
Abstract
Interventions to support patients with complex needs are proliferating. However, little attention has been paid to methods for identifying complex patients. This study aims to summarize approaches used to define populations with complex needs in practice, by cataloging specific population criteria and organizing them into a taxonomy. The authors conducted a pragmatic review of literature published January 2000-December 2018 using PubMed. Search results were limited to English-language studies of adults that specified a set of objective criteria to identify a population with complex needs. The authors abstracted data from each article on population parameters, and conducted thematic analysis guided by deductive coding. The review identified 70 studies reflecting 90 unique complex population definitions. Complex populations criteria reflected 3 approaches: stratification, segmentation, and targeting. Six domains of population criteria were found within, including age-based criteria (59 populations); income (12); health care costs (45); health care utilization (39); health conditions (35); and subjective criteria (15). Criteria from multiple domains were frequently used in combination, and exact specifications were highly variable within each domain. Overall, 83% of the 90 population definitions included at least 1 cost- or utilization-based criterion. Nearly every study in the review presented a unique approach to identifying patients with complex needs but a limited number of “schools of thought” were found. Variability in definitions and inconsistent terminology are potential sources of ambiguity between stakeholders. Greater specificity and transparency in complex population definition would be a substantial contribution to the emerging field of complex care.
Introduction
Interventions to support patients with complex needs are proliferating, and selection of a target population is central to intervention planning. In practice, complex care programs generally use a set of objective and/or subjective criteria to select eligible patients, such as focusing on patients with high costs, frequent utilization, or multiple chronic conditions. 1 Given the heterogeneity of patients with complex needs, a single care model or program cannot meet the needs of all subpopulations. 2 This has led to much experimentation with regard to the ideal design of interventions for maximum impact, titrating program design elements including mix of services, program staffing model, and timing of intervention delivery.
The optimal approach to defining “patients with complex needs” is a matter of ongoing discussion in the field. 3 Often, theoretical descriptions of patients with complex needs are framed around the biopsychosocial model of disease, which describes the interconnectedness of biological and psychosocial factors in determining health and wellness. 4 Although taxonomies exist to describe the major groups of complex patients, these are often high level. Most prominent is the taxonomy put forward by the National Academy of Medicine (NAM), 1 which categorizes complex patients into 6 clinical and functional groups: children with complex needs, non-elderly disabled, multiple chronic, major complex chronic, frail elderly, and advancing illness. Social risk factors and behavioral health factors crosscut through these groups. 1 The NAM taxonomy represents a theoretical framework for groups of complex patients and highlights the interplay between medical, behavioral, social, and functional status factors. However, it does not reflect the diversity of current operational approaches to identify patients for complex care programs.
While evidence about the design of effective interventions for populations with complex needs is slowly accumulating, 1,3,5 less attention has been paid to exploring the implications of patient selection decisions in the complex care field. Often, discussions of evidence surrounding complex care programs treat population selection as a sidebar and focus on the design of services rather than the specification of population criteria. As a result, little evidence is available about the advantages and disadvantages of the many ways to conceptualize complex care populations.
This study aims to catalogue and summarize the range of approaches being used to define populations with complex needs to provide insights that support informed decisions about population selection for complex care interventions. This pragmatic review of the literature presents a holistic survey of the variety of ways in which complex populations are being defined and organizes these approaches into a framework. This review can inform efforts to compose populations of complex patients for intervention planning, post hoc descriptive analyses, or predictive modeling. This study highlights some of the most common approaches and discusses implications of the variability in methods for identifying complex patients.
Methods
This study employed a pragmatic review of the literature. A pragmatic review aims to summarize a body of literature most efficiently by avoiding duplication of effort while maintaining the essential rigor and comprehensiveness of a systematic review. 6,7 A pragmatic approach is appropriate when the question of interest is broad and not intended to guide treatment for specific types of patients. Nevertheless, the methods used were largely consistent with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 8 Specifically, the pragmatic compromises made included searching of a single computerized database by one reviewer, development of a custom search term because of a lack of relevant MESH terms, and use of a team-based data abstraction process.
Search strategy
The research team searched PubMed in March 2019 for studies published January 2000-December 2018 (including advanced and online-first publications) using the following search profile: (“population health management” OR “utilization management” or “risk management”) and (“high-need” or “complex needs” or “high-cost”) and (identif*). Reference lists of studies retrieved were reviewed to identify any relevant papers that were not captured by the search terms.
Eligibility screening
A 2-phased process was used for eligibility screening with explicit criteria. First, studies were potentially eligible if they were published in English between January 1, 2000-December 31, 2018, included adults aged 18 years and older, and involved the use of objective criteria to identify a complex needs population for any purpose (studies must have specified a set of concrete criteria for defining the “complex needs” study cohort). Studies were then excluded from the sample if they focused on a single health condition, presented individual case studies, or were student dissertations and theses, trial protocols, or newsletters and commentaries without presentation of quantitative data.
One screener (TAO) reviewed the titles and abstracts of publications identified using the search strategy. Full-text articles were pulled for all publications that were not eliminated during title and abstract screening. Two screeners (TAO and LJL) then reviewed the full text of articles and applied all inclusion and exclusion criteria to arrive at the final sample of included studies.
Data abstraction
Two members of the research team (TAO and LJL) systematically abstracted relevant data from each article using a Microsoft Excel-based data abstraction form. The data elements abstracted included: full citation, article intent (program/intervention, descriptive analysis, or predictive modeling), setting/data source, objective criteria used to define the study population, notes regarding any element of subjective criteria or processes in the study population inclusion and exclusion logic, and a general category of reviewer notes. Published appendices and other supplemental article materials were used as needed to obtain all data elements.
Each team member independently abstracted data for half of the studies. The coders then exchanged the data for secondary review and confirmation. Finally, together with a third team member (ACD), the coders reviewed and discussed any studies for which data abstraction was unclear or for which there was disagreement. Articles were discussed until consensus could be reached.
Synthesis
To synthesize insights about strategies for identifying and selecting complex populations, the research team then reviewed the abstracted data related to objective and subjective criteria or processes for complex population identification, as well as study setting and data source, using a thematic analysis approach guided by a deductive coding process and data displays. Study setting and data source were included in this synthesis because some study populations were narrowed as a byproduct of these study features even though they were not presented as explicit population criteria in the original studies (eg, studies using Medicare data were focused on seniors and persons with disabilities).
Two team members (TAO and ACD) jointly reviewed the abstracted data to identify and organize the population criteria into domains and subdomains. Then, one team member (TAO) applied the domains and subdomains to the abstracted data for all studies included. Finally, for quality assurance, 20% of the articles were reviewed by a third team member who did not participate in the synthesis process (LJL) to confirm the accuracy of the domains as applied to the abstracted data. This quality assurance review did not identify any errors.
Finally, the team applied a framework presented by NAM in its report on effective care for high-need patients,1(pp 36–37) to further characterize the domains of population criteria identified. The NAM framework presented 3 different approaches to identifying patients with complex needs: stratification methods, segmentation methods, and patient targeting.
Stratification methods separate a population according to risk level (eg, spending or utilization; may be past or future, persistent or acute). Stratification methods do not yield homogenous clusters of patients with shared needs or characteristics. For example, the top 1% of patients with high costs are heterogeneous in their characteristics and needs. 9
Segmentation methods aim to drive toward homogenous groups of people with shared needs and characteristics (eg, clinical, behavioral, or social characteristics or needs). Patient segments may be heterogenous in risk level depending on the granularity of segmentation. For example, segmentation based on presence of conditions such as diabetes and kidney disease would yield a population that is more heterogeneous in terms of risk level, while segmentation based on severity of diabetes and kidney disease would homogenize risk level to a greater extent.
Patient targeting is used to identify clusters of people who are suited for a given intervention, based on presence of “actionable” needs (eg, transportation needs, polypharmacy). Although this approach might be thought of as an action taken to match patients to services after they have already been identified, some programs may use highly targeting criteria to select patients, such as programs that enroll patients based on an assessment/screening for specific needs.
Descriptive summaries of study data according to the domains and subdomains identified are presented.
Results
A total of 3411 citations met the search criteria; after screening at the title/abstract stage, 81 full-text articles were assessed for eligibility. Of these, 11 were excluded after full-text review, and a total of 70 papers were included in the final sample for qualitative synthesis (Figure 1). 9 –78

Diagram of study selection process for qualitative synthesis.
Within these 70 papers, the research team identified 90 distinct complex populations (some studies presented multiple distinct cohorts of complex patients). A detailed tabulation of inclusion and exclusion criteria for complex patient population definitions, as abstracted for the 90 populations from the 70 studies in the review, is provided in Supplementary Table S1 (online Supplementary Data).
Based on the thematic review and synthesis, the research team developed a hierarchy of population definition components. At the highest level, the team grouped inclusion and exclusion criteria for selecting complex patient populations into domains. In total, 6 domains of criteria for complex population selection were identified (Figure 2). Five of these were based on objective data, including health care costs (used as a criterion in 45 out of 90 complex population definitions) 9 –12,16,19,21 –23,26,28 –31,34,35,37 –39,44,47,50,51,54,55,58,60,64,67,72,74,75,77,78 ; health care utilization (39/90) 9 –12,16,19,21 –23,26,28 –31,34,35,37 –39,44,47,50,51,54,55,58,60,64,67,72,74,75,77,78 ; age (59/90) 9,10,13,15 –17,19,20,22 –25,27,28,32 –36,40,42,43,45,47,48,51 –53,56 –58,60,61,63 –67,69,71 –75 ; income (12/90) 12,14,18,21,48,54,56,64,71,72,74,75 ; and health conditions (35/90). 12,15,17,20,21,23,25,27,28,32,42,45,48,50 –53,59,61 –63,65 –69 The sixth domain encompassed approaches based on more subjective methods of patient selection such as provider referral (15/90 complex populations). 13,21,24,30 –32,45,52,53,57,62,64,68,70,75
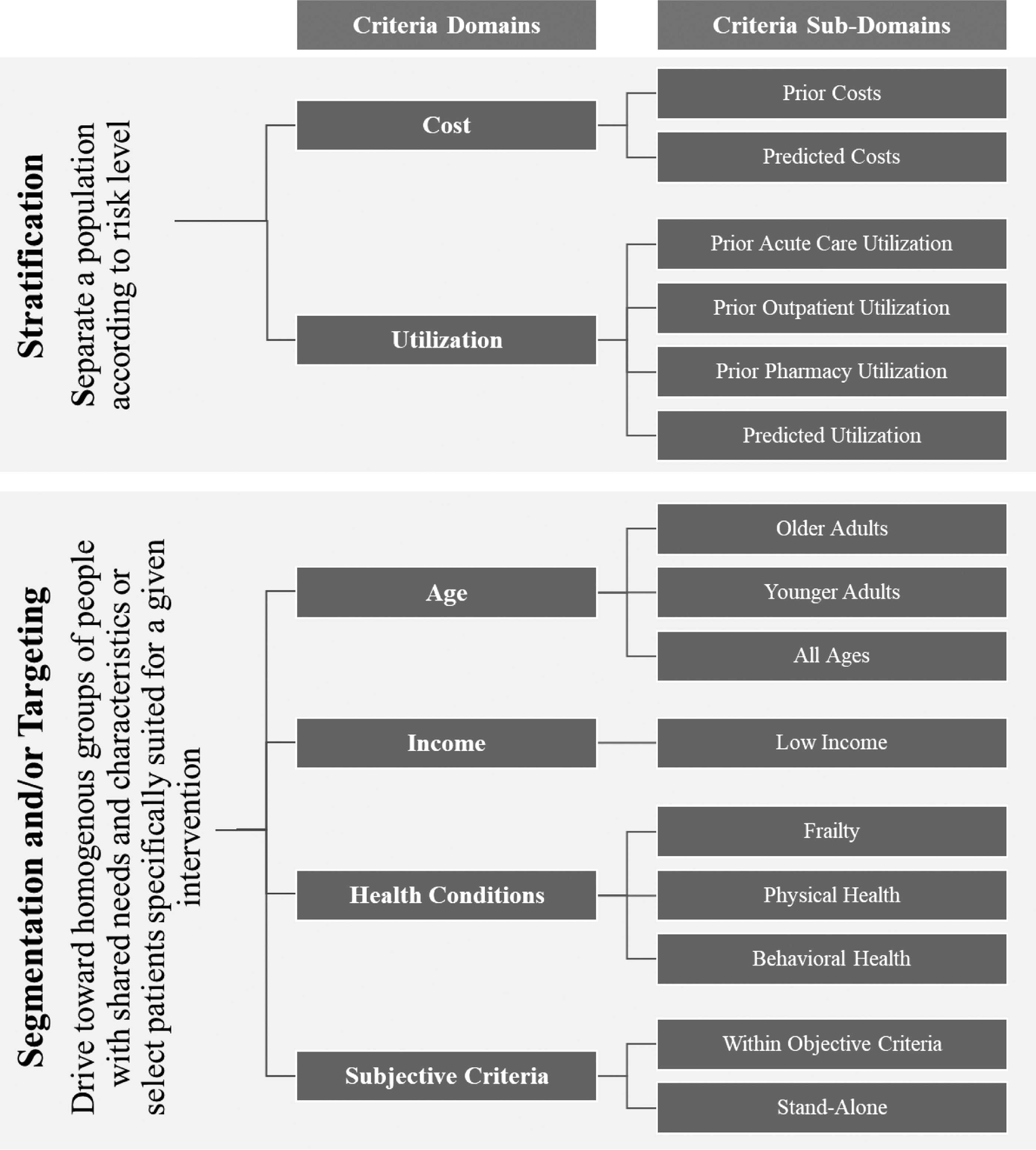
Domains and subdomains of criteria for defining populations of patients with complex needs. The cost- and utilization-based criteria in this framework can be thought of as stratification approaches, while age, health status, and income-based criteria can be thought of as segmentation approaches or targeting approaches, depending on their construction. Most population definitions reviewed combined stratification and segmentation approaches, using a mix of criteria capturing cost and/or utilization as well as health conditions, age, or income.
Within each domain of population criteria, the research team identified subdomains through iterative clustering of the criteria within each domain (Figure 2). For example, the domain of cost-based criteria was split into subdomains of approaches focusing on (a) prior costs versus those focusing on (b) predicted costs.
Building on the NAM framework for approaches to identifying high-need patients, 1 the team classified the domains of cost- and utilization-based approaches as stratification methods. In contrast, age-, income-, and health-based approaches, as well as subjective approaches were classified as segmentation and/or targeting methods (Figure 2).
In this review, most studies employed a combination of criteria across several domains to structure their complex population (Table 1 and Supplementary Table Table S1), highlighting that the 3 broad approaches (stratification, segmentation, and targeting) are not mutually exclusive. Many complex patient populations were defined using criteria that combine the approaches, such as by identifying high-risk patients based on their prior costs, and then segmenting the high-risk group into subgroups based on their functional limitations or clinical needs. The team analyzed the ways in which criteria from multiple domains were used in combination with one another. The most commonly used combination of criteria was an age-based criterion in combination with a cost-based criterion (15 out of 90 complex population definitions), 9,10,16,19,22,28,34,35,47,51,58,60 followed by age with health conditions (12/90), 17,20,27,42,48,51,61,63,65,69 and age with utilization (8/90). 33,36,40,43,51,73 Criteria could be combined with “and” or “or” logic (Table S1).
Distinct Combinations of Domains of Complex Population Criteria and Frequency
In total, 75 of the 90 complex population definitions (83.3%) included a cost-based criterion, a utilization-based criterion, or both 9 –16,18,19,21 –26,28 –41,43 –47,49 –62,64,66,67,70,72 –78 ; 35 of 90 (38.9%) included a health conditions-based criterion 12,15,17,20,21,23,25,27,28,32,42,45,48,50 –52,59,61 –63,65 –69 ; and 89 of 90 (98.8%) had at least 1 criterion from the cost, utilization, or health domains (Table 1). Among the 75 populations defined using objective measures of cost or utilization, 14 of 75 (18.7%) also included a subjective component (eg, referral or screening of the candidate patient list). 13,21,24,30 –32,45,52,53,57,59,62,64,70,75 Among the 35 populations that included a health-based criterion, 7 of 35 (20%) included a subjective component. 21,32,45,52,59,62,68
Finally, the team characterized the dimensions on which criteria varied, after reviewing the detailed population specifications used by the studies in the review (Table 2). Cost-based criteria varied along 5 different dimensions: the threshold set for level of spending (eg, top 5%); the time period applied to the criteria (eg, prior year); the use of explicit specifications for narrowing types of costs being counted (eg, excluding pharmacy or long-term care costs); the method used to classify costs (eg, a percentile-based approach vs. setting a specific dollar amount threshold); and lastly, whether the cost assessment was retrospective or predictive. For example, Cunningham et al defined complex patients as those whose spending was in the top 25% in the prior year, 19 while Bell et al selected patients whose predicted costs in the next year were 50% higher than the average Medicaid recipient. 12 These same dimensions of variation also were seen in utilization- and health-based criteria; age- and income-based criteria were much simpler in their specifications (Table 2).
Dimensions of Variation in Specification of Population Criteria, by Domain
NA, not applicable.
Discussion
In this review of 70 papers containing 90 populations of patients with complex needs, the research team observed a multitude of approaches to defining complex populations. The team presents a framework of simple language that distinguishes broad approaches (stratification, segmentation, and targeting) and categorizes specific types of criteria into 6 domains and 15 subdomains, with itemized dimensions of variation in criteria components. In the studies reviewed, population criteria from multiple domains were used in combination with one another, with expansive variability in how individual criteria were specified. The result was that nearly every study used a unique approach to identify patients with complex needs.
Nevertheless, approaches tended to cluster around specific conceptual and operational groupings. Age-based approaches were most ubiquitous but were relatively simple as they varied only in lower and upper bound thresholds. More complicated (and variable) was the specification of cost, utilization, and health conditions-based approaches. The team observed population definitions in these domains that varied along multiple different dimensions at once. Some examples of approaches were more nuanced than others, such as acute care utilization criteria that focused specifically on treat and release visits to the emergency department, 14 or cost-based criteria that used multiple years of data to establish persistence of high spending. 74 The team also noted several population definitions that relied on more complex (and sometimes proprietary) computed scores that were based on data from multiple domains and/or subdomains. 21,72,73
Age-based (and income-based) criteria often were presented as byproducts of data considerations, such as data source or setting of the study (eg, studies based on Medicaid data were focused on low-income patients; studies based on Medicare data usually were focused on older adults) rather than as intentional patient selection decisions rooted in conceptual understanding.
The NAM report framed 3 core approaches to identifying populations with complex needs: stratification, segmentation, and targeting. The research team applied this framing to the domains of criteria observed in the complex care population definitions found in this pragmatic review. The cost- and utilization-based criteria in the framework can be thought of as stratification approaches, while age, health conditions, and income-based criteria can be thought of as segmentation approaches or targeting approaches, depending on their construction. Most population definitions reviewed combined stratification and segmentation approaches, using a mix of criteria capturing cost and/or utilization as well as health conditions, age, or income.
The team observed the use of subjective criteria for defining complex populations; in general, these were found in studies describing programs/interventions, when there were frontline processes related to intervention delivery through which subjective eligibility determinations could be applied. The addition of subjective criteria may be used to narrow an otherwise heterogenous group of patients and can be thought of as a segmentation approach (seeking more homogenous groups of individuals) or a targeting approach (seeking out specific individuals with actionable needs).
Amid the diversity of approaches observed, many were similar in intention and demonstrate that there are “schools of thought” that likely reflect the specific priorities of individuals in the complex care community with regard to how to identify patients with complex needs. “High utilizer” approaches based on costs and/or utilization combined with an age-based criterion were the most common. In some instances these criteria were combined with a subjective determination, reflecting a desire to, for example, reduce health care utilization among older adults who might benefit from a specific intervention or program. Other schools of thought that the team posited based on this review were represented by criteria focused on predictions (future risk or health) found in both cost and utilization domains; and approaches to identifying “clinically complex” patients by specifying criteria focused on measures of health conditions or functional status.
However, within schools of thought the research team observed an array of distinct criteria specifications, given the wide variability observed across multiple dimensions of each criterion and the combinations of criteria. For example, a common construct was the “frequent acute care utilizer,” but the team observed many variants of this construct: 4+ treat and release emergency department visits in the prior year 14 ; 1+ inpatient stay in the prior year 25 ; 3+ emergency department visits or inpatient stays in the prior year 32 ; 2+ emergency department visits in the prior 28 days 46 ; predicted inpatient readmission risk score of ≥50 out of 100 within the next year 56 ; and so on.
Very little information is available about how important distinctions such as these are, in which conceptually similar definitions employ distinct thresholds or look-back periods. In general, studies rarely discussed the rationale for their approach to identifying complex patients, or the process through which population criteria were selected (eg, via expert opinion, health system prioritization, exploratory analyses). Without information about the implications of these varied approaches to defining constructs of complexity, it is very difficult to draw meaning from the complex care literature. Poor match of intervention services to patient needs can be one reason for program failure, and better understanding the implications of population selection decisions is critical to interpreting and comparing results of interventions.
Limitations
Although this study is a comprehensive assessment of the current landscape of approaches to conceptualizing and identifying patients with complex needs, it has several limitations. The team conducted a pragmatic review and the scan may not have included every paper in the literature that defined a population of patients with complex needs. Studies were included that were described by the authors as focusing on populations with complex needs, high needs, or high costs, but authors varied in their intentions. The team did not observe examples of selection criteria representing measures of social needs. However, this was not an explicit term in the search strategy. Furthermore, few data sources such as claims or electronic health records contain discrete data fields on social needs, and thus their absence from the review may be a reflection of their absence in underlying data systems. 79
The variability in approaches to identifying patients with complex needs has strengths and weaknesses. Given the general agreement that patients with complex needs are a composite of many distinct subgroups, testing of many different population criteria contributes to growing understanding of these subgroups. The diversity of approaches also provides examples of methods that may work in certain contexts (eg, utilization-based methods can be used in contexts that do not have access to cost information).
It may be that the time is right for leaders in the field of complex care to consider a more focused and standardized approach to definition of complex patient populations as one means to further the field through comparable and translatable evidence. The variability in the populations studied is a barrier to drawing generalizable conclusions about programs, population needs, or intervention opportunities. Importantly, it is also a potential source of ambiguity and confusion between stakeholders in the complex care community, who may have different mental maps regarding what constitutes complexity. However, it may be infeasible to standardize definitions of patients with complex needs because criteria chosen and how they are specified may depend on the setting, data available, and other factors.
Conclusion
Complex care program designers need more information about the comparability of the many distinct ways of identifying complex populations. The aim of this pragmatic review was to develop a detailed characterization of the ways that patients with complex needs are identified and to synthesize these approaches into a framework to better support informed population selection decisions for complex care interventions. Greater specificity in the language used to talk about population selection and more transparency surrounding the details of the population criteria and rationale for their use would be a substantial contribution to the emerging field of complex care and its expanding evidence base.
Footnotes
Acknowledgments
The authors express their gratitude to the following individuals who contributed to the conceptualization and development of this work and shared their insights generously: Melinda Abrams (The Commonwealth Fund); Jose Figueroa (Harvard University); Jessica Hughes (New York Health and Hospitals); Rachel Davis, Karla Silverman, and Stefanie Turner (Center for Health Care Strategies); and Mariana Saenz and Michelle Wong (Kaiser Permanente). We are also grateful to Jacob Quinton for his thoughtful comments on early drafts of this manuscript. Finally, the authors also wish to thank the leaders of the Kaiser Permanente CORAL Initiative and the Kaiser Permanente Care Management Institute's Care for Complex Needs Program.
A preliminary version of this work was presented as a poster at the 2019 AcademyHealth Annual Research Meeting in Washington, DC. A related abstract was selected for presentation at the 2020 AcademyHealth Annual Research Meeting. The abstract will be published as part of meeting proceedings although the meeting has been moved to a virtual format.
Author Disclosure Statement
All authors declare that there are no conflicts of interest.
Funding Information
This project was supported by Kaiser Permanente's Garfield Memorial Fund, under its Complex Care Collaboration: Research, Operations and Leadership (CORAL) portfolio.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.