
Abstract
The integration of medical schools and clinical partners is effectively established through the formation of academic medical centers (AMCs). The tripartite mission of AMCs emphasizes the importance of providing critical clinical services, medical innovation through research, and the education of future health care leaders. Although AMCs represent only 5% of all hospitals, they contribute substantially to serving disadvantaged populations of patients, including an estimated 37% of all charity care and 26% of all Medicaid hospitalizations. Currently, most AMCs use a business model centered upon revenue generated from hospital services and/or practice plans. In the last decade, mounting financial demands have placed significant pressure on AMC finances because of the rising costs associated with complex clinical care and operating diverse graduate medical education programs. A shift toward population health-centric health care management strategies will profoundly influence the predominant forms of health care delivery in the United States in the foreseeable future. Health systems are increasingly pursuing new strategies to manage financial risk, such as forming Accountable Care Organizations and provider-sponsored plans to provide value-based care. Refocusing research and operational capacity toward population health management fosters collaboration and enables reintegration with hospital and clinical partners across care networks, and can potentially create new revenue streams for AMCs. Despite the benefits of population health integration, current literature lacks a blueprint to guide AMCs in the transformation toward sustainable population health management models. The purpose of this paper is to propose a modern conceptual framework that can be operationalized by AMCs in order to achieve a sustainable future.
Introduction
Since the Flexner report, published in 1910, US medical schools have pursued a common vision of 3 integral roles: education, research, and clinical care. 1 This triple mission of academic medicine has fundamentally impacted the organizational structure of US health systems. Namely, medical schools and clinical partners, including hospital and physician practices, have become increasingly integrated through the formation of academic medical centers (AMCs). Within an AMC, education, research, and clinical care are combined to deliver improved therapies, generate novel medical breakthroughs, and conduct exclusive clinical trials not traditionally available in other hospital settings. 2
Over the past decade, the integrated AMC structure has favored a business model through which the academic missions of education and research have received financial support from clinical enterprise revenues (hospital and/or practice plan). These clinical initiatives and concentrated specialty expertise allow AMCs to provide complex tertiary care, which supplies direct feedback into research missions. Specifically, established medical schools with an integrated teaching hospital, under the same institutional governance, were able to succeed by balancing the allocation of revenues and expenses across the 3 missions. 3 According to the 2019 Liaison Committee on Medical Education reports, 63.1% of revenue for 141 accredited US medical schools was generated from either practice plans (42.9%) or hospital purchased services and investments (20.2%). 4 Figure 1 depicts the distribution of annual revenues of all US medical schools for fiscal years 2017 to 2019.
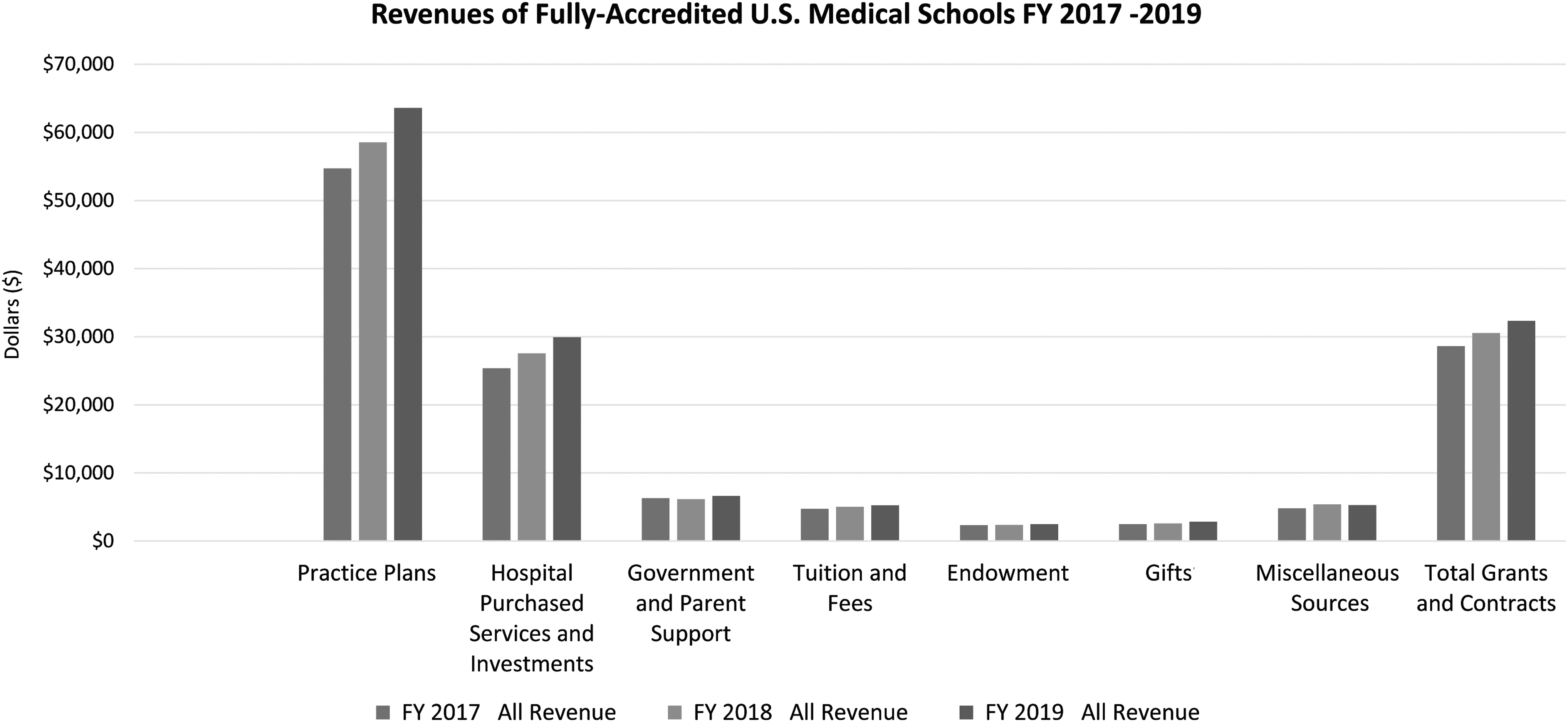
Revenue distribution of fully accredited US medical schools for FYs 2017 to 2019. Source: Association of American Medical Colleges. FY, fiscal year.
Notably, medical schools have become increasingly reliant on practice plans and hospital purchased services over the past 3 years. Moreover, these services are further protected under “safe harbor” exemptions. 5 However, unprecedented financial pressures have mounted on AMCs in the last decade because of rising labor costs, declining public research funding, suppressed tuition revenue, and demographic changes. Although, historically, medical schools have relied on the biomedical research enterprise for support, the indirect cost of reimbursement associated with achieving grant funding often does not cover the infrastructure needed to support this mission. Inevitably, AMCs are forced to subsidize their research efforts and contribute up to 30%, or hundreds of millions of dollars. 6
A majority of AMCs operate in a not-for-profit business model, providing health services to the community that often fail to yield a positive financial margin. 7 AMCs and teaching hospitals of the Association of American Medical Colleges account for only 5% of all hospitals, despite providing services for approximately 37% of all charity care, 26% of all Medicaid hospitalizations, and 38% of transfers from outside hospitals, to treat complex patients who necessitate highly specialized care. 8 Furthermore, AMCs are responsible for operating regional standby services, including 80% of level 1 trauma and burn centers, which necessitates specialized equipment, facility, and staff to be ready at all times. This role forces AMCs to incur daily costs to ensure preparedness, which in turn impacts their overall financial well-being. 6 For-profit hospitals often avoid facilities such as level 1 trauma and burn centers, as they fail to generate a financial return significant enough to fulfill their fiduciary responsibility.
Graduate medical education also places a significant financial burden on AMCs, despite the inherent community and societal value in fulfilling this mission. Although AMCs provide student trainees with ideal learning environments, including exposure to and thorough immersion in clinical settings, the direct cost of training residents and fellows accounts for more than $16 billion annually. 7 While Medicare and grant programs from Veterans Affairs and Medicaid provide modest financial support (approximately $3 billion), AMCs are left to cover a majority of the direct cost. 9,10 These financial pressures, coupled with the advent of health care reform, including the implementation of value-based models, present the opportunity to challenge how AMCs operate.
In order to support its tripartite mission in today's evolving health care industry, academic medicine is forced to reinvent its operational and financial models. Population health management holds the potential to enable AMCs to address future health care needs and create new and more financially viable revenue streams. Notably, vital opportunities exist including leveraging and extending AMCs' research capacity toward population health management, the measurement of health outcomes through health data integration, and the elucidation of social determinants of health. Although current literature has presented modernized approaches to combat AMCs' reliance upon clinical revenue and the importance of population health, actionable models are needed in order to guide AMCs throughout this change. 11,12 With more than 60% of traditional revenue at stake, the success of academic medicine requires a modernized business model in today's modern health care landscape.
Herein, the authors present a foundational framework for AMCs by establishing an integrative environment along 4 pillars, which are defined to be: (1) health outcomes, (2) economic benefit, (3) research and innovation, and (4) education.
Fundamental Changes in Health Care
Changing economics and payors' emphasis on higher quality at lower cost exert tremendous financial pressure on health providers. Health care organizations are striving for efficiency, cost control, and sustainability. The induction of the Affordable Care Act has ignited this change in health care delivery and continues to be a driving force in establishing efficient, value-based care. Moreover, market consolidation activities have increasingly led to mergers of hospitals with faculty group practice plans within AMCs, the latter of which was traditionally the major driver of revenue for medical schools. With the academic and clinical arms of the AMC becoming increasingly decoupled, the financial and organizational model of the AMC has been challenged. Every aspect of how the educational and research enterprises are organized and funded will undergo significant transformation in the decades ahead.
Medical school administrators and deans who have been relegated to manage the academic cost centers of research and education are increasingly becoming “beggars with a tin cup,” unless academic support agreements are established that provide essential subsidies through other revenue sources in perpetuity. 13 The traditional structural relics of AMCs are lacking funding capabilities and posit minimal decision-making capabilities in today's health care environment. As health care funding has expanded in the past 2 decades, AMC business models have become reliant on incentivizing clinical faculty through health care services and referral patterns. Inadvertently, this emphasis has created large, specialized health systems that have given more control to administrators as the financial model transitions away from the traditional academic moniker and mission of AMCs.
Unfortunately, because of the inertia of academic legacy systems and the market dominance of larger health systems, there is a fundamental lack of actionable solutions designed to achieve sustainability on a broader scale. Moreover, because of the diversity in the structure of the US medical school system, universally applicable, one-size-fits-all solutions will not be suitable. While a tailored approach is necessary for individual AMCs, guiding principles can be established and presented to help AMCs evolve in this changing environment.
From Health Service to Population Health Management
Population health is a discipline that is focused on the measurement and distribution of health outcomes as well as the patterns of determinants of health. Determinants may include medical care, public health interventions, genetics, and individual behavior, along with components of the social and physical environments. According to Kindig and Stoddard, population health can be defined as a data-driven approach that (1) focuses on interrelated conditions and factors that influence the health of populations over the life course, (2) identifies systematic variations in their patterns of occurrence, and (3) applies the resulting knowledge to develop and implement policies and actions to improve the health and well-being of those populations. 14
The convergence of scientific insights from population health and related fields, such as public health, epidemiology, health services research, and implementation science, represents a seismic shift in how health care professionals define and measure health outcomes, design and implement interventions, and formulate policies. Population health research also has become a critical perspective in modern health education, as exemplified by a noticeable expansion of new research and training programs in the United States. Additionally, there has been a significant rise in the last decade within allopathic medical schools in new departments of population health – or population medicine – with dedicated faculty members. 15 Academic investments in population health carry significant potential to enable academic-public partnerships and to advance vital components of the triple mission that have been stymied for lack of alignment with external trends and incentives.
The implementation of population health principles into the AMC business model has the potential to advance clinical outcomes, generate a network for societal health advancement, and provide financial support to AMCs. Figure 2 depicts how the determinants of health and population health sciences, through data sciences and analytics, can be translated into managerial applications and activities that can result in value-based health outcomes for individuals and populations.

Translation of population health science principles into management applications.
Studies have shown that 80% of health outcomes are associated with factors outside the traditional boundaries of health care delivery, including health behaviors (eg, tobacco use, sexual activity), social and economic factors (eg, employment, education, income), and the physical environment (eg, air quality, water quality). 16 When health care delivery systems strategically expand their interactions with individuals in their communities, outcomes improve and quality of care increases. By identifying and segmenting health environmental risk factors, as expressed in Figure 2, providers can develop and implement data analytics and incorporate population health applications to optimize clinical outcomes for the patient and financial outcomes for the system. These goals can be achieved through a multipronged approach including the application of select management tools with respect to process, outcomes, data analytics, cost, competency, and system-wide collaboration.
A New Academic Model: Population Health Management
Population health and variations thereof have the potential to serve as a predominant model of health care within the next decade. Health organizations are increasingly pursuing new programs that take on financial risk, such as Accountable Care Organizations (ACOs) and provider-sponsored plans. The combination of these factors contributes to a new form of population health management. To reach this goal, health and academic partners must work together to accelerate the development of strategic areas while managing expectations. Notably, health care systems need to improve the way in which they collect reliable and valid patient outcome data, rather than relying on proxies for care. For example, while it is important to perform a foot exam on a diabetic patient, the exam – a critical component of the process of delivering care – in and of itself, does not guarantee good outcomes. Hence, the measurement of health outcomes is an integral part of health management. Organizations also must understand and track true cost at a granular, highly specific level instead of approximating costs, as in the current model. The current approach is almost meaningless when managing margins.
Existing health systems rarely implement these or other adjustments in order to achieve population health management in an environment of academic medicine. Currently, AMCs focus solely on growing the academic enterprise through cross subsidization of clinical revenues to other missions, including education and research. Furthermore, the academic clinical enterprise is part of a largely fragmented health care system in the United States. Care delivery involves multiple providers and organizations with no effective coordination of different aspects of care. 17,18 As a result, fragmentation across providers leads to suboptimal care, poor patient outcomes, and unnecessary and/or harmful services that ultimately both raise costs and degrade quality. 19
In the era of population health, opportunities exist to redesign the economic model of the academic enterprise by utilizing its educational and research capacities toward health services management. A new organizational model, shown in Figure 3, extends traditional academic capacities toward population health management.
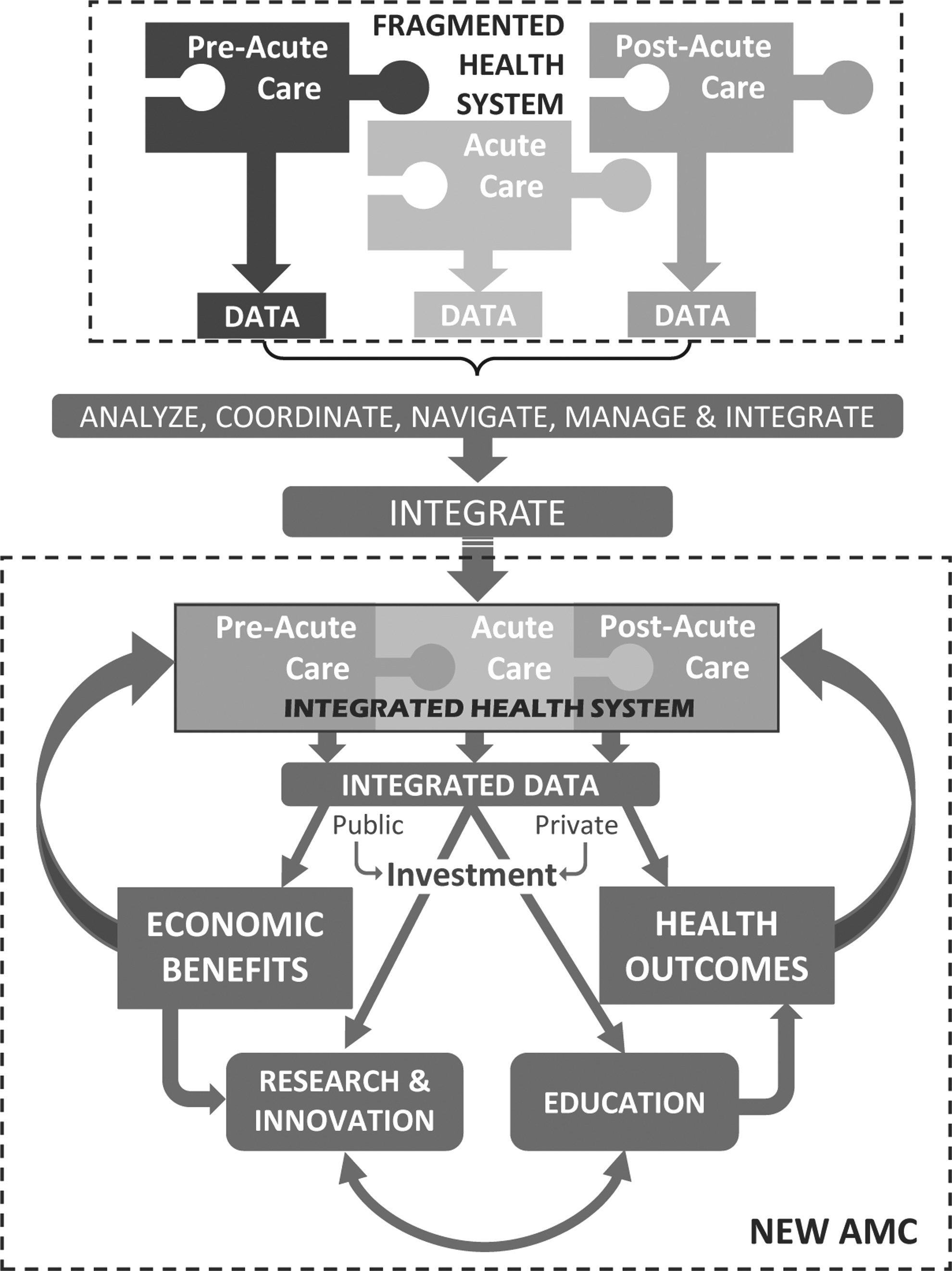
A new organizational model for AMCs.
Currently, the clinical enterprise of most AMCs is but one player in a very fragmented health system attempting to deliver quality care and generate revenues, while providing education and advancing biomedical research. These clinically based revenues, coupled with additional external private and public investments, grants, and contracts, creates subsidies to support the tripartite mission of the AMC. Under the proposed model, AMCs should leverage research in population health science to drive integration of health systems in their catchment areas in order to deliver value-based health outcomes and create economic benefits that support external private and public investments, grants and contracts, research, and education. Furthermore, through the development of an integrative health system, integrating patient qualitative outcomes, cost accounting data, and mechanisms for collaborative care management, the model improves quality of care and mitigates financial risk. Adoption of the new model focuses on integration with health systems outside the traditional care model, leading to a more diverse portfolio of revenue sources for the AMC. Although the literature has pointed to the conceptual integration of population health and AMCs, limited frameworks exist to guide the process. 20,21
It should be noted that AMCs that own their own health system or hospital first need to focus on implementing a value-based approach within their system and then strategically support integration with selected partners in the community. For AMCs without their own health system, striving toward the development of integrative health care partnerships and working toward the creation of an integrated network can allow for further integration of population health strategies and safeguards against the current financial constraints of the traditional reimbursement system. Identifying the characteristics and potential limitations of an individual AMC and creating an individualized approach to implementing population health management strategies can lead to optimal implementation.
The modern conceptual framework for AMCs can be fulfilled by establishing an integrative environment with specific adherence to 4 pillars of health outcomes: (1) health outcomes, (2) economic benefit, (3) research and innovation, and (4) education.
Health outcomes
Of utmost importance is the overarching purpose of an AMC: to provide world-class clinical care to patients while training the next generation of physicians. In the population health framework, clinical care extends beyond treatment of disease to include overall wellness, preventive medicine, and optimized management of chronic conditions. 11 Guided by a shift from specialized, acute care services to integrative primary care and community-based health management programs, population health seeks to further engage patients to provide higher-quality, value-based care. The impact of various critical applications for population health management expands from access and data management, to health outcomes, cost management, policy adjustment, creation of a collaborative network, and competency management for trainees (Table 1). Table 1 was not intended to serve as a comprehensive list of all possible population health management tools, but rather was created to categorize important applications available that align with the proposed model (Figure 3). With respect to health outcomes, the incorporation of risk prediction and consideration of patient-level qualitative outcomes seeks to enhance the overall patient experience, while simultaneously mitigating disease processes. The successful integration of population health into large health systems has been mentioned in the literature. Notably, Stevens et al 22 identified efficient resource allocation for population health strategies at Kaiser Permanente, according to a simulated risk model of the top causes of US mortality.
Categorization and Impact of Critical Application for Population Health Management
ABC, activity-based costing; GIS, Geographic Information Systems; HCAHPS, Healthcare Consumer Assessment of Healthcare Providers and Systems; IT, information technology.
Population health initiatives, including patient-centric care and value-based reimbursement models, can optimize coordination between physicians through care continuity and minimize fragmentation of care. Early indications have identified promising outcomes with population health models, such as patient-centric medical homes, patient navigators, and ACOs, which seek to deliver continuous patient-level care, in a cost-effective manner. 23 Furthermore, alignment between health care delivery systems and population health goals will become increasingly important for AMCs.
A key opportunity for developing population health within AMCs is to encourage a holistic view of health, with adherence to clinical, social, and political determinants of health. Furthermore, policy impact with respect to standard operating procedures, environmental protection, economic development, and health education would extend the engagement of health beyond its conventional focus on the sick to community-based care. 24 Relationship building and care management that provide health systems with tools such as patient risk stratification, enrollment in risk-based plans, and care communication and coordination among members of a patient's care team can contribute to the successful implementation of population health management strategies.
Moreover, developing trust among community members remains critical, specifically in underrepresented populations, through equitable and supportive engagement, which can lead to long-term sustainable health outcomes. 25 Although levels of mistrust in health care and biomedical research remain high in minority communities, population health management strategies can potentially serve a significant role in relationship building while positively impacting adaptive health behavior engagement. 26 A one-size-fits-all approach will not work. For optimal outcomes, patients must be capable and willing to participate in their own care to achieve the highest possible outcomes. This includes widespread patient engagement for low-risk populations and personalized management programs for complex or high-risk patients.
A health system must adjust strategies to reflect that risk and distribute care management resources accordingly. Patient-reported outcomes and metrics of functional and social status extend beyond disease-specific measures and can drive clinical services provided to communities most in need. For example, if metrics indicate that patients in a given community are at increased risk of diabetes, a population health delivery system can synergize with local resources to develop focused strategies within that community. 27 Here, AMCs can facilitate the bridging of traditional health care metrics with patient or community outcomes. 20 For example, the NYU School of Medicine, a large AMC serving a diverse population in New York City, has successfully established a population health department and effectively incorporated population health management models into its traditional care pathway. 21
The transformation from health services delivery to health services integration and health management also represents a critical component of population health (Figure 4). Through the combination of modern cost accounting, community care management, advanced clinical training, and technology-driven health outcome analysis and management, AMCs can improve performance, and access to coordinated care. 28 The conventional AMC business model relies on the development of subspecialty services and treatment of complex, high-risk patients, for whom incentives for prevention are lacking.

Shift from health services delivery to health services management.
Economic benefit
Currently, AMCs are oriented toward a fee-for-service, high-cost specialty system, where revenue is generated based on the type and quantity of services provided. This business model, centered around referral-based, acute care procedures, continues to present increasing challenges. 29 A transformation to population health management would alter the existing revenue structure to accountability-driven payment models, reducing health inequities, and competing for value-based contracts. With respect to clinical care, AMCs commonly fulfill roles as a regional referral center for complex coordinated care, and a referral center for select subspecialties. 12 Furthermore, AMCs traditionally invest in modern, cutting-edge medical equipment and facilities, including research initiatives. The high fixed costs associated with this aspect of the business model historically draws hospitals to maintaining these specialty procedures and high hospital occupancy rates. The competing vision between traditional AMCs and population health management requires complete participation from organizational leadership and establishment of dedicated resources for successful implementation. AMCs can begin this transition by first identifying the underlying conflicts within the existing business models and engage leadership's willingness to shepherd the health system through inevitable challenges. 30
A vital component of the economic benefits of population health management resides in the inherent value of offering higher quality care to a larger percentage of the population. The inclusion of more diverse revenue streams can be developed through ACOs and a transition to value-based reimbursement, which incentivizes preventive treatment modalities and coordination across the care continuum. Increasing a health system's ability to manage risk-based contracts and bundled payment models seeks to incentivize valuable patient care. 31 This includes ensuring health care organizations can understand cost in a population health context and can manage that cost, while also confirming that organizations are aware of pertinent margins. This is the first manageable step in population health—managing the margins in per-member per-month bundled payment contracts. Before a health care organization can launch into gathering outcomes, socioeconomic data, or using a care management application, it must first understand the population it serves and the costs of care. Accountability-based models, as well as capitation or bundled payment structures, incentivize providers to provide highly efficient care, which promotes patient well-being and mitigates the need for advanced, expensive therapies. 32 As payment structures evolve toward optimized risk management of specific populations by the health system, the value of the strategies that reduce the use of these services will continue to rise.
Utilization of activity-based costing can allow accurate management of financial margins in reimbursement contracts and support AMCs in the implementation of value-based care, to create improved patient care at a more efficient cost. 33 Activity-based costing also can help identify excess capacity and assist in strategic decision-making, to ensure lower cost services and efficiently deploy resources where needed. By instilling population health management strategies, AMCs will benefit from modernized payment methods.
Research and innovation
Although AMCs thrive on innovation, many of the inherent features that position them well in this arena limit their success in a value-based system. Achieving integration, improving access to care, and optimizing care coordination are all critical elements of achieving this transformation and all need data, analytics, and technology to support population health management. 34 Many health systems have neither the information nor the technological infrastructure needed to support this transition. The absolute minimal data sets required for this work include patient-reported outcomes data, social determinants of health data, and activity-based costing. Through effective utilization of these 3 integrated data components, an institution can fulfill aspirations of value-based care and the creation of an integrative, collaborative, health care network. 35
Various examples exist throughout the literature. 36,37 Actionable risk prediction tools have demonstrated value in preventing adverse events, and, in a population health setting, hold the potential to further mitigate advanced disease adverse outcomes through early intervention. The development of an integrated system also presents the opportunity for simplified care coordination among clinical staff and can eliminate fragmented care, commonly experienced, and typically not addressed, by the traditional AMC model. Furthermore, a collaborative network facilitates implementation reimbursement based on quality outcomes and ensures proper incentives are allocated appropriately. Moreover, linkages among health information technology systems, with either passive or actively aggregated patient outcomes, offer a modern tool to identify trends in behavior and further assess subgroups within the communities. 38,39
AMCs nationwide have placed significant value on traditional funding mechanisms for research endeavors such as the National Institutes of Health (NIH) and other federal and nonfederal sources. Although the NIH has supported some research congruent with population health, further expanding the amount and scope of population health research is needed. Furthermore, transitioning from the long-standing tradition of biomedical and clinical research toward a tradition that is more population health oriented will require increased and stable departmental support within AMCs. Long-term improvements can be identified by developing mutually beneficial partnerships with the private sector, service grants at the county and state level, and population health contracts.
Education
AMCs serve a crucial role in educating current and future health care providers. Notably, through annual support from governmental graduate medical education (GME) funding, AMCs have a direct impact on how competency and quality training are assessed. Furthermore, AMCs also serve as a main source of medical education for the surrounding community, thus influencing not only academic physicians, but community members and stakeholders. 40 Modernized initiatives in medical schools have sought to educate students on the delivery of health care as well as nonmedical influences on health, including social determinants of health. 41
AMCs serve a critical role in mitigating the impact of health disparities and instilling community trust through the engagement of key stakeholders and community leaders. AMCs must continue to work with the community to address and overcome health disparities in their regions and beyond. Weaving population health pillars, such as population health management, tools, health policy, epidemiology, and disease prevention, into graduate medical curriculums will ensure future leaders' ability to understand the context of their clinical skills. 42,43
Furthermore, AMCs have the responsibility to train a combination of primary care physicians, specialists, and other health care providers in order to combat the physician shortage, specifically within the primary care field. The introduction of population health management practices early in medical training can potentially engage student physicians and educate the future generation of physicians regarding the growing importance of these strategies in improving overall health care quality and access and maximizing health.
A directive toward understanding and appreciating the impact of the social determinants of health, in an academic setting, also can help in generating innovative solutions to enhance access. Moreover, developing future health care providers who are cognizant of the environmental and economic impacts on an individual's health state can help improve the physician patient relationship, resulting in better health outcomes. 44 In order for ACOs and value-based facilities to succeed in the incoming health care system, engaging students at the precipice of primary care can help augment understanding while simultaneously providing an experiential learning experience. 45
In the past decade, academic institutions have started incorporating population health management values and learning initiatives into the curriculum for GME. 15 Gourevitch et al 15 have described the recent emergence of population health departments within AMCs. These institutions are positioned to drive change and lead the implementation of sustainable paradigm shifts toward population health management and continually advance the broad spectrum of the discipline. 46 The ideal framework for population health management requires individualization and unique tailoring dependent on each institution. 34 As federal and private market demands begin to change, leaders should proactively begin to adopt population health management strategies and set the stage for the future of care delivery models.
Future Direction
AMCs reside at the forefront of medical advancement and hold the potential to improve health care delivery. Although non-AMCs remain critically important to clinical care, AMCs can function as a gatekeeper to community health overall and serve a vital role in ensuring the successful implementation of value-based health care. While the presence of a health system associated with an AMC may emphasize specific components of the proposed model, this highlights the importance of an individualized approach needed for AMCs in order to effectively implement population health management strategies. The model presented herein can help guide AMCs, academic institutions, and community stakeholders through the value-based transformation of health care systems and can serve as a framework for developing and implementing population health management strategies.
Inevitably, there are significant challenges and limitations that must be overcome during the transition to population health management. Namely, the complexity and costly nature associated with technology integration, as well as navigating through associated tensions with accountable care health strategies. 47 Additional concerns regarding resource allocation, wholehearted executive leadership support, cost implications of implementing software, including early adoption technical issues, and learning curve errors for key stakeholders should be considered. Through developing an integrative, collaborative network centered around health analytics and coordinated managed care, AMCs can thrive in the burgeoning population health-based system. Future directions include augmenting the current model through the use of clinical and financial outcomes data, as AMCs transition into fully value-based care and continue to develop and implement population health management strategies.
Conclusion
Dynamic market conditions, immense financial pressures, and the decoupling of the academic and clinical arms of the AMC have necessitated the need for academic health centers to rethink their organizational and business model. The need to research, develop, and support population health management methodologies and systems, integrating big data analytics, patient engagement, and risk stratification technologies, is paramount. This “new mission” for medical schools is an opportunity to diversify the revenue portfolio, achieve better integration with health systems, and become an important component of population health systems. Population health management presents the opportunity to bridge the existing gap between medical science and health by generating an integrated collaborative network between patients, health care providers, and community stakeholders. The proposed framework presents a modern organizational model to assist AMCs to shift from a focus on health services delivery to population health management.
Footnotes
Authors' Contributions
Dr. Jacko: substantial contributions to conception and design, drafting the article for critically important intellectual content, and final approval of the version to be published. Dr. Sainfort: substantial contributions to conception and design, literature review, and interpretation of references, drafting the article for critically important intellectual content, and final approval of the version to be published. Mr. Messa: substantial contributions to conception and design, literature review, and interpretation of references, drafting the article for critically important intellectual content, and final approval of the version to be published. Dr. Page: substantial contributions to conception and design, drafting the article for critically important intellectual content, and final approval of the version to be published. Dr. Vieweg: substantial contributions to conception and design, review, drafting the article and final approval of the version to be published, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.