
Abstract

A
Paradigm Shift
Traditionally, the health care system has worked downstream from the root causes of the adverse health condition. By waiting until a health issue presents itself, has the health care system missed an opportunity to intervene earlier (ie, outside its walls) in the disease progression? It is important to note that the health care system is not solely responsible for SDoH that contribute to poor health outcomes. However, providers are being asked to expand their work to act on SDoH to improve the health of the overall population as we adapt to a value-based health system. Health care providers have reported barriers to adopting an upstream and downstream approach (eg, lack of time, absence of pertinent compensation programs). 5 Nevertheless, many providers acknowledge that the work is important and they are but one link in a chain of stakeholders who should address this issue.
Health care systems often engage in social needs-informed care and social needs-targeted care, which have been described as approaches to respond to a population's health issues. These approaches are helpful but not sufficient on their own to address the underlying causes of poor health. Improving population health takes a team of community-based organizations, government, and private and public sectors to partner with the health care system, as well as policy interventions at the local, state, and national levels. 6 So, how can the health care system work to address not only the downstream factors it is accustomed to tackling but now the upstream factors – both of which are necessary to improve the health of the population?
The National Academies of Sciences, Engineering, and Medicine recommends that a paradigm shift is warranted because of the current evidence of the role that SDoH play in shaping a population's health landscape. Thus, to achieve more equitable population health outcomes, an integration of social care and health care is advised via an approach that uses activities focused on awareness, adjustment, assistance, alignment, and advocacy. Interprofessional teams, health information technology innovations, and new financial models will be required to establish and sustain the partnerships necessary to improve the population's health in this new era of health care. 7 In many communities, we are asking entities to work together that have not had a reason or incentive to collaborate despite offering services to the same population. We address this critical point by expanding Caron's work to illustrate the role for partnership building among the systems involved in coproducing health. 4
Current research presents the following key factors as drivers of coproduction: geography, innovation, mission and vision, governance, multisector partnerships, priority focus areas, data/measurement, and financing/sustainability (Figure 1). Additionally, we propose that a commitment to partnership principles (eg, community-based participatory research, Health in All Policies [HiAP], interprofessional integration) and value-based payment models (eg, Accountable Care Organizations [ACOs], Accountable Care Communities [ACCs], Patient-Centered Medical Homes, and Population Health Organizations [PHOs]) are needed to advance multisector partnerships. For example, ACCs integrate entities from diverse sectors, including behavioral health, public health, social services, and community-based supports, to meet patients' medical and social needs. The most common strategies to address SDoH involve screening and linking patients to community resources followed by maintaining social services databases, using value-based payment models to incentivize clinicians' behavior, using community health workers and/or interdisciplinary teams, and funding additional services such as housing or food-related supports. 8,9 Some states are examining ways to use risk adjustment to better account for “complex” patient populations.
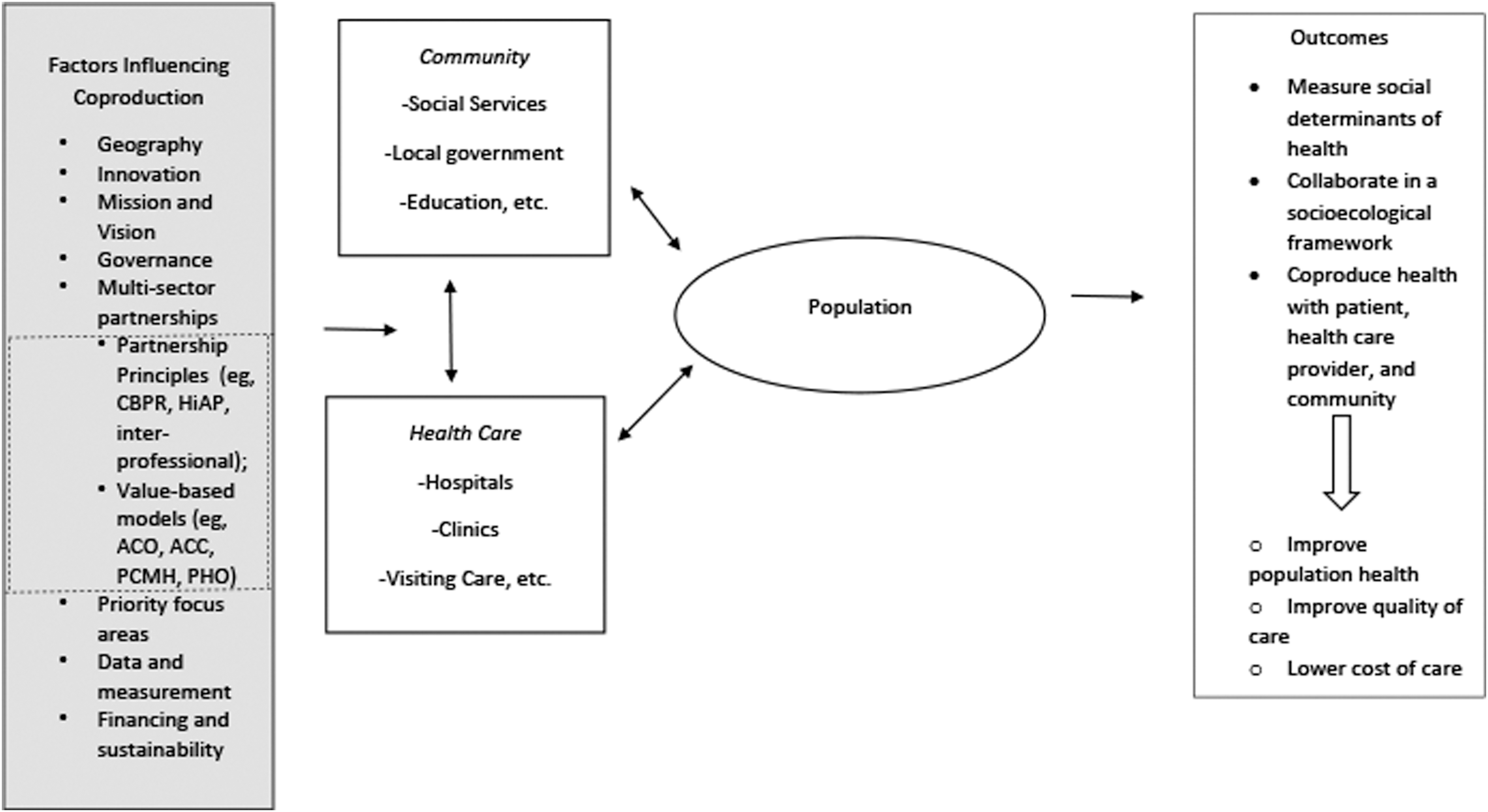
Coproduction of health concept broadened to indicate the importance of multisector partnerships in improving the population's health in a dynamic environment (adapted from Caron, 4 with permission).
Nationally, however, screening alone is unlikely to be enough. A recent study suggested that although approximately 88% of hospitals have implemented some type of screening to identify patients' health-related social needs, only 62% report screening target populations in a consistent way, and even fewer report using the data systematically to improve health outcomes. 8 This is problematic not only because additional time and effort are being taken away from patient care without being linked directly to quality improvement, but also because identifying acute needs (eg, housing concerns) without being able to address the root cause of the social problem (eg, housing markets, policies that hinder an adequate supply of affordable housing) may leave clinicians feeling ethically compromised and patients feeling even more frustrated. Furthermore, disparities in information technology infrastructure and limited data-sharing capacity pose barriers for many smaller or medium-sized organizations.
Thus, a balance of flexibility, innovation, and standardized measurement are critical for coproduction. For example, several State Innovation Models (SIMs) are testing ACC models to advance their goals and address the full range of SDoH. The SIM initiative, generated through the Center for Medicare and Medicaid Innovation, provides select states with financial and technical support to advance new service delivery models and multipayer health care payment reforms. SIM awardees are required to develop a population health plan that addresses health disparities, determinants of health, mental health, and substance misuse to integrate community health and prevention into their delivery system and payment models.
Despite the widespread adoption of ACO models, some scholars contend that cost shifting (eg, rewarding organizations for lowering costs for their ACO patients while simultaneously increasing costs in other parts of the system) has posed a barrier to ACO success. The concept of PHOs has been proposed to address these limitations by moving toward a more fully capitated model. This includes providing universal coverage (eg, offering patients a choice of PHOs in statewide insurance marketplaces), real-time data exchange, and more robust payment models that would enable market forces to reward entities that deliver better, less costly care. 10
Recommendations
We propose that, along with policy reforms in the health care sector, a renewed focus on HiAP would incentivize other sectors to consider health in diverse policy-making arenas and facilitate inclusion of health professionals in policy-making processes. Policies that could facilitate integration of SDoH include providing sustainable funding, implementing local and regional networking initiatives to facilitate partnership development, and developing standardized data on community-based organizations' services and quality to aid providers that seek partners. Providing training to ensure literacy with respect to partnership principals could enable interprofessional teams to function more effectively, accelerating transformative social learning as their coproduction efforts evolve.
Footnotes
Author Contribution Statement
The authors contributed to the development of this work, which builds upon prior work published by R.M. Caron. Both authors drafted and revised the intellectual content, and were involved in the final approval of the manuscript to be published. Both authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.