
Abstract
Implementing emergency department (ED) and hospital patient throughput management coupled with at-home medical and tele-management upon discharge may increase surge capacity during national emergencies and pandemics. This novel intensive transitional care management (ITCM) intervention presents the opportunity to optimize hospital bed capacity through prevention of inpatient admissions for patients who could be discharged home safely with appropriate in-home medical support and tele-management. This observational cohort intervention was conducted between April 7, 2020 and April 30, 2020, at the 4 largest inpatient facilities of RWJBarnabas Health System in New Jersey. The intervention group included a convenience sample of 192 patients who were evaluated in the ED, monitored in the observation unit, or admitted to the hospital with a diagnosis of mild-to-moderate COVID-19 infection. Their outcomes were compared to a matched comparison group of 593 patients who were admitted with the same COVID-19-related diagnosis and severity. The primary outcome was the reduction in inpatient days as a result of the intervention that included provision of at-home oxygen supplementation therapy, expanded home care services, and tele-management sessions. Secondary outcomes were re-encounters with the health system in the ED, observation unit, or inpatient readmissions. A total of 481.6 hospital patient days were avoided for 78 patients who had been discharged from the ED or observation unit stays. Secondary analysis included hospital readmission rates. The ITCM intervention demonstrated a feasible strategy for improving throughput of patients with COVID-19, resulting in increased hospital bed capacity.
Introduction
The COVID-19
Background
COVID-19 is the seventh coronavirus to circle the globe. In many ways it is similar to the other coronaviruses, which were positive RNA (ribonucleic acid) viruses and Baltimore Class IV subtype that infect humans. However, one notable difference is the ease with which the COVID-19 virus enters the host cell, which is estimated to be 1000 times more efficient than with SARS (severe acute respiratory syndrome) or MERS (Middle East respiratory syndrome), making widespread transmission a central challenge. 4 –6 Symptomatic patients often present with fever and dry cough, and depending on the severity of the lung injury, there is a decrease in oxygen saturation. 7 For patients who are paucisymptomatic and mildly hypoxic, the World Health Organization and the Centers for Disease Control and Prevention have recommended supportive oxygen therapy as the first-line therapy. 8,9 Approximately 81% of patients with COVID-19 present with mild disease, typically reflected in oxygen saturations of 90% or above. 10 This subpopulation of patients may not require inpatient hospitalization and could potentially benefit from at-home oxygen supplementation and monitoring. However, during the COVID-19 crisis there was a critical shortage of many supplies, including home oxygen concentrators and home monitoring equipment. 11 Traditional home care services were neither ready nor equipped to provide daily telenursing monitoring services. In addition, many primary care providers' offices were either closed or unavailable for daily telemedicine monitoring.
As the pandemic expanded across the country, the majority of hospital beds were occupied by patients with COVID-19 in moderate-to-severe distress, many requiring high flow oxygen therapy or mechanical ventilation. 12 Hospital inpatient wards also admitted patients who were less acutely ill but could not be safely discharged home because of the need for oxygen supplementation and close monitoring that was not readily available in the community. 11
During the initial peak of the COVID-19 pandemic, health systems encountered significant capacity challenges. 13 The fear and the reality of hospitals being overwhelmed by patients, critical shortages of beds, medical supplies, equipment, and personnel resulted in state and federal authorities taking urgent and unconventional measures to expand capacity. 14 As the federal and state governments mandated inpatient bed expansion, converted public spaces to makeshift field hospitals, even dispatching a United States Navy hospital ship to increase capacity, these strategies did not alleviate the need for staffing the additional beds nor did they address medication and equipment shortages. 11,15,16
The Urban Institute's 2020 Hospital Readiness COVID-19 Report indicated that in 2018, the United States had 728,000 medical and surgical hospital beds available, or 2.2 hospital beds per 1000 population with only approximately 36% of these beds available on a typical day and approximately 0.8 beds per 1000 population unoccupied. 17 The report also noted that the number of available beds in New Jersey (NJ) was 19,476, with 2.2 beds available per 1000 population, resulting in 6554 unoccupied beds or 0.74 unoccupied beds per 1000 population. 18 According to the NJ Hospital Reporting Portal COVID-19 Dashboard, during the 2-week peak of the COVID-19 surge, NJ hospitals averaged 7628 hospitalizations for patients with COVID-19, peaking at 8084, reported on April 14, 2020. 19 The significant shortage of inpatient beds resulted in the emergency departments (EDs) and observation units being used as entry portals to inpatient beds, stretched beyond physical, staffing, and resources capacity.
Health care systems facing the challenge of managing the ongoing demands of the COVID-19 pandemic need to explore opportunities to mitigate the need to rely on the limited bed capacity of acute care hospitals. Research suggests that patient throughput management and care management at home could lessen the burden on the health system and increase surge capacity during emergencies such as this. 18,20,21
To address the need to optimize inpatient bed capacity and reduce the number of patients with COVID-19 remaining in the ED and observation unit until inpatient beds are available, the authors conceptualized, implemented, and assessed a novel intensive transitional care management intervention aimed to improve patient throughput and increase bed capacities at 4 RWJBarnabas (RWJBH) Hospitals.
Description of the Intensive Transitional Care Management (ITCM) Intervention
The ITCM intervention for patients positive for COVID-19 and/or persons under investigation (PUIs) for COVID-19 includes expanding home health services to include home oxygen supplementation and daily medical monitoring of patients via telemedicine and telenursing to ensure safety and maximize outcomes.
Under the RWJBH COVID-19 Assessment Protocol (Figure 1), patients were included in the ITCM intervention if they met the following inclusion criteria: (1) confirmed or suspected (PUI) of COVID-19 diagnosis, (2) medically stable to be discharged home with supportive care, (3) oxygen saturation ranging from 90% to 93%, (4) availability of a caregiver, (5) ability to self-care safely at home, and (6) access to a computer, tablet, or a phone with video capabilities.

RWJBarnabas Health COVID-19 assessment protocol. DC, discharge; EKG, electrocardiogram.
The ITCM model included the following key elements (Figure 2):
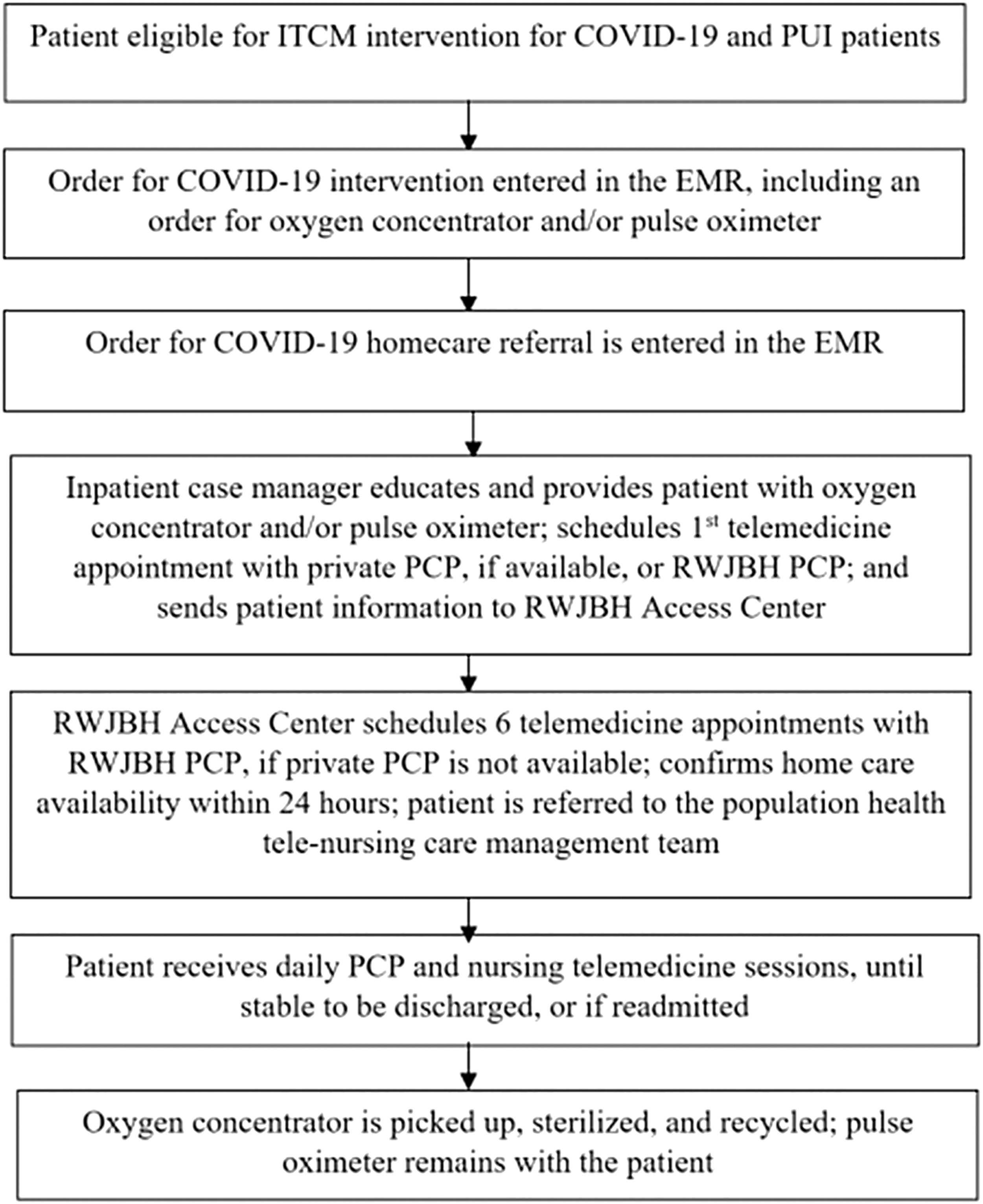
ITCM intervention workflow. EMR, electronic medical record; ITCM, Intensive Transitional Care Management; PCP, primary care physician; PUI, persons under investigation for COVID-19 infection; RWJBH, RWJBarnabas Health.
Provision of oxygen concentrator and/or pulse oximeter
The case manager provided education about and demonstration with an oxygen concentrator and/or pulse oximeter (depending on the O2 levels) using the teach-back method to ensure the patients understood the instructions.
Daily telemedicine visits with primary care provider (PCP)
Upon discharge, the case manager contacted the patient's PCP to schedule a telemedicine appointment within 4–6 hours of the patient arriving at home. If the PCP was unavailable or unreachable, patients were scheduled to be seen by RWJBH-employed physicians. If the patient's PCP was subsequently available, the care was transferred to the private PCP following communication between the 2 providers.
Home care telenursing services or daily telenursing with population health care management nurses
All patients who were qualified for home care services, and in whose respective geographic areas the services were available, received an initial face-to-face visit within 24 hours. Home care nursing services follow-up via telemedicine continued daily until patients were ready to be discharged or were readmitted to the hospital. Home care services were provided by the Visiting Nurse Association Health Group of New Jersey, a nonprofit home health and hospice agency affiliated with RWJBH.
For all patients who were ineligible for home care services, if the services were not available in their respective geographic areas or if the initial home care nursing encounter was not possible within 24 hours of discharge, the intervention included a telenursing encounter with population health care manager nurses, who contacted the patient within 24 hours of arrival at home.
The home care nurses or population health nurse care managers provided daily nursing assessments that included at a minimum, oxygen saturation levels, temperature, and intake and output.
The initial length of the intervention was planned to be 7 days per patient; however, based on patient needs, the average intervention length was 11 days per patient, ranging from 1 to 37 days. Patients were instructed to call 911 immediately if they experienced O2 saturation <90%, severe chest pain, or worsening shortness of breath. Patients continued to receive the intervention until their PCP determined the patient was medically stable for discharge or if the patient was readmitted to the hospital, at which point the oxygen concentrators were picked up, cleaned, sterilized, and prepared for future use.
Methods
Design and setting
The intervention was conducted between April 7, 2020 and April 30, 2020 at the 4 largest inpatient facilities in the RWJBH System. Collectively, these facilities comprised a total of 801 staffed medical and surgical beds: Saint Barnabas Medical Center (n = 324), Newark Beth Israel Medical Center (n = 135), Clara Maass Medical Centers (n = 126), and Jersey City Medical Center (n = 216). During the study period, each facility reported the number of staffed medical and surgical beds daily, based on their available staffing during this period. The percentage of available medical and surgical staffed beds during the peak of COVID-19 admissions between April 6, 2020 and April 21, 2020 ranged between 1.8% (n = 14) to 5% (n = 40) (Figure 3).

Percentage of staffed beds available in study hospitals from April 6, 2020, through April 21, 2020.
Participants
Intervention group
The intervention was offered to all patients who met the inclusion criteria based on the RWJBH COVID-19 Assessment Protocol (Figure 1). Patients' consents to participate in the intervention were documented in the institutional medical record. The intervention enrolled 192 patients from the inpatient units (n = 114; 59.45%), the observation unit (n = 40; 20.8%) and the ED (n = 38;19.8%). Patients were enrolled at Saint Barnabas Medical Center (n = 107), Newark Beth Israel Medical Center (n = 29), Clara Maass Medical Centers (n = 26), and Jersey City Medical Center (n = 30). The intervention group included 117 (61%) male and 75 (39%) female participants and their ages ranged from 19 to 93 years (mean [M] = 57.44, standard deviation [SD] = 11.84). All patients presented with mild COVID-19-like symptoms and, depending on the availability of confirmatory testing, were identified as patients positive for COVID-19 or PUI patients. The majority of the PUI patients had clinical symptoms and radiologic findings that supported a diagnosis of COVID-19. Race, ethnicity and comorbidity data also were collected (Tables 1 and 2).
Demographics of Intervention Group (n = 192) and Comparison Group (n = 593) Participants
Top 10 Comorbidities of Intervention Group (n = 192) and Comparison Group (n = 593) Participants
Comparison group
A total of 7141 patients positive for COVID-19 were admitted to the entire RWJBH system from March 1, 2020 through May 9, 2020. During this period, a total of 3619 patients were admitted to the 4 hospitals that implemented the ITCM intervention. To identify a comparable comparison group, the authors initially included 1676 patients, aged ≥18 years, with a diagnosis of mild-to-moderate COVID-19, who were admitted urgently or emergently. In order to ensure a close match to the intervention group, the comparison group was then limited to include only patients with a principle diagnosis of COVID-19 acute respiratory disease (n = 888; 86%), other viral pneumonias (n = 101; 9.8%), and pneumonia, unspecified organism (n = 43; 4.2%), who were discharged home with self-care or discharged home with home care, bringing the comparison group to 1032 patients. The authors excluded patients with moderate COVID-19 who required intensive care during their stay, with or without mechanical ventilator support, bringing the comparison group to 593 patients. The comparison group also was matched to the intervention group by their top 10 comorbidities (Table 2).
Data analysis
ITCM intervention data were analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 26 (IBM, Armonk, NY). After data were entered into SPSS, descriptive statistics were calculated for all demographic data. In particular, means and standard deviations were calculated for all continuous demographic variables (age and length of stay), and frequencies and percentages were computed for all categorical demographic variables (sex, race, and ethnicity). Chi-square tests of independence were conducted to examine the relationship between the intervention and hospital re-encounters and readmissions. An independent samples t test was conducted to examine mean differences in length of stay between the intervention and the comparison groups.
Results
The intervention was offered to 201 patients, 192 (95.5%) of whom agreed to participate. Descriptive statistics for demographics and comorbidities for both the intervention and comparison groups are provided in Table 1 and 2, respectively.
Of 192 patients enrolled in the intervention, 38 were enrolled from the ED, 40 were enrolled from the observation unit, and 114 were enrolled from the inpatient units. Re-encounters with the health system, hospital readmissions, and lengths of stay were analyzed.
Thirty-eight patients in the ED were included in ITCM and discharged home. A total of 7.9% of these patients (n = 3) subsequently had a re-encounter in the observation unit within 6 to 20 days; however, no patients were admitted to the hospital within 30 days. In the intervention group, of 40 patients who were discharged home from the observation unit, a total of 10% (n = 4) subsequently had an ED (n = 1) or observation unit (n = 3) re-encounter within 5–17 days, and no patients were admitted to the hospital within 30 days. In the intervention group, of 114 patients who were discharged from an inpatient unit, a total of 14.9% (n = 17) subsequently had a re-encounter in the ED (n = 6) or an observation unit (n = 11) within 1–19 days, and only 3.5% (n = 4) were readmitted to the hospital within 30 days of index discharge. In the comparison group, of 593 inpatient discharges, a total of 28.2% patients (n = 167) subsequently had re-encounters in the ED (n = 28) or observation units (n = 139) within 1–30 days, and 4.4% patients (n = 26) were readmitted to the hospital within 30 days of index discharge. There were no mortalities within 30 days for both the intervention and comparison groups.
In the intervention group, the combined rate of additional hospital re-encounters with the health system (ED or observation unit visits) was 12.5% (n = 24) compared to 28.2% (n = 167) in the comparison group. A chi-square test of independence was conducted to examine whether differences in hospital re-encounters were observed between the intervention group and the comparison group. This difference was statistically significant (χ 2 = 19.3, P < 0.001).
In addition, a chi-square test of independence was conducted to examine whether differences in hospital readmissions were seen between the intervention and comparison groups. The readmission rate in the intervention group was 3.5% (n = 4) compared to 4.4% (n = 26) in the comparison group. This difference was not statistically significant (χ 2 = .18, P = 0.671).
Finally, an independent samples t test was conducted to examine the differences in the length of stay between the intervention and the comparison groups. This identified that patients in the intervention group had lower average length of stay (M = 4.61, SD = 5.8) than those in the comparison group (M = 6.80, SD = 4.67) (t(782) = -5.28, P < 0.001). Additionally, the mean length of stay for ITCM-enrolled patients who were discharged from the ED, observation and inpatient units was 0 days, 1.22 days (SD = 0.53) and 6.94 days (SD = 5.9) respectively.
Discussion
One of the hallmarks of the 2020 COVID-19 pandemic has been an acute shortage of inpatient medical and surgical hospital beds, resulting in overcrowded EDs and observation units. Furthermore, the COVID-19 pandemic stressed supply chains for the provision of home oxygen delivery and at-home oxygen saturation monitoring. Because of the highly contagious nature of the virus, there was an urgent need to shift clinical intervention in the outpatient setting from face-to-face visits to an expanded use of virtual visits via telemedicine and telenursing. A solution was proposed that included an assessment protocol for patients with COVID-19 to identify patients clinically appropriate for participation; provision of at-home oxygen supplementation therapy; and daily medical monitoring via telemedicine and telenursing.
Assuming that the total patient bed days saved related to implementation of this intervention was the difference in total length of stay between the comparison group and the ITCM ED and observation unit groups, the calculated savings is 481.6 patient days for the 78 participants who were enrolled in the intervention and discharged directly from the ED or from observation units (see Table 3).
Number of Hospital Inpatient Days Avoided
Difference between the intervention group and comparison group length of stay.
Subsequent readmissions for the intervention group, while very uncommon with 3.5% (n = 4) admitted during the intervention at an average of 8.25 days (range 4 to 11 days post inclusion in the intervention), were not significantly different than the 4.4% (n = 26) readmissions for the comparison group.
Overall, the data suggest that this intervention resulted in increasing bed capacity by reducing the number of patients with COVID-19 remaining in the ED, observation, and inpatient units.
The assessment of this intervention has certain limitations. The patient population is based on a convenience sample of patients who met the criteria as RWJBH System Hospitals approached the peak of this pandemic crisis. The sudden and emergent need to increase hospital bed capacity and reduce the number of patients with COVID-19 remaining in the ED and observation units were the impetus for developing this intervention as a performance improvement project rather than a formal research study. Similar to health systems around the country, RWJBH's health care providers were working extraordinary hours, making appropriate accommodations to serve the volume of patients, their health status, the severity of and need for continued urgent care, as well as finding space for patients when all beds became occupied. RJWBH health care providers recognized the need to identify another safe and rational approach so that patients needing intensive care could receive it quickly without displacing other patients in the hospitals. Under these dire circumstances, the health system's clinical leadership identified another process that would maintain standards of care, health system policies, and expand on current delivery of care (eg, home health care services, telemedicine). The patients for whom ITMC was an appropriate intervention were informed and provided consent to engage in the clinical intervention, which was documented in the electronic medical record. Changing the venue for the delivery of care was a quality improvement intervention, not research needing Institutional Review Board approval, driven by the need for severely ill patients to receive more timely intensive care. In the future, a randomized controlled trial will be necessary to validate these findings, something that was not feasible during the height of the pandemic.
A likely outcome of this pandemic will be greatly expanded telemedicine and telenursing services. The fundamentals of this intervention promote intensive daily telemedicine-based medical and nursing management and in-home clinical monitoring for a relatively short period of time. RWJBH is adapting the framework of this intervention beyond patients with COVID-19 for selected chronic conditions.
Conclusion
Never has it been more vital for the US health system to develop strategies for increasing hospital surge capacity and managing patient throughput than in the COVID-19 pandemic. The ITCM intervention demonstrated that it was a practical and effective process for improving throughput of patients with COVID-19 to optimize hospital bed capacity. Further studies will be required to refine patient eligibility, optimal intervention length, and specific components of telemedicine and telenursing. Lessons learned and best practices from ITCM will be applied to future transitions of care interventions.
Footnotes
Author Contributions
Irene Borgen, RN, MSN, MBA, MJ – participated in writing the paper, data analysis, both revisions and intervention implementation. Martha Romney, RN, BSN, MS, JD, MPH - participated in writing the paper, data analysis, and 1st revision. Nicole Redwood - participated in writing the paper, data collection, 1st revision, and intervention implementation. Belynda Delgado, RN, MSN - participated in writing the paper, data collection, 1st revision, and intervention implementation. Patricia Alea, RN, MSN- participated in writing the paper, data collection, 1st revision, and intervention implementation. Brian H. George, MS, MBA - participated in writing the paper, data collection, 1st revision, and intervention implementation. Jennifer Puzziferro, RN, DNP - participated in writing the paper, data collection, 1st revision, and intervention implementation. Lina Shihabuddin, MD – project conceptualization, team selection, participated in writing the paper, data analysis, revisions, and intervention implementation.
Acknowledgement
The authors would like to recognize Ms. Ellen Gusick, Chief Nursing Officer of Visiting Nurse Association Health Group, for her leadership of the home care aspects of this project.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.