
Abstract
This study aimed to comprehensively evaluate whether income affects long-term health outcomes for older patients who underwent percutaneous coronary intervention (PCI) provided by a universal health coverage system. Data were from the Latter Stage Elderly Healthcare Insurance database in Fukuoka Prefecture, Japan. A total of 5625 individuals aged ≥65 years who underwent PCI in 2014–2016 were included. Cox proportional hazards models were used to assess the association between income status and the incidence of health outcomes. With a median follow-up of 1095 days, 554 acute myocardial infarction (AMI) cases, 1075 stroke cases, 1690 repeat revascularization cases, and 1094 deaths were observed. Risk of all-cause mortality decreased significantly with increasing income level in both unadjusted and adjusted Cox regression models. Patients in the low-income level had a significantly higher rate of AMI (log-rank P = 0.003), stroke (log-rank P = 0.039), and all-cause mortality (log-rank P = 0.001) compared with patients in the high-income level. Observed rates for repeat revascularization also were high in the first year after PCI. In the Japanese universal health setting, low-income patients had a comparatively higher mortality risk after PCI. Poor long-term outcomes might be attributed to patients' baseline characteristics rather than treatment processes.
Introduction
Percutaneous coronary intervention (PCI) is one of the most effective methods for treating coronary artery diseases in an aging society, 1 and the use of PCI is increasing worldwide. 2,3 PCI is used widely in Japan. It is estimated that more than 200,000 PCI procedures are performed annually in Japan, 4 and the proportion of older people who undergo PCI has increased over the past decade. 5 Patients with PCI are at high risk of myocardial infarction, stroke, and repeat revascularizations. 6 To minimize the risk of these complications, long-term postoperative care must be provided.
Low income was reported to be associated with higher mortality and poorer quality of life after PCI. 7,8 However, the impact of income on long-term survival outcomes for older adults after PCI has seldom been evaluated. A large cohort study in England found an increased mortality rate after PCI in the lowest socioeconomic status patients compared with the highest socioeconomic status patients. 9 Although issues related to health care inequity among patients by income status was unheard of under the universal health insurance coverage in Japan, many studies have demonstrated that patients' postoperative outcomes and quality of life after cardiovascular-related surgery, including PCI, varied substantially among the populations with different income levels. 10,11 One possible reason is that sufficient postoperative management might not be provided. Although Japanese universal health insurance set a limit on what patients pay out of pocket for expensive medical care, 12 such as the cost for PCI, the cost for long-term postoperative care following hospital discharge is still a huge burden for patients with low-income status. 5
Understanding the relationship between income status and clinical outcomes in patients with PCI is important for addressing health care allocation inequality and for increasing access to quality care. Therefore, this retrospective cohort study was conducted that involves older patients with PCI status and uses an insurance claims database in Japan—a country that provides universal health coverage to older adults. This study aimed to clarify whether income has an impact on PCI patients' long-term outcomes after discharge from the hospital.
Methods
Study design and data source
This study was designed as a retrospective cohort study. Data were obtained from the Latter Stage Elderly Healthcare Insurance database of Fukuoka Prefecture with permission from the local government. Latter Stage Elderly Healthcare Insurance is an insurance plan designed specifically for residents aged ≥75 years and for residents aged between 65–74 years who have a specified disability. Each individual's identification number, sex, birth date, income level, diagnostic information, and treatment procedures are available in the claims database. Records were extracted for 5 fiscal years (ie, April 1, 2014, until March 31, 2019). A total of 5666 individuals who were discharged from the hospital between April 1, 2014, and March 31, 2016 were identified. Follow-up covered a 3-year period, starting from the date of hospital discharge.
International Classification of Diseases Tenth Revision (ICD-10) codes were used to capture patients' comorbidity status. Charlson comorbidity index (CCI) was used to measure severity of comorbidity status. To assess the potential impact on treatment prognosis and mortality, weights for CCI scores ranging from 1 to 6 were assigned. CCI scores for each patient were calculated by adding the weights of all comorbidities. 13 A previous study indicated that dementia and acute myocardial infarction (AMI) had a significant impact on the survival of patients who underwent PCI. 14 Therefore, the present study also extracted the history of dementia and AMI status from the database separately. ICD-10 codes for dementia were adapted from the work of Chartier et al (F00–F04, F05.1, F10.7, F12.7, G30, G31.0, and G31.1). 15 The ICD-10 code for myocardial infarction was defined as I21, and the type of diagnosis procedure combination (DPC) from the claims data was used to distinguish patients' acute conditions because the DPC is a Japanese mixed classification that is used by almost all acute care hospitals.
The claims database was used to identify the use of antiplatelet medications, which included clopidogrel, prasugrel, ticlopidine, beraprost, cilostazol, and aspirin. The database also was used to identify the use of commonly prescribed medications for post-PCI patients, including statins, β-blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, nitrates, warfarin, proton pump inhibitors, and H2 blockers.
Patients without income records were excluded from the study. A total of 5625 patients were identified as study subjects. The selection and exclusion processes are presented in Figure 1. The databases that were used to obtain study data were computer administered. Based on the Japanese government report, the insurance databases must have had a high penetration rate of up to approximately 98.6% until April 2015. 16 The Institutional Review Board of Kyushu University (Clinical Bioethics Committee of the Graduate School of Medical Sciences, Kyushu University) approved this study. Because anonymized claims insurance data were used, there was no requirement to obtain informed consent.
Flowchart of subject identification and inclusion and exclusion criteria details. PCI, percutaneous coronary intervention.
Patients' characteristics
This study assessed information on sex, age, income level, comorbidities, and CCI. Age was categorized into the following 4 groups: 65–74 years, 75–79 years, 80–84 years, and ≥85 years. The insurance database records income levels for the older population as low, middle, and high. Therefore, in this study, income levels were classified into low-, middle-, and high-income levels. These categories are applied by insurance associations operated in all prefectures in Japan. Such categories also correspond to the threshold set by the Japanese Ministry of Health, Labour and Welfare based on annual income: low-level, <1,550,000 yen ($13,868.5); middle-level, 1,550,000—3,830,000 yen (($13,868.5—34,268.7); high-level, >3,830,000 yen ($34,268.7). CCI scores were applied to define severity of comorbid conditions as mild (CCI = 0–1), moderate (CCI = 2–3), or severe (CCI ≥4).
End points
The end points of this study were 3 major adverse cardiac events and 3-year all-cause mortality. This study defined major clinical events as AMI, stroke, and repeat revascularization. Therefore, these 4 outcomes (AMI, stroke, repeat revascularization, and death for any cause) were analyzed separately. Repeat revascularization was defined as an event during which a PCI patient received subsequent procedures of PCI or coronary artery bypass grafting (CABG) after being discharged from hospital. Patients were censored at the time of death or at the end of the 3-year follow-up period. Information on these outcomes, including the dates of these outcomes, were extracted from the insurance claims database.
Statistical analysis
Baseline patient characteristics, medications, and clinical outcomes were compared among different income levels using one-way analysis of variance for continuous variables and Pearson's chi-square test for categorical variables. Cox proportional hazards models were used to compute crude and adjusted hazard ratios (AHRs) and 95% confidence intervals (CIs) for the end points to estimate the association between income levels and each outcome. In the adjusted Cox regression models, sex, age group, income level, CCI scores, AMI status, dementia status, and number of medications were adjusted covariates. Proportional hazards assumptions were checked based on Schoenfeld residuals. Cumulative event rates for each outcome were calculated by means of the Kaplan-Meier method. Log-rank tests were performed to assess the significance of income levels for each observed event time. All reported P values were 2-tailed, and the level of significance was set at P < 0.05. All statistical analyses for this study were performed using Stata Statistical Software: Release 15 (StataCorp LLC, College Station, TX, USA).
Results
Descriptive analysis
The study includes 5625 patients who previously had PCI. Table 1 shows the characteristics of the patients, 1960 (34.8%) of whom were at the low-income level, 3201 (56.9%) at the middle-income level, and 464 (8.2%) at the high-income level. Compared with males, more females were in the low-income level group. Patients between ages 75–79 had higher income levels compared with patients in other age groups. Patients with low-income status had a higher proportion of high CCI scores compared with the other patients. Patients with AMI were not significantly different among the different income levels, while patients with dementia showed a significant difference among the income levels.
Baseline Characteristics of Patients Undergoing Percutaneous Coronary Intervention, by Income
AMI, acute myocardial infarction; CCI, Charlson comorbidity index.
Regarding medications, clopidogrel was the most frequently prescribed antiplatelet drug (Table 2). There also was frequent use of aspirin, nitrates, proton pump inhibitors, and statins. Statins were prescribed more often among patients in the high-income level, while clopidogrel, proton pump inhibitors, and H2 blockers were prescribed more often among patients in the low- and middle-income levels. Median follow-up time was 1095 days. During follow-up, 554 (9.8%) MI, 1075 (19.1%) stroke, 1690 (30.0%) repeat revascularization, and 1094 (19.4%) death events were observed. Proportions of AMI, stroke, and death cases were significantly higher among low-income patients.
Medications and Health Outcomes, by Income
Total number of other medications (excluding antiplatelet and aspirin) was measured at the time of discharge. The number of total medications was selected to be a covariate in the Cox proportional hazard models. Patients received subsequent performance of percutaneous coronary intervention or coronary artery bypass grafting.
ACE-I, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; AMI, acute myocardial infarction; IQR, interquartile range.
Clinical outcomes
Table 3 shows hazard ratios for AMI, stroke, repeat revascularization, and death from any cause by income level. Risks of AMI and stroke decreased significantly in middle-income-level patients. Risk of AMI was similar even after the estimate was adjusted for sex, age, CCI scores, AMI status, dementia status, and number of medications. Risk of all-cause mortality decreased significantly with increasing income level in both unadjusted and adjusted Cox regression model (middle: AHR 0.83, 95% CI 0.73–0.95, P = .005; high: AHR 0.65, 95% CI 0.50–0.84, P = .001) (Table 3, Figure 2). The Kaplan-Meier curves for outcomes that compare cumulative rates of patients by different income levels are presented in Figure 3. The Kaplan-Meier estimates showed that patients in the low-income level had a significantly higher AMI rate (log-rank P = 0.003), stroke rate (log-rank P = 0.039), and long-term mortality rate (log-rank P = 0.001) compared with patients in the high-income level.
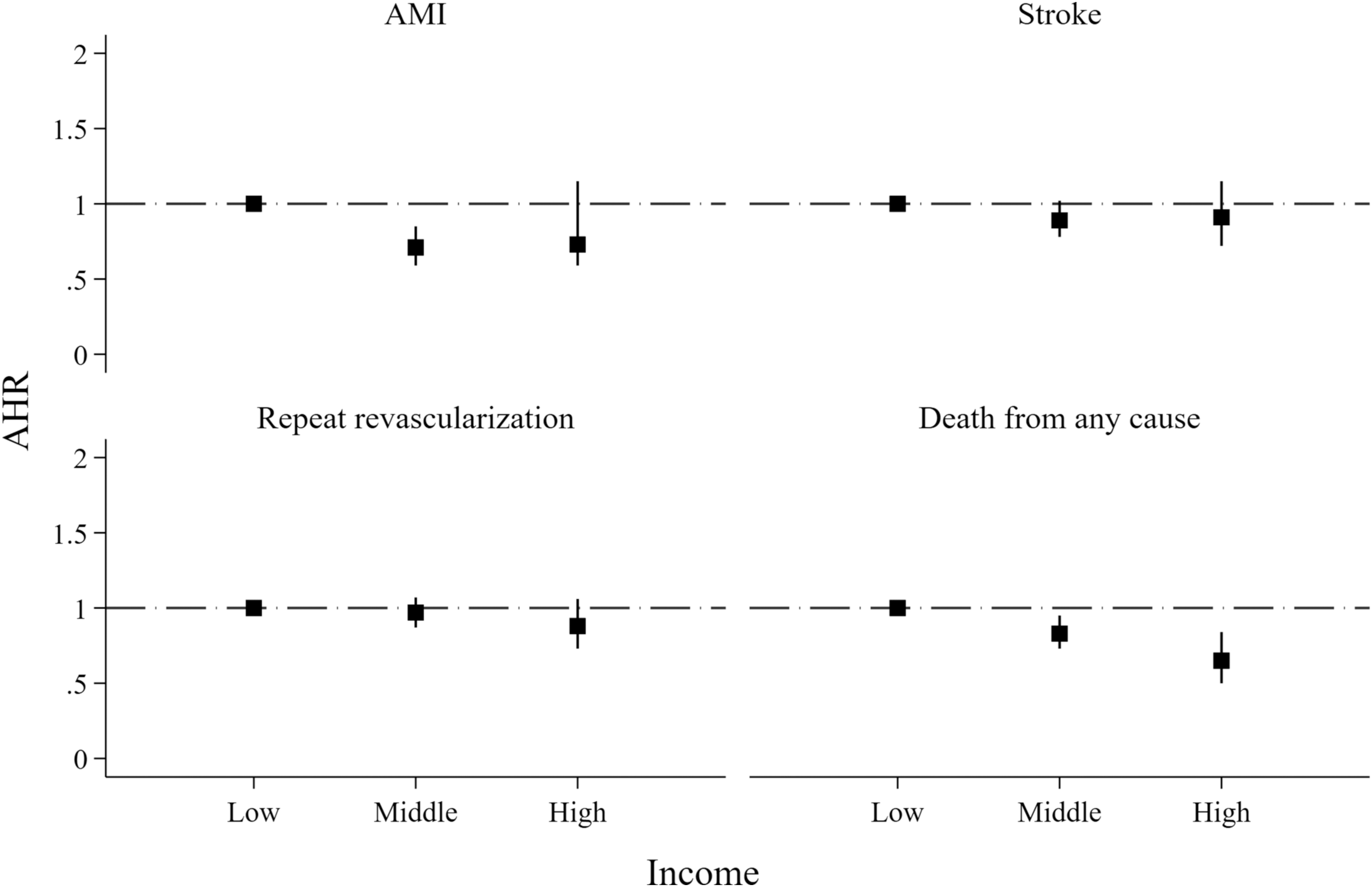
Adjusted hazard ratios among different income levels for AMI rehospitalization, stroke, revascularization, and death from any cause. Covariables in the models include age, sex, Charlson comorbidity index scores, history of AMI, history of dementia, and numbers of medications. AHR, adjusted hazard ratio; AMI, acute myocardial infarction.
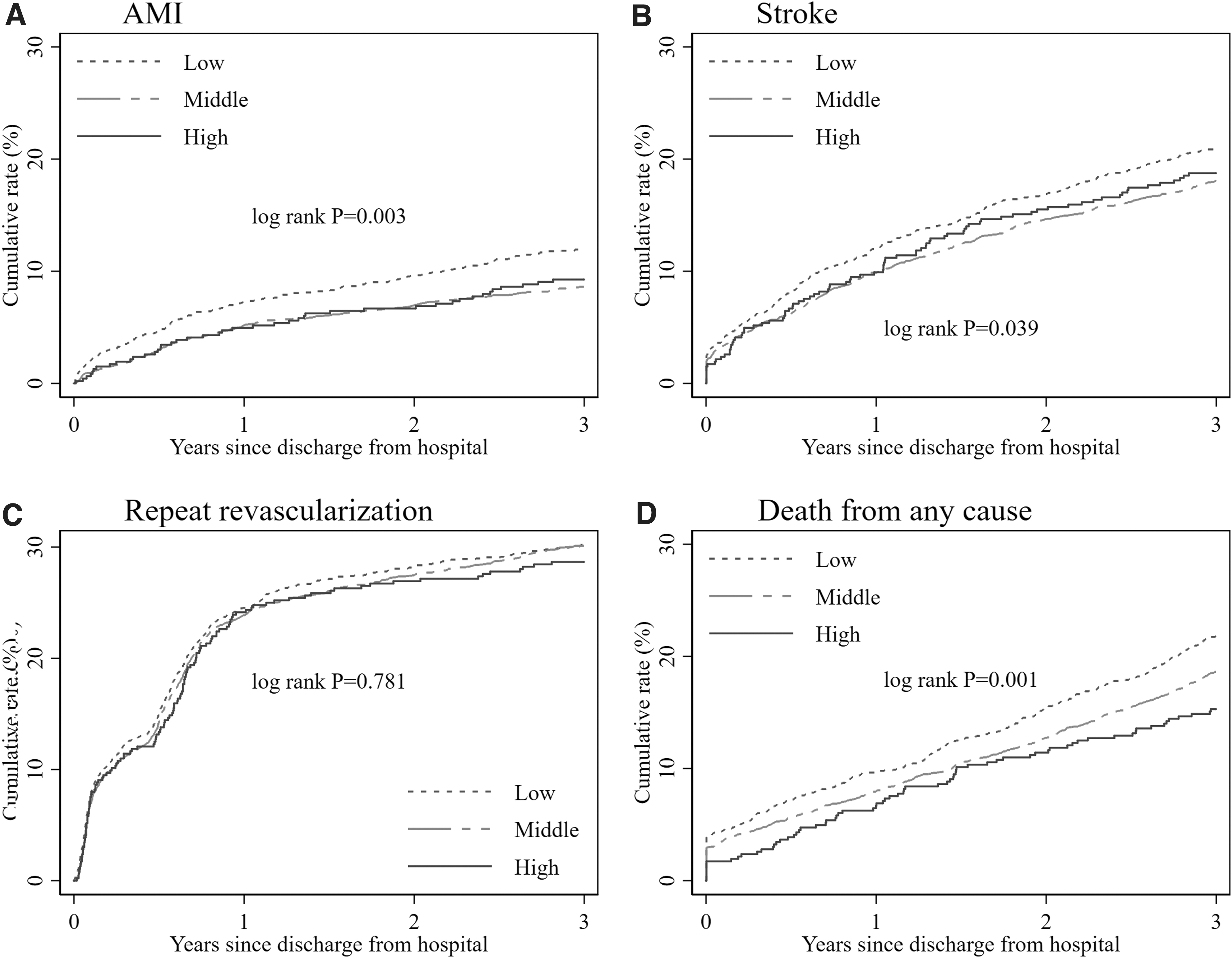
Kaplan-Meier curves among different income levels for AMI
Crude and Adjusted Hazard Ratios for Acute Myocardial Infarction, Stroke, Revascularization, and Death, by Income
AHRs were estimated by Cox proportional hazard models. Covariables in the models include sex, age, Charlson comorbidity index scores, history of AMI, history of dementia, and numbers of medications.
AHR, adjusted hazard ratio; AMI, acute myocardial infarction; CI, confidence interval; HR, hazard ratio.
Discussion
This retrospective cohort study comprehensively evaluated the association between income levels and clinical outcomes among older patients who underwent PCI in the setting of universal health coverage in Japan. This study found that patients with a high-income level were less likely to have a mortality risk compared with patients with a low-income level in both unadjusted and adjusted analyses (AHR: 0.65). There was a progressive increase in the cumulative rates of death from any cause from the high- to low-income level. Significant effects were not observed for the risk of AMI, stroke, and repeat revascularization among different income levels.
This is the first study to investigate the effect of income status on clinical outcomes after PCI in Japan. A number of studies conducted in western countries showed that a lower income level is associated with a higher all-cause mortality rate following PCI. 7 –9,17,18 The present study is consistent with and extends the findings of previous studies in the setting of a universal health coverage in Japan. A study involving 1346 PCI patients reported that low-income patients who were treated with PCI have more readmission events than high-income patients. 7 A study involving 13,770 patients who were undergoing PCI reported that the all-cause mortality rate was significantly higher in patients in the lowest quintile socioeconomic status than the highest quintile during a median follow-up of 3.7 years. 9 However, these studies were focused on valuating a specific adverse event after PCI. The present study concurrently evaluated a number of major adverse cardiac events (AMI, stroke, and repeat revascularization) and death from any cause. This study found that low-income patients faced a higher risk of all-cause mortality rather than other adverse cardiac events. By assessing these major clinical outcomes, this study ascertained the presence of disparities in outcomes among patients with different income status in Japan.
Some previous studies demonstrated several possible reasons why income level might influence PCI patients' long-term mortality rates. One possible reason might be social inequalities in the long-term management of chronic diseases among patients with different income levels. 8,9 Some evidence demonstrated that the measures for long-term management of chronic diseases, including post-PCI medication compliance and cardiac rehabilitation, are reduced in patients with a lower income level, 19,20 which might contribute to increased long-term mortality for these patients. 21,22 Despite some consistency with previous studies, the present study failed to observe a significant difference in any outcome of AMI, stroke, and repeat revascularization among patients with different income status. To the best of the authors' knowledge, this could be explained by the provision of universal health coverage in Japan. Because most out-of-pocket expenses could be subsidized by the government under this scheme, 12 it is possible to have identical medical treatment processes and clinical outcomes for all patients with different economic status. Another possible reason might be different lifestyle and dietary habits among patients with different income levels. 9,23 A previous study reported that patients with low-income status had a considerably worse diet and a lower quality of life, 7 which also might contribute to increased morbidity and mortality. A past study of 5622 PCI patients reported that low-income patients with PCI had a worse prognosis than high-income patients during a mean follow-up of 3.7 years, 8 and that the poor outcomes could be explained by differences in patients' baseline characteristics rather than treatment procedures. Therefore, in a universal health coverage setting, patients with different income levels have equitable access to health care services. Thus, the higher mortality rate is related to patients' characteristics rather than the treatment process.
In addition, despite a previous study concluding that lower economic status was associated with higher rates of repeat PCI and CABG, 9 the present study did not observe a significant difference in the outcome of repeat revascularization among patients with different income levels. The reason might be that the universal health coverage insurance system in Japan ensures that all patients receive access to medical treatment with affordable out-of-pocket expenses. 12 Nevertheless, it was observed that repeat revascularization rates in the first year after PCI were comparatively high in older patients, which is consistent with some previous clinical studies. 24,25 Thus, in the setting of universal health coverage, long-term secondary medical prevention of restenosis seemed necessary. 24
These findings have some important implications. To improve the quality of care for older adults who are undergoing PCI, it is important for post-PCI patients to have proper secondary prevention strategies and a healthy lifestyle, which might be substantially influenced by their economic status. 9,26 Policies to address poor post-PCI prognosis issues for older adults must cover secondary community prevention programs. To provide an environment that supports high quality of life, Japan is currently structuring a nationwide program called the Community-based Integrated Care System (CICS). Municipal governments are required to facilitate the construction of this CICS through collaborations with health care, nursing care providers, health promotion, and public health practitioners. 27,28 In order for this system to succeed, it is necessary to identify older people with low incomes and those with high mortality risk. 8,29 Identification of these vulnerable populations in the CICS system is useful in providing intensified secondary prevention and promoting a healthy lifestyle. 30
This study also has some limitations. First, the insurance claims data used were not specifically designed for clinical research purposes. Data analyzed did not provide information on disease severity, adherence to preventative therapies, or cardiac rehabilitation services. Researchers should explore these health care interventions, such as cardiac rehabilitation, to overcome the limitations faced by the current study. To compensate for this limitation, the current study provided information regarding medications prescribed after discharge and used the total number of other medications except antiplatelet drugs as a covariate. Second, the database does not contain information on living conditions. After discharge from the hospital, patients might choose to either go back home or to other health care facilities for recuperation. Patients who returned home may live alone or together with family. Third, by performing a power log-rank test to examine whether the sample had sufficient size power to detect the significance of the finding for all-cause mortality as one of the study outcomes, it was found that the number of samples in the high-income group (n = 464) is smaller than the sample size needed in each group. Therefore, study estimates might be statistically less accurate. Furthermore, there is a possibility of coding errors in the database. Upon inspection, it also was observed that a number of records for income status were missing. However, such an issue represents <1% of the total observation; therefore, the authors believe that it had little influence on the statistical inferences.
Despite these limitations, there are some strengths to this study. The main strength is the assurance of wide population coverage and a large sample size. The insurance claim database covered more than 600,000 insured people in Fukuoka Prefecture, and the penetration rate was as high as 98.6%, which was cited in some previous studies that used a similar insurance database. 16 Based on the wide population coverage, the insurance database provides complete information regarding patient-level characteristics, use of medications, and complete follow-up, which could minimize the risk of selection bias.
Conclusions
This study indicates that low-income patients faced a worse survival outcome after PCI even under universal health coverage in Japan. This association persisted despite adjustment by sex. The poor long-term survival outcome seems to be explained by patients' characteristics rather than the acute treatment processes. Intensified secondary prevention of restenosis and healthy lifestyle promotion in the CICS for older patients, especially those with a lower income status, could provide a promising solution to address this health inequality.
Footnotes
Authors' Contributions
Mr. Li conceived the design, acquired the data, performed statistical analysis, and drafted the manuscript. Dr. Babazono supervised the design and interpreted the results. Mr. Jamal performed the analysis and interpreted the results. Drs. Ohmori and Yoshida provided input from the clinical perspective. Ms. Kim, Dr. Fujita, and Ms Liu assisted with acquiring the data and revised the manuscript critically.
Acknowledgments
The authors thank the Wide-area Association of Latter Stage Elderly Healthcare of Fukuoka Prefecture for their provision of a health care claims database. We thank Jodi Smith, PhD, from Edanz Group for editing a draft of this manuscript.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.