
Abstract

The role of serological antibody testing to aid in the management of the COVID-19 pandemic has garnered considerable enthusiasm in the lay media and policy spheres. There is intuitive appeal in using Immunoglobin G (IgG) testing to better understand levels of immunity in individuals and populations as we develop plans for resuming economic activity. Some have explored the role of mass antibody testing to create a “passport” to guide safe reentry into the workforce. Others have recommended antibody testing in much narrower contexts, such as for high-risk individuals with pulmonary or other chronic diseases, a prerequisite for vaccine delivery (in order to use limited vaccine supply only on those who would benefit), or as a mechanism to identify those who could donate convalescent plasma.
Some key questions about the utility of antibody testing remain. There is uncertainty about the levels of antibody needed to provide immunity, and how long that immunity lasts. There also is uncertainty regarding the ability of an individual to exhibit IgG antibodies and continue to shed the virus, allowing for continued transmission. 1 Nonetheless, several studies have demonstrated the emergence of neutralizing antibodies concurrent with the rise in antiviral antibody titers and reductions in viral load, and these responses appear to persist for at least some months. 2,3 For the purposes of this article, as the science continues to accumulate, we are assuming that the tests do predict protection from subsequent infection from the virus – this must be confirmed to make informed decisions about the use of antibody testing. As we await further evidence about the extent and durability of immunity, we are proposing a solution for broader consideration so that a testing strategy is available if antibodies prove to be sufficiently protective. We cannot yet comment on the need for subsequent antibody testing in those who test positive.
Today, there are no clear recommendations from federal agencies about when to use antibody tests to inform Return to Workplace (RTW) scenarios. Experts note the many variables that should be considered when deciding whether and when to use the tests. Early availability of more than 120 different test models in the United States, with widely varying test characteristics and validation, contributed to the confusion. This complexity is compounded by varying underlying risk of populations to be tested, and varying rates of regional prevalence of viral infection – all of which influence the utility of testing. On May 4, 2020, the Food and Drug Administration (FDA) issued a revision to its initial, flexible policy and now requires the FDA to grant emergency use authorization (EUA) for antibody tests, and created a special website for the summarized performance of the serology tests that are granted EUA. 4
As businesses consider their approaches to reopening, it is likely that employers will set precedent and determine antibody testing practices and norms. Although antibody testing should not be used to determine which employees go back to work, it can be used to better guide how employees go back to work in order to protect the safety of employees, customers and the public. We convened Chief Medical Officers from several national payors, laboratory companies, retail pharmacies, and provider organizations to develop consensus around basic guidance, and a simple algorithm that employers can use to guide thinking around testing policy during reopening once more is known about the protection conferred by the presence of antibodies. While we all recognize that this is far from perfect, our goal was to suggest key considerations and provide a framework that helps guide the decision-making process for employers. We should underscore that antibody credentials should not determine whether an employee can or cannot return to work, as such policies could cause meaningful hardship (similar to concerns with policies regarding the presence of mental health or social limitations).
Once it is clear from the local government and public health authorities in a specific geography that it is appropriate for the company or job category to RTW, several key factors should be considered in constructing an effective program. The first relates to the characteristics of the test. We anticipate that antibody tests will be used primarily to test for immunity, and not to identify active infection. The delay in generation of measurable Immunoglobin M makes antibody testing far less useful for rapid infection detection when compared with molecular or antigen testing. When assessing immunity, the test characteristic of focus is the test's specificity. Considering the relatively low prevalence of the virus in most regions, specificity lower than even the high 90s likely will produce more false positives than true positives, limiting the ability to interpret testing. Although the early available tests had widely variable reported specificities, IgG antibody tests with demonstrated high specificity (>99%) are now available from large national laboratory companies, making the tests far more interpretable. For individual and population health measurements, we believe a threshold of greater than 99% specificity is a prerequisite for IgG antibody testing.
The second key variable relates to employee characteristics. Three categories of employees should be considered for antibody testing. The first and potentially most useful population to test is health care workers. There may be value to knowing who is antibody positive and therefore may be immune to future coronavirus infection in order to make decisions about who should deliver care on the front line, how to best conserve personal protective equipment (PPE), and how to reduce the need for subsequent symptom checks and molecular or antigen screening, all while reducing exposure to patients who need in-person health care services. 5 The second employee population who should be considered for antibody testing is those who work in close proximity to colleagues and cannot practice social distancing (eg, meat-packing facilities). For those firms providing essential services, antibody testing could enhance planning to reduce exposures to those still susceptible to the virus, reduce spread, and increase the likelihood that those firms can reopen safely. The third employee population to consider is those who have frequent exposures to customers where social distancing may be challenging (eg, checkout clerks at retail outlets), and where physical barriers and sneeze guards may be difficult to construct and employees will have extended close contact with customers. Although these settings may be easier to manage with PPE, employee role placement and use of PPE could guide safer reentry practices.
The third key variable to determining the need for antibody testing is the underlying regional viral prevalence – the proportion of the population who have been infected. If the prevalence is very low, then the yield of the antibody test will not be revealing, and will not provide meaningfully actionable results. More specifically, in a region with prevalence of viral infection that is less than a specific threshold (eg, 3%), antibody testing will identify so few antibody-positive employees that little useful resource allocation or safety policy could be implemented. When seroprevalence is at higher levels, such as currently seen in New York and northern New Jersey, the value of population-based serology testing increases, with lower false-positive rates and a meaningful yield of IgG-positive individuals who, once recovered, are unlikely to bring SARS CoV-2 (severe acute respiratory syndrome coronavirus 2) into the workplace and also may not require surveillance at the same level as for IgG-negative individuals. Large employers with employees in multiple geographic regions should make decisions about testing at the local market level, as prevalence will vary geographically. As more testing occurs across the country, large testing laboratory data can inform on local seroprevalence. Nonetheless, we do not have a systematic way to assess local prevalence of the virus today – a critical variable in testing determinations for employee populations. The Centers for Disease Control and Prevention and the National Institutes of Health have initiated antibody testing in regionally representative samples, and those results will be foundational to thoughtful decision-making about testing. These sampling initiatives also will be essential to address disparities in care, as local prevalence rates are currently reflective of underlying testing rates, which have been shown to vary by sociodemographic characteristics. 6,7
These 3 variables can be used to generate a simple algorithm to determine which employers should consider antibody testing for their employees (Figure 1).
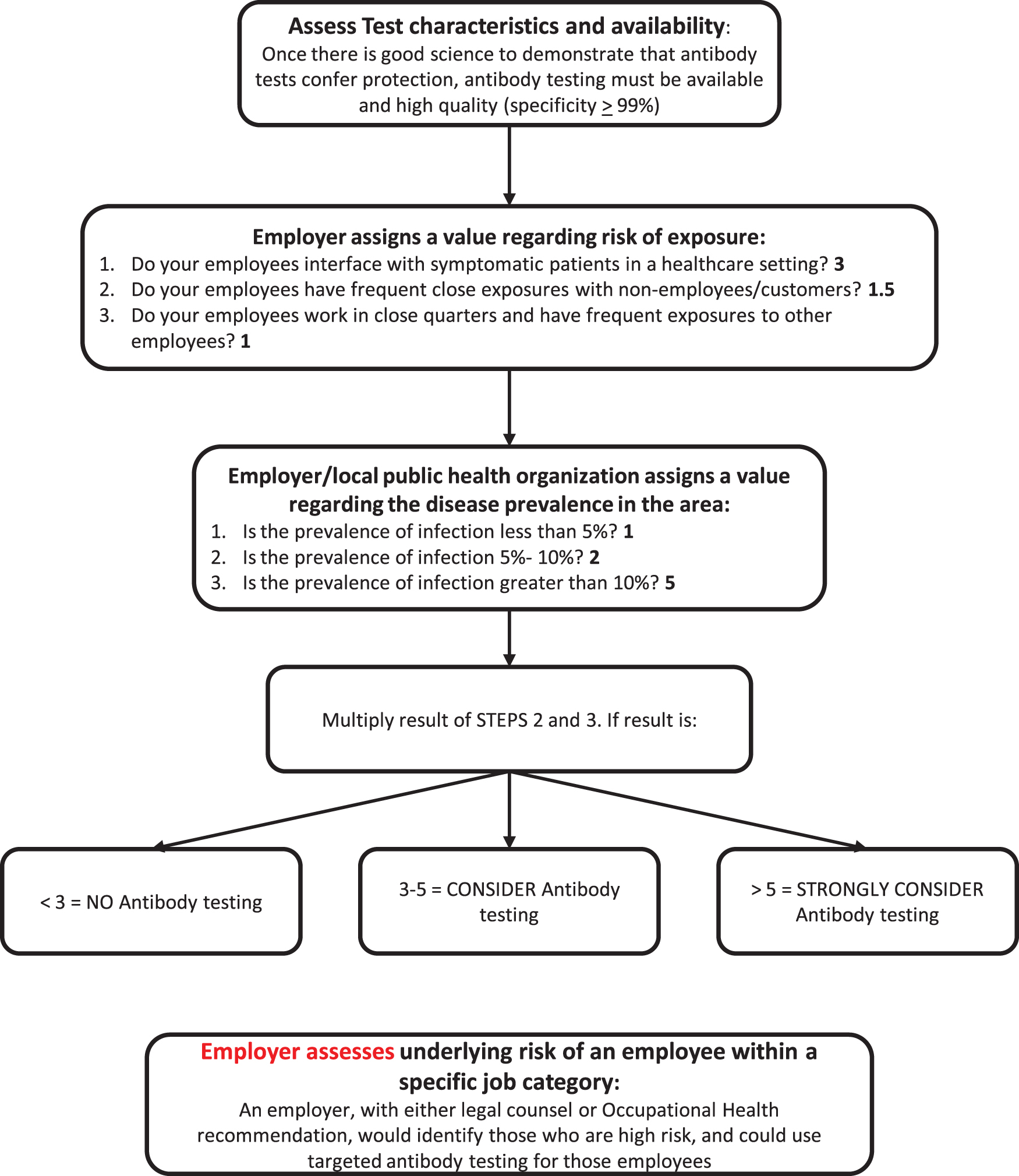
A simple algorithm to determine which employers should consider antibody testing for their employees.
Employers may consider one other variable – an individual employee's risk. For employees with specific, high-risk comorbidities (eg, immunocompromised, chronic lung disease), individual antibody testing may assist in determining appropriate timing for RTW and optimal protective measures for the employee. In the absence of immunity, these employees could benefit from continued social distancing and work from home flexibility. Any decision to test individual employees based on health risk must be made in accordance with employment regulations to be sure no employees are discriminated against based on their existing health conditions. These decisions likely will require case-by-case determinations by occupational health professionals within organizations or with legal counsel to foster a safe work environment without compromising privacy or infringing on ERISA (Employee Retirement Income Security Act of 1974) requirements. Moreover, if we ultimately observe high proportions of individuals testing antibody positive, we will need to reassess evolving levels of risk as herd immunity may be achieved.
RTW antibody testing should be framed as a safety effort. It is possible that immune credentials or lack of them and the policies associated with those credentials (in terms of time off, special benefits, or limitations at work) might cause a myriad of hardships for individuals based on the status of their credentials. This could generate a variety of legal, ethical, and workflow challenges. These issues should be carefully considered prior to initiating broad serology screening.
If an employer does implement serology-based testing as a component of a RTW program, other components of that program will need to be considered to make it holistic and effective. These include onsite temperature screening, symptom attestation, molecular or antigen testing for symptomatic individuals or in the context of surveillance, and plans for contact tracing and isolation for those who do become infected.
Without question, any simple algorithm cannot account for the myriad permutations of individual employer or employee concerns or considerations that may arise. Moreover, we acknowledge that any threshold defined here is not precise or absolute, and should be thought of as directional. The science must rapidly confirm that a positive IgG antibody test confers meaningful and durable immunity as a prerequisite for decision-making. Nonetheless, we hope that by achieving consensus on guiding principles and a simple framework we may be able to reduce some of the complexity that employers are facing as they consider the use of antibody testing in the safe return to the workplace. Large employers with ongoing RTW programs should share data to inform best practices around integrated RTW testing programs. We hope to test and refine these concepts to continue learning and structuring policies to encourage safe workplaces.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
The authors received no funding for this article.