
Abstract
Recent national statistics show that an estimated 11.2 million American adults live with serious, chronic forms of mental illness. The burden of mental illness is considerable for these individuals, their families, and communities. Effective medical treatment for serious mental illness (SMI) requires a patient-centered approach that engages patients in shared decision-making and supports the therapeutic alliance. Information regarding medication-taking behavior is essential for making treatment decisions, particularly in the instance of suboptimal therapeutic response. However, the evidence suggests that the probability of nonconformity with prescribed medication is elevated for individuals with SMI and that clinicians often overestimate their patients' adherence to medication-taking behaviors. In patients with SMI, unidentified problems with adherence may lead to unnecessary changes in treatment regimen and increased rates of hospitalization. Although various approaches have been used to assess medication ingestion with greater accuracy, none are without limitation. The growing field of digital medicine has introduced tools that engage patients for clinical purposes, gather and organize clinical data, and help measure care quality. Physician surveys show an appreciable increase in physician adoption of digital clinical tools, and studies suggest that a significant population of patients with SMI own and are comfortable using digital devices and tools. Digital tools designed to help people with SMI have the potential to transform the support and care available to people with mental health disorders, bridging a technology gap in mental health services.
Prevalence of Serious Mental Illness and Its Burden on Patients, Families, and Communities
Mental illnesses are surprisingly common conditions in the United States. National statistics show that nearly 1 in 5 American adults lives with a mental illness (51.5 million Americans aged 18 years or older were living with a mental illness in 2019). 1 The term mental illness is used to define a broad range of conditions that vary in degree of severity. 1 Two general categories are used to describe these conditions. The first, any mental illness (AMI), describes the broad range of mental, behavioral, or emotional disorders that can vary in impact—from no impairment to mild, moderate, and even severe impairment. 1 The second, serious mental illness (SMI), describes a smaller and more severe subset of AMI wherein the disorders result in serious functional impairment that substantially interferes with or limits 1 or more major life activities. 1 The burden of mental illnesses is particularly concentrated among those who experience disability because of SMI. 1 Chronic SMIs include conditions such as schizophrenia (SZ), bipolar I disorder (BP-I), and major depressive disorder (MDD).
In 2019, an estimated 13.1 million adults (aged 18 years or older) in the US had an SMI, a figure representing 5.2% of all US adults. 1 The prevalence of SMI was higher among women (6.5%) than men (3.9%); and young adults (aged 18–25 years) had the highest prevalence of SMI (8.6%) compared to adults aged 26–49 years (6.8%) and aged 50 years and older (2.9%). 1 In terms of racial distribution, the prevalence of SMI was highest among adults reporting 2 or more races (9.3%) and lowest among Native Hawaiian/Other Pacific Islander adults (2.6%) (Figure 1). 1
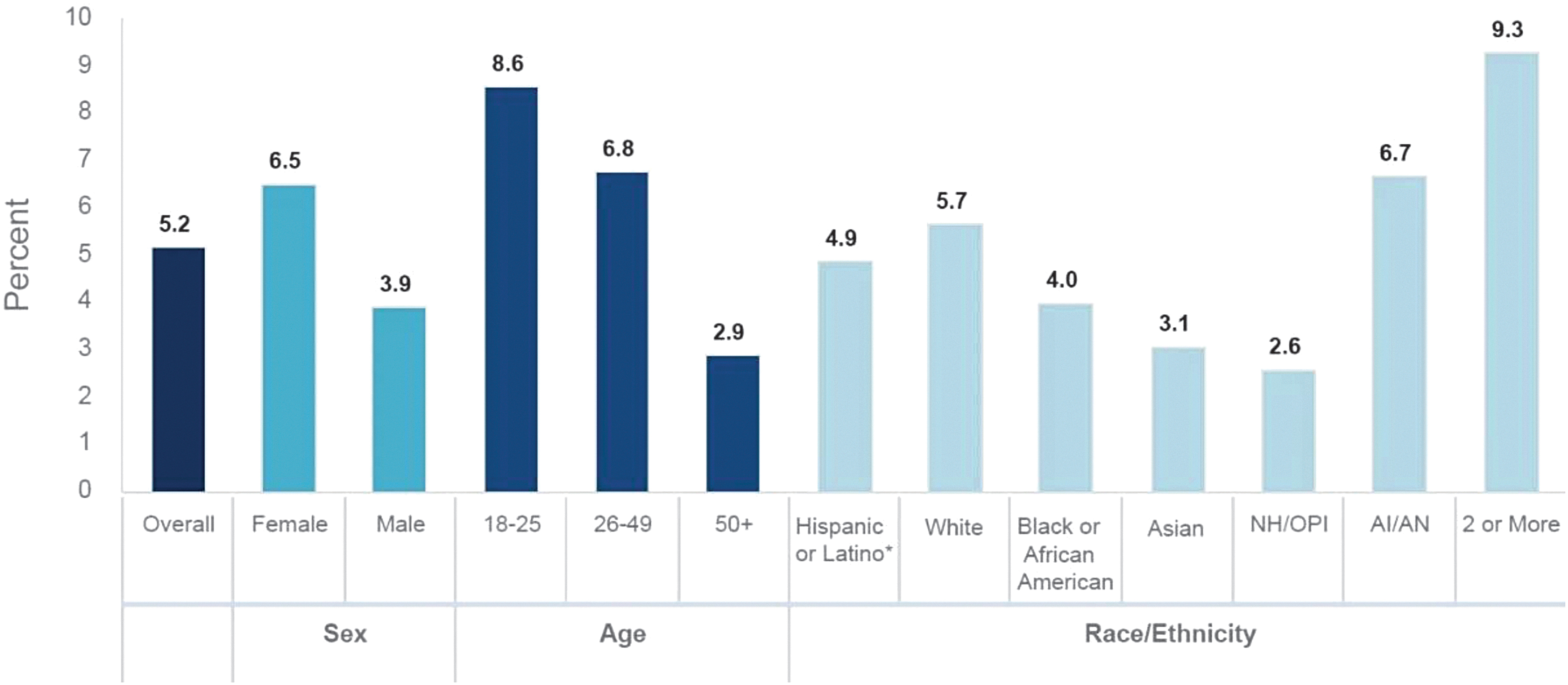
Past year prevalence of serious mental illness among US adults (2019).*
Some individuals who recognize their own need for mental health care may not seek out professional help, and those seeking help may not receive appropriate care, resulting in unmet mental health needs (UMHNs). 2 –4 Attitudinal barriers, such as not perceiving a mental health need, is one of the most frequently cited reasons for not seeking mental health care. 2,4
Compared to the general population, individuals with SMI are nearly twice as likely to develop cardiovascular and metabolic diseases. 5 Consider that among patients diagnosed with SMI, common comorbid physical disorders may include hypertension (32.5%), cardiovascular disease (11.3%), and diabetes (7.5%). 6 In addition, intrinsic factors (eg, stress, inflammation, genetics) and extrinsic factors (eg, diet, lifestyle, socioeconomic status) in combination with the antipsychotic drugs necessary for treating SZ, for example, are associated with an increased risk for obesity, metabolic syndrome, and diabetes for patients in this population. 7 These individuals are at a higher risk of being unemployed as adults. 8 It is estimated that at least 8.4 million people in the United States provide supportive care to an adult with a mental or emotional health issue, and caregivers of adults with mental or emotional health issues spend an average of 32 hours per week providing unpaid care. 5
The societal burden of mental illness is considerable. Mental illness and substance use disorders are involved in 1 out of every 8 emergency department visits by a US adult—an estimated 12 million visits per year. 5 Nationwide, an estimated 20.1% of people experiencing homelessness are diagnosed with an SMI; approximately 37% of incarcerated adults have diagnosed mental illnesses; and 41% of patients admitted to Veterans hospitals have a diagnosed mental illness or substance use disorder. 5 Across the US economy, SMI causes an estimated $193.2 billion in lost earnings each year. 5
According to results from both the US National Comorbidity Survey and the Epidemiologic Catchment Area survey, up to 50% of individuals with an SMI had not received mental health care in the prior year. 8 UMHNs are high in patients with multiple health conditions. 2 Nonadherence to offered therapies may occur in patients with physical disease and mental health disorders. 2,9 A 2019 study by Shafrin et al demonstrated that 61.5% to 88.1% of patients who were nonadherent to their antipsychotics also were nonadherent to other prescribed medication classes (P < .001). 9 For patients with SMI, medication adherence is needed for optimal symptom stability and day-to-day functioning, and as such, it may be a precondition for adherence to other prescribed medications. 9 Consequences of UMHNs may lead to negative emotions in both clinicians and patients, which may result in either party experiencing feelings of frustration and powerlessness. 2
Attitudinal barriers are among the most frequently cited reasons for not seeking mental health care. 2 Some patients with SMI may not perceive a need to seek out professional help, and this insight is a prerequisite for demanding care. 2,10 Other individuals prefer to deal with their problems on their own. 2 Insight into one's own illness may be lacking in individuals with low mental health literacy. In other words, some people feel something might be wrong, but do not know how to articulate their experiences or how to explicitly ask for help. 2
One of the biggest obstacles to effective management of SMI is that individuals living with these conditions are often difficult to engage consistently in treatment. 11 Poor engagement is associated with not fully realizing the potential benefits of treatment, symptom relapse, and rehospitalization. 11 The principles of behavioral economics are one of several concepts that can help shed some light on the reasons for this.
As an academic discipline, behavioral economics focuses on why investors, organizations, and individuals make financial decisions that are not always entirely rational, conscious, or fully aligned with their best interests. 12 When applied to medicine, the principles of behavioral economics are useful in understanding why individuals sometimes make decisions based on immediate gratification rather than on the potential for harm when faced with obvious behavioral challenges (eg, choosing to eat a delicious but unhealthy meal, not taking medication as prescribed to treat a serious condition). 12 Behavioral economics research shows that even patients who comprehend the likely benefits of medications may be swayed by variables such as possible side effects and/or co-payments that lead them to deviate from their treatment regimens. 12 Social determinants of health, such as health literacy, access, transportation, and economics, also may lead patients to not follow prescribed treatment. This phenomenon may help explain why near-term elements and incentives, such as medication reminders, free trial offers, and other educational efforts to impact medication adherence are often ineffective. 13 Incentives may support adherence for patients with SMI, but one study suggests that some incentives become less effective over time, and improvements may be lost once incentives are removed. 12
The Importance of Patient-Centered Care and the Provider–Patient Relationship in Treating Patients with SMI
A variety of factors may influence a patient's engagement in treatment. Patient-centered care that facilitates shared decision-making may be useful for engaging patients in behavioral health care. 8 Individuals with SMI stand to benefit from patient-centered care because, by addressing the full complement of their needs, it serves to bolster the therapeutic alliance. 8 In essence, patient-centered care is a vehicle for engaging and empowering patients as active partners with their clinicians and caregivers in determining their treatment and managing their chronic condition. 8
Shared decision-making, a cornerstone of participatory medicine, is a beneficial approach. Rather than directing patients to do something, shared decision-making informs patients of beneficial treatments and “nudges” them toward making choices that are in their best interest. In contrast with more authoritative models, shared decision-making is a collaborative, dynamic, interactive process in which patients and providers act as equal partners in exchanging information and reaching a mutually satisfying agreement regarding treatment decisions. 8 Literature suggests that focusing on patient-centered care and shared decision-making can improve patient-centered communication and help engage patients in their mental health treatment decisions. 8
A related principle of “concordance” views the provider–patient relationship as a partnership agreement between the parties that considers the perspectives of both and can lead to open discussion regarding medication taking, information sharing, and support. 14 Ultimately, concordant relationships actively involve patients in planning and goal setting, and encourage greater participation in managing their chronic conditions. In the context of SMI, this concept lends itself to care being driven by the physician's insight and incorporated into the patient's perspectives.
Approaches to Assessing Medication Ingestion
Concordance focuses on adequate communication and the physician–patient relationship as the cornerstones of the medication-taking process. 14 Adherence to prescribed medication is vital to the effective management of symptoms associated with SMI. Patients with SMI who do not adhere to prescribed treatment are at high risk for suboptimal response and substantial consequences that may include increased risk of relapse and/or hospitalization, recurrence of symptoms, impaired social functioning, and impaired occupational functioning. 15,16 Unfortunately, nonconformity with prescribed medication regimens is common among these patients, ranging from 20% to 72% for SZ, 20% to 50% for BP-I, and 28% to 52% for MDD. 16 This presents additional challenges for treating physicians as well as for patients and their families.
Over the years, a variety of approaches and tools have been developed to assess medication ingestion with greater accuracy. However, the evidence shows that none of these is without limitation (Table 1). As an example of clinical intervention, the American Psychiatric Association (APA) treatment guideline for depression calls for an assessment of adherence levels prior to any change in medication for patients who are exhibiting a suboptimal response. 17 For patients with MDD who have not responded to initial treatments with an antidepressant after 4 to 8 weeks of use, the APA recommends assessing the patient's medication-taking behavior prior to making adjustments to the treatment plan. 17 The guideline does not recommend a specific method as standard of care for assessing adherence.
Current Approaches to Assessing Medication Ingestion
Technology-assisted monitoring refers to digital caps that measure the opening of medication bottles.
White coat syndrome (also known as “white coat hypertension”) is a term used to describe occurrences wherein some patients present with high blood pressure levels in a provider's office, yet readings return to normal levels upon return to their typical environment.
The value of objective data in making treatment decisions cannot be overstated. When confronted with a suboptimal therapeutic response, the clinician needs objective information regarding the patient's medication-taking behavior and any potential barriers to adherence. This is challenging when the assessment relies on patient self-reporting. Retrospective reports from patients can be unreliable because they are not collected at the time they occur. 18 Individuals with SMI also are susceptible to memory impairment that may impede recall. 18
Clinicians' perceptions of their patients' adherence to medications is often misaligned with real-world estimates of medication-taking patterns among patients with SZ and/or bipolar disorder. 19 One study in which 44% of physicians overestimated their patients' treatment adherence found that this was true even among those with well-established patient relationships. 19
Digital Patient Data to Support Condition Management
Digital health is a broad category that encompasses digital medicine. 20 Digital health comprises a wide range of tools that engage patients for clinical purposes; gather, organize, interpret, and use clinical data; and allow for patients to track, document, and report outcomes, as well as other measures of care quality. 21 This list includes a range of digital technologies involving telemedicine and telehealth, wearables and activity trackers, mobile health (mHealth), apps, remote monitoring, and others. 21
The emerging field of digital medicine explores the potential benefit of using technologies as tools for measurement and intervention in health care delivery.
20
Based on high-quality hardware and software that support health research and clinical practice, digital tools may be able to help with treatment, recovery, and health promotion for individuals and populations.
22
Digital medicine products are evidence-based digital tools that can be used alone or in connection with pharmaceuticals, devices, or other products to address a wide range of conditions.
22,41
Examples of such technology already in use include the following
20
: Measurement products—digital biomarkers, electronic clinical outcomes assessments, wearable sensors to track falls Intervention products—digital therapeutics, connected implantable technologies (eg, insulin pump) Combination products—measurement and intervention (eg, continuous glucose monitor).
In recent years, digital medicine products have been evaluated as a means of improving outcomes for patients with chronic physical conditions. For example, a study using a digital medicine product for patients with comorbid hypertension and diabetes showed that approximately 98% (106/109) of patients achieved blood pressure targets within 90 days. 42
Patients with chronic physical conditions and co-occurring mental health disorders also may benefit from evidence-based digital tools. A digital medicine product could help support illness self-management by potentially helping patients monitor their physical symptoms and mental health. For example, the data derived from such technology could help support interventions for weight reduction associated with antipsychotic medications. 43
As health care expands its footprint in the digital space, emerging technologies that facilitate provider–patient communication may, in turn, be able to help measure adherence to treatment and impact care. 21 The hope is that by encouraging open communication, digital tools may help strengthen the therapeutic alliance between physician and patient. A variety of new mental health applications and interactive data-driven interventions may be able to function as adjuncts to treatment for educating patients, motivating positive health behavior and self-care, and monitoring disease in the home setting. 21
However, as the field of digital medicine emerges, future research will be needed to evaluate the potential impact of digital tools on treatment outcomes in patients with SMI. 44 There may be value in examining intermediate outcomes, which are important for the assessment of data-driven interventions. 44 For example, the effect of using digital patient data to support providers and patients in managing SMI is influenced not only by the data derived from a digital tool, but also by a host of other factors, including health literacy, access, transportation, poor engagement, and biomedical factors such as whether a person responds appropriately to prescribed treatments or has comorbidities. 44 A systematic framework of how a data-driven intervention functions may be helpful in understanding the pathways through which a data-driven intervention may influence a targeted behavior. 44 This framework also will help in selecting appropriate outcomes along these pathways to evaluate. 44 Future research also will be needed to assess and examine how digital tools might best be deployed in clinical practice.
Provider and Patient Adoption of Digital Tools
In 2016 and 2019, the American Medical Association conducted a survey of physicians to determine their motivations and requirements for adopting digital tools. 21 The types of tools included in the survey were related to the following 21 :
Remote monitoring for efficiency (smart versions of common clinical devices, such as blood pressure cuffs)
Remote monitoring and management for improved care and patient engagement (apps and devices for daily measurement and transmission of vital signs to the physician)
Clinical decision support (modules used in connection with the electronic health record that flag significant changes in measurements, such as blood glucose)
Tele-visits/virtual visits
Point-of-care workflow enhancement (communication and clinical data sharing for referrals and/or transitions of care)
Consumer access (secure method for physician–patient communication that also permits patients access to their clinical information).
Among the more remarkable attitudinal shifts from 2016 to 2019 were an increase in the number of physicians (especially primary care providers) who perceive advantages in using digital tools; a growth in technology adoption that is unrelated to gender, specialty, or age; a significant increase in adoption of remote care; and a high awareness of emerging technologies, such as artificial intelligence. 21
Recent reports indicate an even more dramatic rise in technology adoption by physicians during the COVID-19 pandemic. Results of one survey of 70 specialists (from cardiology, gastroenterology, and pulmonary/respiratory medicine) estimated that 79% of participants increased their use of virtual care between March 2020 and when the survey was conducted (May 27–July 2, 2020). 45 Fewer than half of those surveyed reported using telehealth prior to that time. 45 Another survey (N = 476) estimated that of the 86% (409/476) of behavioral health providers who used telehealth for the first time in the past 6 months, 75% (357/476) reported that they intended to continue offering virtual visits 40% (190/476) or more of the time even after the pandemic. 46
Skeptics may believe that patients with SMI will not use technology. However, a small but growing body of evidence suggests that people with mental illness already use digital tools to support their recovery and leverage technology in a manner similar to the general population. 47 A National Alliance on Mental Illness survey revealed that individuals with mental illnesses already have an appetite for digital tools, with a high rate of ownership and utilization of technology among, for example, people with SZ. 47 Specifically, 90% (411/457) reported access to 1 or more technologies, 61% (279/457) had access to 2 or 3 devices, and 54% (247/457) had access to a smartphone. 47 In responses to questions about SZ, 66% (302/457) anticipated an increasing role for technology in recovery, and 36% (165/457) reported using web-based technology often or very often to cope with their mental illness. 47
Conclusion
Physicians may be able to leverage digital tools to give them a clearer understanding of the factors that affect adherence and help them provide objective data to facilitate management of patients with SMI. 48 Digital tools can assist physician–patient relationships, which may potentially help improve treatment outcomes. 48,49 The intended outcomes of shared decision-making include improved communication and more effective treatment. 48
The pandemic has forced the health care industry to reassess traditional ways of providing care, and serious attention should be given to leveraging available technology. Today's digital tools may help patients engage in their care, partner with their providers to determine treatment goals, and share in ownership of desired health outcomes. 50 The time has come to consider how digital tools may affect patient outcomes and support disease self-management.
Footnotes
Author Contribution Statement
Dr. Skoufalos: conception/design, drafting the article, critical review/revisions, final approval. Dr. N'Dri: literature review, analysis, interpretation; drafting the article. Mr. Waters: literature review, analysis, interpretation; drafting the article.
Acknowledgments
The authors thank Janice Clarke of Jefferson College of Population Health at Thomas Jefferson University for her contributions to reviewing the literature, consulting with designated experts, and for providing technical writing support for the manuscript.
Author Disclosure Statement
Dr. Skoufalos is Associate Dean for Strategic Development at Jefferson College of Population Health at Thomas Jefferson University. She has served as a consultant to Otsuka America Pharmaceutical, Inc. in support of the National Steering Committee for Digital Medicine. Dr. Skoufalos did not receive compensation for her contributions to this work. Dr. N'Dri is a 2nd-year Fellow in Health Economics and Outcomes Research at Jefferson College of Population Health at Thomas Jefferson University. Dr. N'Dri did not receive compensation for her contributions to this work. Mr. Waters is a 2nd-year Fellow in Health Economics and Outcomes Research at Jefferson College of Population Health at Thomas Jefferson University. Mr. Waters did not receive compensation for his contributions to this work.
Funding Information
Jefferson College of Population Health at Thomas Jefferson University received funding from Otsuka America Pharmaceutical, Inc. to support the development of this article.