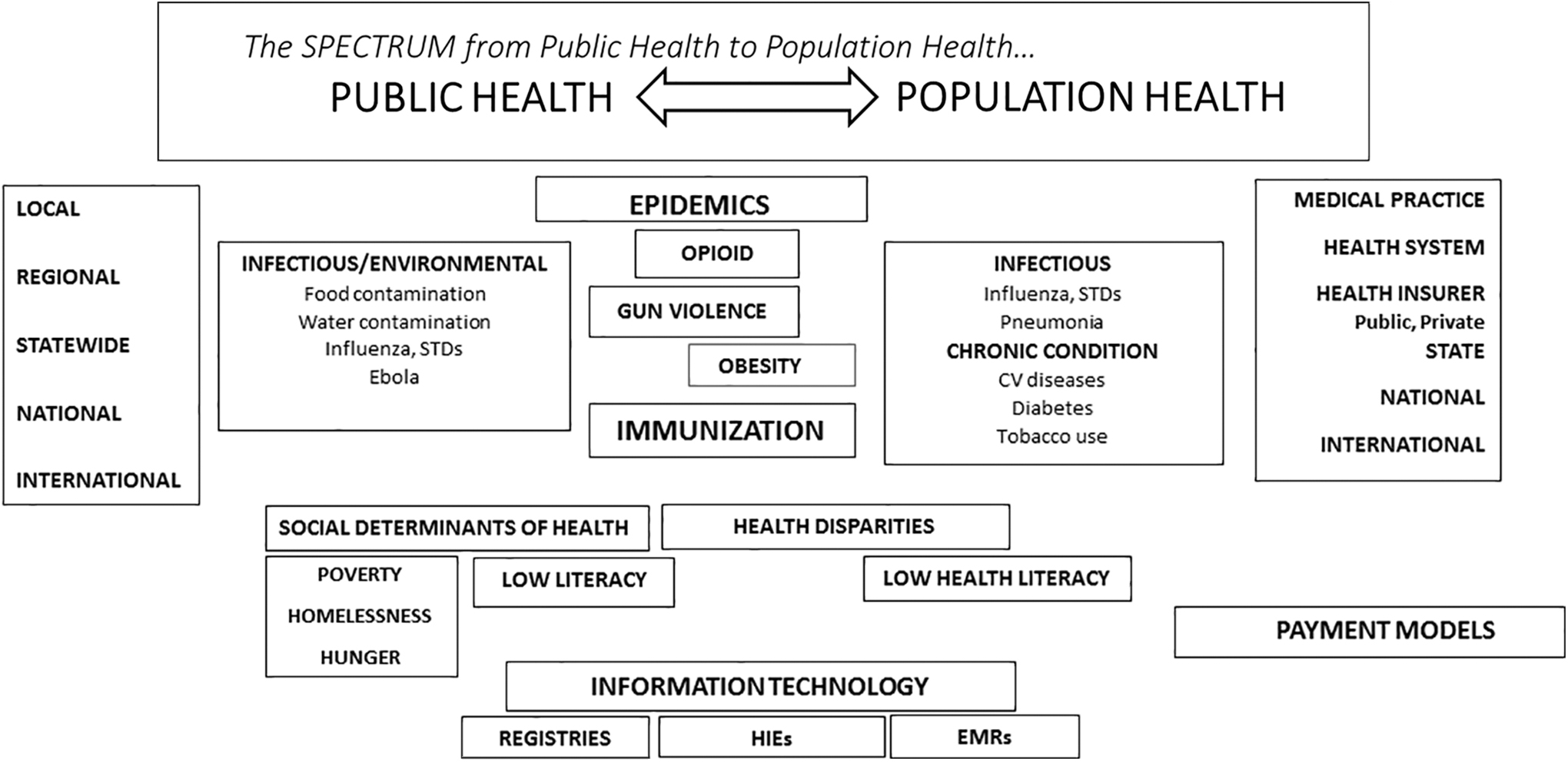
The spectrum from public health to population health. CV, cardiovascular; EMRs, electronic medical records; HIEs, Health Information Exchanges; STDs, sexually transmitted diseases.
History helps to better understand this ongoing evolution. The US health care industry and public health institutions have grown, largely independent of each other, over 2 centuries. Medical discoveries have been applied to public health initiatives, while health care workers have assisted public health organizations to address epidemics, but the disciplines had remained largely distinct.
American history captures the story of a new nation, built with a romantic reverence for rugged individualism and the “self-made man,” driving economic and social policy. This contrasts with a European ethos that promoted social and governmental responsibility for the community. Tension between these fundamentally opposed philosophies continues to be expressed in politicization of health care policy and beliefs.
The US health care system, in its fee-for-service heyday, rapidly developed advances in care, and profits. The United States became widely recognized as leading the world in technological innovation. Investment grew. The 5% of our national wealth (gross domestic product [GDP]) devoted to health care in 1960 more than tripled over the ensuing 60 years to almost 18% 4 and is projected to reach 20% in 2024. During the same time, political and social concerns in support of protecting vulnerable segments of our population resulted in the passage of Medicare in 1965 for citizens ages 65 and older, and was expanded to protect those with disability and end-stage renal disease in 1972.
Continued support for our nation's ever-growing allotment of percent GDP to health care might be bolstered if the return on investment were a healthier, more productive population. However, in the face of an explosion of health care costs and advances, poor population health outcomes have become increasingly evident over the past decade. 5 Poor outcomes do not support the high cost. Additional recognition that our massive investment in health care contributes toward only 10%-20% of a population's health 6 is dismaying.
Seminal work by, among others, Brenner in Camden, New Jersey (given wider attention through Gawande's article “The Hot Spotters” 7 ) contributed to rising health care system awareness of the high-need/high-cost patient and the profound impact that social determinants of health have on our health care costs. And Brenner illustrated that attention to the historically nonmedical issues that drive social disparities results in more effective and efficient medical care, one patient at a time. To address social determinants of health, realignment of some investment from medical to social focus appears inevitable.
The difference in resource allotment between the United States and other industrialized nations is evident in Organisation for Economic Co-operation and Development comparisons of social and medical spending as percent of GDP. The United States is an outlier, spending much more on health care and much less on social care compared to other industrialized nations. 8 A recent study published in JAMA found that only 15.6% of physicians reported screening for 5 social determinant of health factors: food insecurity, housing instability, utility needs, transportation needs, and interpersonal violence. 9
“Where will the money come from?” becomes the critical question with the need for greater social investment in the United States. Progress in reducing error to improve quality, and better medical tools, drugs, and protocols will drive better outcomes, but cannot promise enough reduction in total expenditure to fund unmet social needs. In fact, innovation could drive escalating costs. Will root causes of poor health be addressed?
As Nash has lectured, “Shut off the faucet and stop mopping the floor!” 10 From that faucet flow those social determinants of health: poverty, homelessness, hunger, lack of education, and others that thwart the potential success of our best medical innovations. It is incumbent on the US health care industry to move upstream, with community and public health partners, to address not just the prevention and treatment of disease, but to promote a culture of wellness.
Nearly one third of health care expenditure is waste 11 ; savings from waste reduction could fund efforts to improve social determinants of health. Waste includes excessive administrative overhead of an industry burdened with duplicative processes that drive even greater investments in technology and staffing. Unnecessary testing, and care that is not evidence based, afford additional cost-saving opportunities that reduce waste.
The Centers for Medicare & Medicaid Services, the nation's largest health insurer, has been leading efforts away from a purely fee-for-service volume-based enterprise for a decade. With a budget representing 4.8% of GDP (2018) the change has been challenging and disruptive, and some say not fast enough. A strategy of shifting risk of cost from payers to those who order the goods (providers [physicians and hospitals]) opens the door to innovative approaches to address total costs of care (and, by necessity, social determinants of health). And private payers are following similar strategies. It will become increasingly painful for proponents of the status quo to weather these changes.
Against this background, the answer to “What is population health?” becomes clearer. Beyond understanding the health outcomes of a group of individuals, including the distribution of such outcomes within the group, an evolving toolbox of knowledge and skills becomes critical to successful strategies for change. Population health is the study and implementation of these tools. Strategies to confront social determinants of health, and the reengineering of health care systems to achieve transformations, are at the root of population health research, teaching, and practice.
Population health experts along with public health experts can work together with private and public health care leaders, communities, and government representatives under the umbrella of population health. And just as health care is transforming, so will population health.
Footnotes
Acknowledgment
I would like to acknowledge Drs. David Nash and Billy Oglesby, colleagues of mine at the Jefferson College of Population Health, for their thought contributions to this article.
Author Disclosure Statement
The author declares that there are no conflicts of interest.
Funding Information
No funding was received for this article.