
Abstract
Little information has been compiled across studies about existing interventions to mitigate issues of medical financial hardship, despite growing interest in health care delivery. The purpose of this qualitative systematic scoping review was to examine content and outcomes of interventions to address medical financial hardship. PRISMA guidelines were applied to present results using PubMed, Scopus, and CINAHL, published between January 1980 and August 2020. Additional studies were identified through reference lists of selected papers. Included studies focused on mitigating medical financial hardship from out-of-pocket (OOP) health care expenses as an intervention strategy with at least 1 evaluation component. Screening 2412 articles identified 339 articles for full-text review, 12 of which met inclusion criteria. Variation was found regarding targets and outcome measurement of intervention. Primary outcomes were in the following categories: financial outcomes (eg, OOP expenses), behavioral outcomes, psychosocial, health care utilization, and health status. No included studies reported significant reduction in OOP expenses, perceptions of financial burden/toxicity, or health status. However, changes were observed for behavioral outcomes (adherence to treatment, patient needs addressed), some psychosocial outcomes (mental health symptoms, perceived support, patient satisfaction), and care utilization such as routine health care. No patterns were observed in the achievement of outcomes across studies based on intensity of intervention. Few rigorous studies exist in this emerging field, and studies have not shown consistent positive effects. Future research should focus on conceptual clarity of the intervention, align outcome measurement and achieve consensus around outcomes, and employ rigorous study designs, measurement, and outcome follow-up.
Introduction
Patients' affordability challenges with health care in the United States predate the Great Depression, with policy reforms thereafter attempting to address this pressing issue. 1,2 The problem has only grown since. Currently, 1 in 4 American families are experiencing financial burden related to medical care. 3 Affordability challenges are among the top 4 reasons patients across health conditions and disease types do not follow through with therapeutic recommendations. 4,5
Researchers use several terms to describe the financial hardship experienced by the patients/families as they navigate health care: financial toxicity, 6,7 economic/financial burden of disease, 8 cost-related nonadherence 9 /cost-related prescription delay, 10 medical financial hardship, 11 and financial stress/strain/distress. 12 These terms describe concepts that include how one feels about one's financial resources, and/or what one is doing in terms of a behavioral response as a result of one's economic circumstances. 13 Terms such as financial toxicity and medical financial hardship often encompass multiple domains of objective hardship, stress, and behavior.
As an example, among people with diabetes, 40% of families report medical financial hardship, resulting in high levels of distress, food insecurity, cost-related treatment nonadherence, and forgone/delayed care. 14,15 Cancer, as another example, is one of the most expensive conditions to treat in the United States because of parallel trends of increasing cost of cancer therapies, evolving treatment patterns, greater prevalence of high-deductible health plans, cost sharing, and underinsurance, and progressively increasing survival related to new therapies. 7 Families often make substantial financial and behavioral adjustments to their budget and expenses following a cancer diagnosis, which can have a negative impact on both the patient and other family members. 16 Financial distress from mounting financial obligations and debt and the erosion of wealth may interfere with the patient's ability to cope effectively with cancer, its physical symptoms, and its treatment, thereby adversely affecting health outcomes and potentially creating a vicious cycle of mounting expense. Failure to prevent and address this financial toxicity leads to poor treatment optimization, reduced quality of life, high symptom burden, and earlier mortality. 17,18 Similar investigations of hardship have been done for other diseases and treatment contexts as well, including Alzheimer's, cardiovascular disease, surgery, Crohn's disease, respiratory disease, and stroke. 19 –27
A growing number of interventions are being developed and tested in health care delivery to mitigate issues of medical financial hardship for patients. The need for such interventions is exacerbated by limited policy changes to address the rising costs of health care. The causes and effects of medical financial hardship are established, especially in oncology, 6,7,28 –32 but strategies to reduce its burden are less frequently discussed in the literature and systematically studied. There is currently a lack of knowledge about known effective or optimal targets or mechanisms for improving medical financial hardship. Despite increasing calls to intervene on medical financial hardship, 7,33 no systematic review of interventions has been published across studies about the types and impacts of existing interventions. The first step in establishing recommendations for strategies to reduce medical financial hardship requires understanding the current state of science on interventions. The purpose of this qualitative systematic scoping review was to examine the existing peer-reviewed literature on content and outcomes of interventions to address medical financial hardship. For this review, medical financial hardship is defined as encompassing either material, psychosocial, or behavioral domains.
Methods
Study design
This review utilized the 5-step scoping review method and the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework for reporting standards. PRISMA steps were followed, including (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; and (5) collating, summarizing and reporting results. Study findings from the scoping review were used to establish recommendations for interventions to address current gaps. This study was considered exempt by the Institutional Review Board.
Literature search strategies
A systematic search of the literature between January 1, 1980, and August 2020 was performed using several databases including PubMed, Scopus, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL). The search strategy included search queries with a Boolean combination of Medical Subject Heading (MeSH) terms (eg, medical financial burden, financial hardship, patient, intervention) customized for each literature database. Only English-language, full-text articles were selected for further review. The literature search was performed by trained research assistants in consultation with health sciences librarians, who together refined search queries, screened titles, and retrieved abstracts for potentially eligible studies. Additional studies were identified from reference lists of selected papers. Search results were imported into Mendeley Reference Manager (Mendeley Ltd, London, UK) for initial title and abstract assessment.
Eligibility criteria
Included publications tested interventions mitigating material, psychosocial, or adverse behavioral domains of medical financial hardship. Included studies had at least 1 evaluation component, including process or outcomes evaluation. Pilot studies were included, as well as studies with outcome evaluation without a control group or assignment to more than 1 treatment condition. Studies also had to be published between January 1, 1980, and August 2020, conducted in the United States and published in an English-language journal. Studies were excluded if they were literature reviews, non-empirical recommendation pieces such as an opinion or perspective, or if the full-text article was not available for review.
Data extraction and analysis
First, titles were reviewed for study eligibility to ensure that they described an intervention addressing medical financial hardship. When a title was insufficient to determine study eligibility, the abstracts were reviewed. Two authors (DB and NI) independently reviewed each article included to determine if it met all inclusion criteria. A protocol was used to resolve discrepancies or uncertainty about study inclusion. During the title and abstract screening, the independent reviewers erred toward inclusion. Data were extracted using a form that captured study design, sample and setting, intervention description, and outcomes.
Results
Figure 1 shows the PRISMA diagram describing the literature search and screening processes. Of the 2412 articles that resulted from the literature search, 339 were considered relevant based on the title and/or abstract. These articles were retrieved and reviewed for inclusion criteria. Of the 339 full articles reviewed, 12 articles representing 12 unique studies met the inclusion criteria.
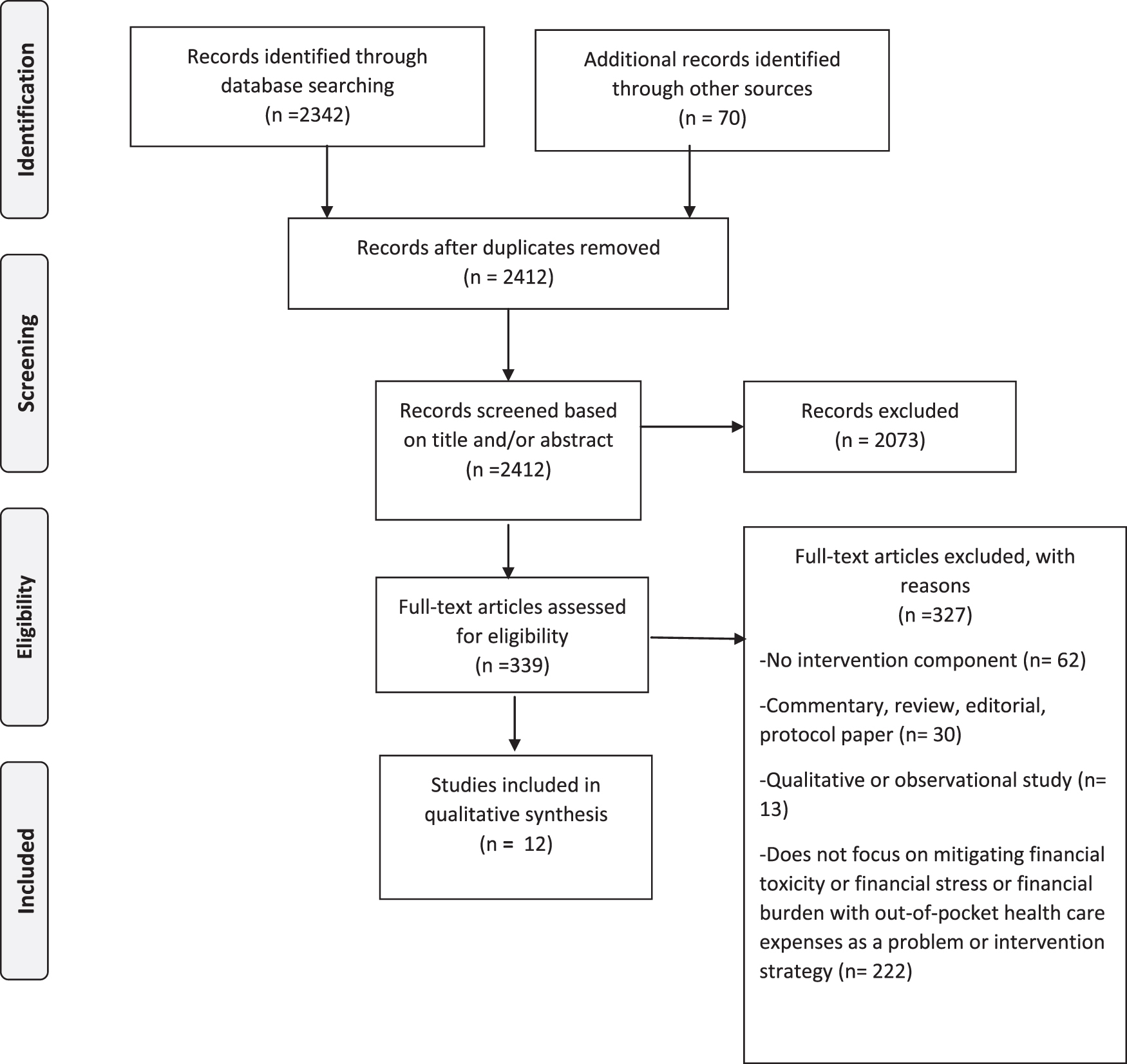
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study designs
Five studies used a randomized controlled trial design to evaluate outcomes, 34 –38 while 1 study used a quasi-experimental design. 39 The majority of studies utilized a pre–post evaluation design without a control group to examine changes in outcomes from their intervention. 40 –45
Program characteristics
Intervention models
Intervention approaches to address medical financial hardship varied by types of support and intensity (Table 1). Three studies tested out-of-pocket (OOP) payment elimination for treatment and/or health care services. 34,39,40 One study examined an intensive strategy of care management that included nurses and social workers who managed the care of patients with high health care costs. 36 Two studies provided information about assistance as their intervention. One study screened for medical financial hardship and unmet social risk factors in a sample with diabetes and provided resource options to meet each need. 41 Another study provided informational decision support for living donor kidney transplant recipients, supplemented with information about donor financial assistance for both medical and nonmedical expenses. 38 Four studies used patient and or/financial navigation as an intervention, where ongoing support sessions with trained personnel emphasized identifying and addressing barriers to treatment, including treatment costs and nonmedical social and economic needs. 35,42,44,45 Three studies used financial education as an intervention. 37,42,45 One study used a program for teaching financial management skills to parents of pediatric patients. 37 Two studies coupled financial skills training with financial counseling and financial navigation support. 42,45
Included Studies
MSW, master of social work; NA, not applicable; RN, registered nurse.
Five studies tested low-touch interventions, 34,38 –41 and 7 studies tested high-touch interventions. 35 –37,42 –45
Setting and target populations
Half of the studies included were conducted in academic medical centers, 39,37,41 –43,45 while 1 study was conducted in an integrated health system. 35 Three studies were conducted in community clinical settings, 38,40,44 and 2 studies were in nonclinical community settings. 34,36 Studies primarily focused on adults as the primary target of intervention, while 2 studies focused on the family/household. 34,37 Six studies focused on individuals with cancer, 39,42 –45 while other studies focused on populations with diabetes, 40,41 mental health, 36 anemia, 34 kidney disease, 38 chronic disability, 37 and general chronic care populations. 35,36
Target of medical financial hardship
Eleven out of 12 studies targeted OOP expenses related to patients' medical care as part of the intervention strategy. 34 –36,38 –45 One study focused exclusively on financial literacy. 37 Four studies focused on addressing OOP expenses related to direct treatment and co-payments only, 34 –36,40 while 7 studies targeted not only medical expenses, but also nonmedical needs such as transportation costs; support with utilities and food, among other items; logistics or expenses. 38–39,41 –45 Two studies targeted financial literacy, medical care expenses, and nonmedical social needs. 42 –45
Outcome measures
Primary outcomes measured in included studies were classified into the following categories: financial, behavioral, psychosocial, health care utilization, and health status (Table 2). Two studies measured financial outcomes, specifically OOP expenses of patients. 36,40 Three studies measured behavioral outcomes. One study measured adherence behaviors to the treatment plan, 41 1 study measured uptake of offered assistance, 38 and 2 studies measured financial management skills. 37 –41 The majority of studies addressed psychosocial outcomes. Six studies measured financial stress of participants, 39,41 –45 1 study measured mental health and social support, 44 1 study measured patient satisfaction, 35 and 1 study measured caregiver strain. 45 Finally, 2 studies measured disease outcomes, 34,40 and health care utilization. 34,36
Outcomes Measured Across Included Studies
Study findings
No patterns were observed in the achievement of desired outcomes between studies testing low-touch and high-touch interventions.
Financial outcomes
No included studies showed reduction in OOP expenses after the intervention. 36,40
Behavioral outcomes
There were consistent positive findings across studies demonstrating improvement in behavioral outcomes after intervention, specifically for adherence to the treatment regimen, 40,41 having their needs addressed or uptake of offered assistance, 39,44 and financial skills/management behavior. 37,41
Psychosocial outcomes
After intervention, included studies showed improvements in perceived social support, 44 improved patient satisfaction, 35 and improved mental health symptoms. 42,44 There were consistent findings across studies showing no changes in perceptions of financial burden/toxicity, 39,41 –43,45 and no change in caregiver strain 45 after the intervention.
Health care utilization outcomes
Findings were consistent across studies around health care utilization. Both studies that measured health care utilization as a primary outcome showed increased use of desired forms of health care, specifically primary care use, and outpatient mental health service use after the intervention. 34,36
Health status outcomes
No included studies showed changes in health status after the intervention. 34,40
Discussion
This qualitative systematic scoping review is the first to the authors' knowledge to report on the content and outcomes of interventions to mitigate medical financial hardship. This review was undertaken in order to inform future interventions and research to reduce medical financial hardship. A total of 339 articles were assessed, which yielded only 12 articles that evaluated an intervention to address medical financial hardship, identifying little consensus on effective, evidence-based approaches. Not all included an appropriate control condition, further diminishing current knowledge.
Variation was found across studies regarding both strategy and intervention targets and outcome measurement. Included interventions were designed to reduce medical care expenses and co-payments, and improve financial literacy, nonmedical social needs, and care logistics – either exclusively or in combination. This variation reflects conceptual heterogeneity around what encompasses medical financial hardship. Within some frameworks, and at the health policy level, medical financial hardship is often discussed in the context of health insurance, objective OOP expenses, and income loss constituting burden. 28 Tucker-Seeley and Thorpe have proposed a material-psychosocial-behavioral model of medical financial hardship that considers a broader definition of hardship encompassing nonmedical social needs, as well as financial literacy in the “material” domain, and financial stress in the psychosocial domain. 13 No included studies were guided by a theoretical or conceptual framework specific to medical financial hardship, complicating how intervention targets lead to improvement in chosen outcomes, and thus limiting their impact.
No included studies reported significant reduction in OOP expenses, perceptions of financial burden/toxicity, or health status. However, changes were observed in behavioral outcomes (adherence to treatment regimen, perception that patient needs were addressed), some psychosocial outcomes (mental health symptoms, perceived support, patient satisfaction), and health care utilization such as greater use of desired forms of routine health care. Although included studies demonstrated a mix of low-touch and high-touch interventions to address medical financial hardship, no patterns were observed in the achievement of outcomes across studies based on intensity of intervention. All included studies lacked conceptual clarity regarding hypothesized mechanisms to outcomes. No included studies had long-term follow-up in assessing outcomes. Long-term follow-up may be needed to demonstrate significant changes in objective financial burden, such as OOP expenses from a medical financial hardship intervention. Poor measurement validity also may explain consistent null findings with changes in perception of financial burden/toxicity. There are few measures for financial toxicity or perceptions of medical financial hardship, and existing measures have not been widely validated across different populations. 46,47 Notably, some studies did demonstrate significant changes when measuring mental health symptoms with validated instruments specific to mental health. Finally, perhaps intervening on OOP expenses and perceptions of financial burden/toxicity (eg, subjective experience) requires a stronger theoretical approach than evident in included studies.
Certain limitations to this review should be noted. Studies published between the initial search and publication of this article will not be included. Efforts to implement and evaluate medical financial hardship interventions and to identify best practices are not limited to academic institutions and may be undertaken by health care and nonprofit organizations without peer-reviewed publication; these may be underrepresented in the academic published literature. Finally, studies examining medical financial hardship interventions were excluded if they did not describe any evaluation components of the intervention. These intervention studies may nonetheless provide more indirect insights about addressing medical financial hardship and should be considered alongside the findings from this review.
Despite these limitations, this scoping review provides useful insights into future directions.
Overall, research on mitigating medical financial hardship requires conceptual clarity and greater use of behavior change theory to inform interventions. 48 There are various definitions of medical financial hardship and financial toxicity, each of which have several potential mechanistic pathways that could be targeted with interventions. This level of ambiguity makes studies that clearly conceptualize a mechanistic model, and test those mechanisms directly, key to moving knowledge forward. Along these lines, consensus on appropriate outcomes also will be critical to move knowledge forward.
Future research should focus on (1) conceptual clarity of the intervention, (2) align outcome measurement and achieve consensus around outcomes, (3) employ rigorous study designs, measurement, and outcome follow-up, and (4) attention to implementation of evidence-based approaches.
Lastly, intervention focus on multiple conceptual components of medical financial hardship (material, psychosocial, behavioral) versus a singular focus may lead to more robust changes in desired outcomes.
Conclusion
This review synthesizes the peer-reviewed literature on content and outcomes of interventions to address medical financial hardship. To date, very few rigorous studies have been generated in this emerging field. This review found variation across studies regarding targets and outcome measurement of intervention, and the studies yielded mixed findings. Future research should focus on conceptual clarity of the intervention, align outcome measurement, and employ more rigorous study designs, measurement, and outcome follow-up.
Footnotes
Authors' Contributions
Dr. Patel: conception or design of the work; acquisition, analysis, and interpretation of data; drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Jagsi: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Resnicow: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Smith: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Hammel: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Su: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Dr. Griggs: drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Ms. Buchanan: analysis and interpretation of data; drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Ms. Isaacson: analysis and interpretation of data; drafting the work, revising it critically for important intellectual content; final approval of the version to be published. Ms. Torby: analysis and interpretation of data; drafting the work, revising it critically for important intellectual content; final approval of the version to be published.
Author Disclosure Statement
Dr. Jagsi has no relevant conflicts. Outside the submitted work, Dr. Jagsi has stock options as compensation for her advisory board role in Equity Quotient, a company that evaluates culture in health care companies; she has received personal fees from Amgen and Vizient and grants for unrelated work from the National Institutes of Health, the Doris Duke Foundation, the Greenwall Foundation, the Komen Foundation, and Blue Cross Blue Shield of Michigan for the Michigan Radiation Oncology Quality Consortium. She has a contract with Genentech to investigate financial toxicity experiences of breast cancer patients. She has served as an expert witness for Sherinian and Hasso and Dressman Benzinger LaVelle. She is an uncompensated founding member of TIME'S UP Healthcare and a member of the Board of Directors of ASCO.
The coauthors declare that there are no conflicts of interest.
Funding Information
This work was supported by 5R01DK116715-03-Patel and the Michigan Center for Diabetes and Translational Research (P30DK092926) from the National Institute of Diabetes and Digestive and Kidney Diseases, and the Rogel Cancer Center (P30CA046592) from the National Cancer Institute.