
Abstract
Evidence suggests that the patient-centered medical home (PCMH) model of primary care improves management of chronic disease, but there is limited research contrasting this model's effect when financed by a single payer versus multiple payers, and among patients with different types of health insurance. This study evaluates the impact of a statewide medical home demonstration, the Maryland Multi-Payer PCMH Program (MMPP), on adherence to antihypertensive medication therapy relative to non-PCMH primary care and to the PCMH model when financed by a single payer. The authors used a difference-in-differences analytic design to analyze changes in medication possession ratio for antihypertensive medications among Medicaid-insured and privately insured non-elderly adult patients attributed to primary care practices in the MMPP (“multi-payer PCMHs”), medical homes in Maryland that participated in a regional PCMH program funded by a single private payer (“single-payer PCMHs”), and non-PCMH practices in Maryland. Comparison sites were matched to multi-payer PCMHs using propensity scores based on practice characteristics, location, and aggregated provider characteristics. Multi-payer PCMHs performed better on antihypertensive medication adherence for both Medicaid-insured and privately insured patients relative to single-payer PCMHs. Statistically significant effects were not observed consistently until the second year of the demonstration. There were negligible differences in outcome trends between multi-payer medical homes and matched non-PCMH practices. Findings indicate that health care delivery innovations may yield superior population health outcomes under multi-payer financing compared to when such initiatives are financed by a single payer.
Introduction
Mortality rates from cardiovascular disease have decreased in high-income countries, including the United States. 1,2 This decline has been attributed in part to effective medication therapies for patients with hypertension. 3 Adherence to antihypertensive medication therapy is fundamental to reducing the risk of worsening cardiovascular symptoms, organ damage, and stroke in hypertensive patients. 4 Improving adherence to blood pressure control medications is an important strategy of the US Department of Health and Human Services' Million Hearts 2022 initiative to reduce the incidence of heart attacks and strokes. 5
The patient-centered medical home (PCMH)—or medical home for short—is an innovative model of primary care with strong potential to enhance management of hypertension and other chronic conditions. The model originated in pediatrics and is centered on continuity and coordination of the patient's care by an identifiable primary care physician and his/her care team. 6 The patient maintains a direct, longstanding relationship with this personal provider, who takes accountability for the care provided to the patient and organizes appropriate care for them across the spectrum of health care settings as needed.
Relative to traditional or routine primary care, the PCMH model is centered on safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity of health services provided. 7,8 The model also promotes better health for populations through emphasis on patient education, delivery of evidence-based preventive services, and care management for complex patients. 7
Previous evaluations have reported positive associations of the medical home model with antihypertensive medication adherence. 9 –11 These studies, however, analyzed data on patients covered by a single private or public insurer. Their study design limits the generalizability of findings to, and comparability of outcomes among, diverse payer types. The studies also provide limited inferences on whether the PCMH model is more effective when financed by a single payer or by multiple payers, a critical distinction in implementation that influences providers' administrative burden, the level of risk borne by any individual payer, and the proportion of patients in the practice likely to be covered by the program's incentives. 12 –14
The objective of this study is to evaluate the impact of a PCMH demonstration funded by multiple payers on antihypertensive medication adherence among publicly and privately insured patients, relative to a PCMH model funded by a single payer, and to non-PCMH care.
The chosen context, the Maryland Multi-Payor PCMH Program (MMPP), permits a robust evaluation of the effect of the PCMH model on antihypertensive medication adherence.
MMPP was a 3-year statewide demonstration of the efficacy of the PCMH model through which Medicaid and large private payers supported a group of primary care practices in the state of Maryland financially to function as advanced medical homes. Participating practices attained formal accreditation as PCMHs and received financial incentives for providing high-quality, cost-effective care to both their publicly insured and privately insured beneficiaries. At its inception, MMPP was among the most comprehensive of several ongoing statewide PCMH demonstrations, characterized by multi-payer involvement, national PCMH qualification standards for participating practices, care management and fee-for-service payments, and technical support to practices for medical home transformation. 15
This study evaluates the effect of MMPP on antihypertensive medication adherence for privately insured and publicly insured patients with hypertension. Outcomes for patients with hypertension in MMPP-participating multi-payer PCMHs are compared to outcomes of similar patients in non-PCMH practices, and in medical homes participating in a PCMH program financed by a single payer. PCMH effects are contrasted by type of patient's insurance, and under multi-payer versus single-payer PCMH financing structures.
Methods
Study setting
MMPP was instituted in April 2011 by legislative mandate authorizing the participation of Medicaid and the largest private payers in Maryland in a medical home demonstration to improve the efficiency and effectiveness of health services. 16 Fifty-three primary care practices from across the state were purposively selected by the Maryland Health Care Commission to represent a geographically and structurally diverse cohort of intervention sites. The final set was comprised of private and freestanding clinics, hospital-owned practices, and Federally Qualified Health Centers located in urban, semi-urban, and rural parts of the state. In aggregate, the selected practices were staffed by more than 300 physicians and nurses providing family medicine, pediatric, and geriatric health services. The patient population served included publicly and privately insured beneficiaries.
Ultimately, 52 of the 53 selected practices participated in MMPP till the end of the demonstration in December 2013. Participation in MMPP required practices to obtain medical home certification by the National Committee for Quality Assurance (NCQA) within the first year, and to achieve Level 2 or Level 3 certification in NCQA's ordinal 3-tier PCMH classification system 17 before the conclusion of the demonstration's second year. In addition to fee-for-service payments, participating practices received per-member-per-month (PMPM) care transformation payments for each attributed patient to perform medical home functions. PMPM payments ranged from $3.51 to $6.01 depending on the practice's PCMH recognition level, size of the practice's patient population, and whether the patient was insured by Medicaid or a private payer.
Each practice was mandated to spend at least one third of these funds on engaging a clinical care manager to facilitate care coordination for medically complex patients and patients with chronic diseases. Practices were eligible to earn shared savings from reducing aggregate patient expenditure and for meeting clinical quality standards. Shared savings were computed as the difference between the practice's historical medical expenses and current medical expenses per patient in a given year, and practices could earn between 30% and 65% of these savings depending on the practice type and performance on specified quality of care metrics. Practices also received technical support on medical home transformation and on quality improvement through a shared learning collaborative. 18 Interim assessments of MMPP 19,20 and an overview evaluation of the program have been published previously. 21
Study design and sample
A retrospective analysis was conducted of administrative data from 2010—baseline year preceding MMPP—till the final year of MMPP implementation (2013) on Medicaid-insured and privately insured beneficiaries attributed to MMPP-participating practices or to a matched cohort of comparison primary care practices in Maryland. Multi-payer PCMHs participating in the MMPP were propensity-score matched to: medical homes in Maryland participating in a regional PCMH program financed by a single private insurer; and primary care practices in Maryland that neither participated in MMPP nor in the single-payer PCMH program during the baseline year. The comparison groups were termed “single-payer PCMHs” and “non-PCMH practices,” respectively. Propensity scores modeled participation in MMPP as a function of practices' structural characteristics, locations, and aggregated patient characteristics. 21
PCMHs in the single-payer program were not required to achieve NCQA medical home certification, but the sponsoring payer required these practices to adopt core PCMH features including extended access, care coordination for patients with chronic and complex conditions, and emphasis on quality improvement. 22 Single-payer PCMHs received enhanced fee-for-service reimbursements equivalent to $10.34 PMPM and also were eligible for shared savings based on reductions in expenditure and quality performance. 23 These benefits, however, could only be received for their patients covered by the single sponsoring insurer. Under the program, single-payer PCMHs did not receive incentives for their patients covered by insurers other than the sponsoring payer.
The population of interest was non-elderly adult beneficiaries in multi-payer PCMHs or in comparison practices who were diagnosed with hypertension and had at least 2 filled prescriptions for antihypertensive medication therapy during the study period, from January 2010 to December 2013. Patients were attributed to the practice in which the plurality of their office-based encounters occurred during each calendar year. Data on hypertension diagnoses, prescriptions for antihypertensive medication therapy, and dates of prescription fills were obtained from adjudicated Medicaid claims and from the Maryland Medical Care Data Base, the private insurer portion of the state's all-payer claims database.
Included individuals were aged 18–64 years with a diagnosis code for hypertension recorded in an outpatient or inpatient encounter. In each year of the study period, excluded individuals were adults with ˂11 months of health insurance coverage, and female individuals with a diagnosis code for pregnancy. Included individuals recorded ≥2 filled prescriptions of the 5 principal drug classes recommended for first-line and secondary management of hypertension in the Seventh Report of the Joint National Committee on Prevention, Evaluation, and Treatment of High Blood Pressure: diuretics, beta-blockers, angiotensin-II receptor blockers, angiotensin-converting enzyme inhibitors, and calcium channel blockers. Also included were prescriptions for cardiac glycosides and other cardiovascular agents indicated to treat hypertension. Filled prescriptions that occurred before the initial diagnosis of hypertension were excluded.
Outcome measure
The outcome was semiannual medication possession ratio (MPR), a measure that tracks gaps in medication adherence by aggregating days' supply of antihypertensive prescriptions over a defined period of a calendar half year. 24 The numerator of the measure was operationalized as an individual's total days' supply of filled antihypertensive medication prescriptions during a calendar half year (ie, January 1 - June 30 [first calendar half year, or H1], or July 1 - December 31 [second calendar half year, or H2]). If the individual had an antihypertensive prescription fill prior to the first day of a given half year, the denominator was the number of days within the half year. If the individual's first antihypertensive prescription fill occurred during a given half year, the denominator was the number of days between the first day of medication supplied and the last day of the half year.
MPR was calculated by dividing the numerator by the denominator, and expressed as a percentage ranging from 0% to 100%. For individuals with multiple prescriptions, the numerator and denominator were aggregated across prescribed antihypertensive drug classes. Where the numerator exceeded the denominator within a half year, the MPR was capped at 100%, and the excess of medication days' supply was carried over into the subsequent half year. 25
Statistical analyses
The distributions of individual-level and practice-level characteristics among patients with hypertension in multi-payer PCMHs, single-payer PCMHs, and non-PCMH practices were described using counts and proportions for categorical variables, and using means and standard deviations for continuous variables. The unadjusted average MPR was calculated across patients included in each half year of the study period by practice type and by payer type. To estimate the adjusted change in MPR among individuals in multi-payer PCMHs relative to the comparison groups, a difference-in-differences (DID) analytic approach 26 was employed with patient half year as the unit of analysis.
A hierarchical linear regression model of the MPR was built with random intercepts at the levels of the patient (to account for repeated measures of MPR over the study period) and practice. The model included only patient half years with a denominator of at least 90 days and adjusted for patient's age category, sex, and Charlson comorbidity index score 27 computed annually from diagnosis codes using the algorithm developed by Quan et al. 28 From the model, DID estimates are reported as the change in average MPR, in percentage points, from the baseline half year (second half year of 2010, or 2010-H2) among patients in multi-payer PCMHs adjusted for the concurrent change among counterparts in other practice types. The first half year of the study period, 2010-H1, was considered a lookback period for confirming eligibility criteria for the analytic baseline period, 2010-H2.
All analyses were conducted using Stata Statistical Software: Release 15 (StataCorp LLC, College Station, TX). Double-sided P values are reported for estimates, and P values ˂0.05 were considered statistically significant. Study protocols were approved by the institutional review board of the Johns Hopkins Bloomberg School of Public Health.
Results
From 2010 to 2013, a total of 48,396 adult patients with hypertension from 51 multi-payer PCMHs, 51 single-payer PCMHs, and 42 non-PCMH practices were included (Figure 1). Table 1 presents descriptive characteristics of included patients by practice type. Multi-payer PCMHs and comparison groups were generally similar with respect to demographic characteristics of patients, payer mix, distribution of drug classes, and practice-level features.
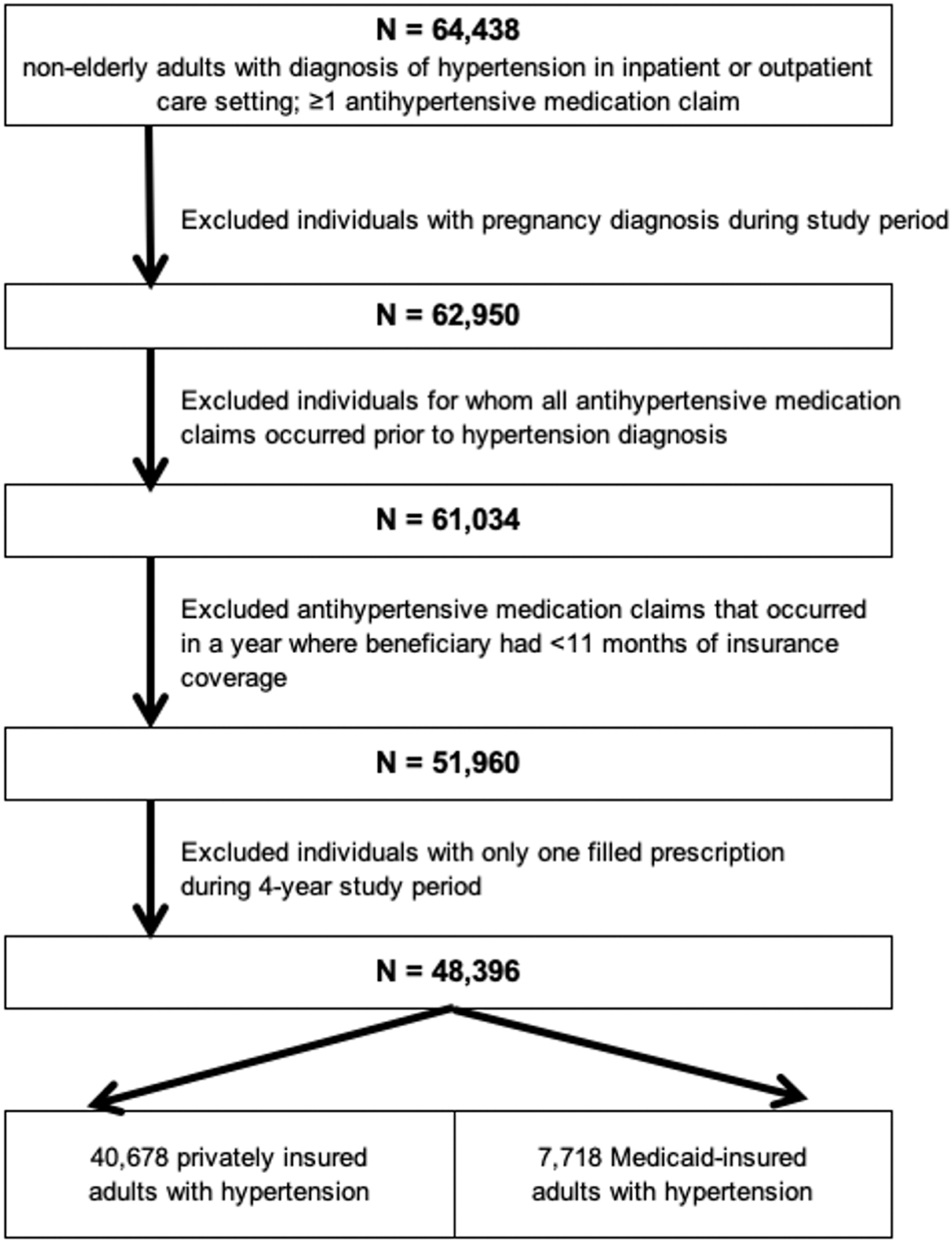
Flowchart of study inclusion and exclusion criteria. Selection criteria for patients included from multi-payer PCMHs, comparator single-payer PCMHs, and non-PCMH practices. PCMHs, patient-centered medical homes.
Characteristics of Included Patients, by Practice Type
ACE, angiotensin-converting enzyme; FQHC, Federally Qualified Health Center; HMO, health maintenance organization; PCMH, patient-centered medical home; SD, standard deviation.
A total of 157,419 patient half year observations were analyzed for included individuals. On average, patients in multi-payer PCMHs were followed for 3.4 (standard deviation [SD]: 2.0) of 8 half years, patients in single-payer PCMHs for 3.5 (SD: 2.0) half years, and patients in non-PCMH practices for 2.8 (SD: 1.7) half years. Segmented by payer type, patients insured by Medicaid generally had lower MPR than privately insured patients.
In the baseline half year, average unadjusted MPR ranged between 74.4% and 75.3% for Medicaid-insured patients, and between 85.6% and 87.4% for privately insured patients (Figure 2). Although both PCMH and non-PCMH practice types experienced a decrease in unadjusted MPR for Medicaid-insured patients during the study period, multi-payer PCMHs had higher averages than the comparison groups from the second year of the demonstration. Among privately insured patients, those in multi-payer and single-payer PCMHs had lower means for unadjusted MPR relative to counterparts in non-PCMH practices for the majority of the study period.

Unadjusted semiannual medication possession ratio for adult patients with hypertension in multi-payer medical homes and comparison practice types. Semiannual medication possession ratio was averaged across all included patients for each payer type. H1, first calendar half year (January 1 – June 30); H2, second calendar half year (July 1 – December 31); PCMH, patient-centered medical home.
For privately insured patients, the adjusted model estimated that the average MPR decreased by 9.88 percentage points [95% confidence interval: -10.83%, -8.93%, P < 0.001] during the study period among multi-payer PCMHs. Declines also were observed but greater in magnitude among single-payer PCMHs (-10.49% [-11.49%, -9.50%], P < 0.001) and non-PCMH practices (-10.87% [-12.41%, -9.34%], P < 0.001).
Relative to single-payer PCMHs, multi-payer PCMHs saw a significantly lower decrease in MPR from baseline to the third (DID for multi-payer PCMH vs. single-payer PCMH = 2.05% [0.72% - 3.37%], P = 0.002) and fifth (DID = 1.67% [0.32% - 3.01%], P = 0.02) half years of the demonstration (Table 2). There were no significant differences between multi-payer PCMHs and non-PCMH practices with respect to change in MPR among privately insured patients, except in the first half year of the demonstration (DID for multi-payer PCMH vs. non-PCMH in 2011-H1 = -2.46% [-4.20%, -0.72%], P = 0.006).
Adjusted Changes in Semiannual Medication Possession Ratio from Baseline for Adult Patients with Hypertension in Multi-Payer Medical Homes Relative to Comparison Practice Types
Estimates from multilevel linear regression models showing adjusted DID estimates, in percentage points, of change in the medication possession ratio from the baseline half year among patients of multi-payer PCMHs relative to concurrent change among counterparts in single-payer PCMHs and non-PCMH practices. The baseline is the second half year of 2010 (2010-H2). Estimates are adjusted for patient's age category, sex, and Charlson comorbidity score. The figures in brackets represent lower and upper 95% CIs for the DID estimates.
P < 0.05; ** P < 0.01.
CIs, confidence intervals; DID, difference-in-differences; H1, first calendar half year; PCMH, patient-centered medical home.
Among Medicaid-insured patients, adjusted MPR increased by 1.73% [95% CI: -0.08% - 3.54%, P = 0.06] among multi-payer PCMHs, but decreased by 5.55% [95% CI: -8.00% - -3.01%, P < 0.001] among single-payer PCMH practices, and decreased by 3.84% [95% CI: -6.70% - -0.97%, P = 0.009] among non-PCMH practices from 2010-H2 to 2013-H2. Relative to multi-payer PCMHs, average MPR decreased significantly among single-payer PCMHs during the latter half of the demonstration, with the difference ranging between 3.81% and 6.04% during the final year of the demonstration. There were no statistically significant differences in average MPR for Medicaid-insured patients between non-PCMH practices and multi-payer PCMHs.
Discussion
This study evaluated the impact of the PCMH model of primary care on improving antihypertensive medication adherence among adult patients with hypertension. To the best of the authors' knowledge, this is the first study to examine this question by comparing outcomes of this innovative model separately for publicly insured and privately insured patients in the same practices, in addition to comparing single-payer to multi-payer financing structures of this model. This study examined a large sample of patients from a diverse set of primary practices that adopted the PCMH model under the auspices of a comprehensive demonstration that promoted high fidelity to the intervention. A validated measure of medication adherence, the MPR, and rigorous empirical models were used to assess the effect of multi-payer PCMH care on patients with hypertension while controlling for relevant confounders.
Study results primarily demonstrate that practices participating in a medical home demonstration financed by multiple private and public payers performed higher on medication adherence for their privately insured and Medicaid-insured patients than single-payer medical homes. Improvements in antihypertensive medication adherence were significantly greater for privately insured patients of multi-payer PCMHs than counterparts in single-payer medical homes in 2 of the last 4 half years of the demonstration. Similarly, improvements in adherence were greater for Medicaid-insured patients in multi-payer PCMHs relative to single-payer PCMHs in 3 of the last 4 half years.
The comparative effectiveness of the multi-payer over the single-payer PCMH model was more striking for Medicaid-insured patients, with the differential impact peaking at 6 percentage points during the final year of the demonstration. Although the single-payer PCMH program had a similar incentive structure to the MMPP, a fundamental difference was that the PCMH program funded by a single private payer provided care management funds and financial incentives for only the portion of a practice's patient panel that was covered by the private insurer financing that program. Hence, providers in single-payer medical homes could not earn the rewards that multi-payer medical homes stood to gain for improvements in management and outcomes for their Medicaid-insured patients.
The merits of multi-payer financing over single-payer financing for innovative delivery models include standardization of quality requirements, reporting, and payment over a larger portion of the practice's patient population, as well as reduced administrative workload. 14 The findings of this study indicate that a multi-payer structure may be stronger motivation for providers to adopt a population health paradigm that enhances outcomes for all patients, rather than focusing on the proportion for whom incentives may be available.
This study did not find consistent evidence to support the superiority of the multi-payer PCMH model over non-PCMH care for antihypertensive medication adherence. Compared to a set of matched primary care practices that were not certified as medical homes at the onset of the MMPP, multi-payer medical homes participating in the demonstration did not perform significantly better or worse on the outcome. The null effect was observed in spite of clinical markers of hypertension control such as blood pressure measurement and blood pressure control being among the quality measures on which practices participating in the MMPP were assessed to determine eligibility for and magnitude of shared savings. 29 Present study results differ from previous work reporting that receiving medical home care was associated with between 2.2% and 3.2% improvement in adherence with antihypertensive medication. 10,11
Although it was established that the non-PCMH practices in this study were not certified by NCQA as medical homes at the onset of the demonstration, they were matched to be structurally similar to the medical homes evaluated. In fact, they were more likely than the multi-payer medical homes to report having an all-electronic medical record (EMR) system in the baseline year, indicating that these non-PCMH practices were capable of delivering some medical home functions enhanced by EMR functionality such as medication management, and electronic prescribing. 17 Medical home status of non-PCMH practices was not tracked during the course of the medical home demonstration. It is possible that some of these practices may have embarked soon after on the journey toward medical home certification or selectively adopted medical home features to improve their outcomes.
The improvements in antihypertensive medication adherence among patients in multi-payer medical homes were incremental, not immediate. Most changes did not occur till after the first year of the demonstration. Among privately insured patients, improvements in medication adherence for multi-payer medical homes surpassed concurrent changes for single-payer medical homes in the second and third years of the demonstration. Similarly, improvements in the outcome among Medicaid-insured patients of multi-payer medical homes were consistently greater than among counterparts in single-payer medical homes from the demonstration's second year.
These trends are aligned with the recurring conclusion from other PCMH evaluations that the process of transforming care delivery to implement the medical home model within a primary care practice is comprehensive, disruptive, gradual, and continuous. 30 –32 Transformation into a medical home involves changes in patient management practices, modifications to workforce composition and roles, updates to infrastructure, and significant administrative coordination for changes in payments and incentive structures. These processes also must be accompanied by continued training and sensitization of providers to the essential principles of medical home care, and managing resistance to change. Because of the time, investment, and motivation required for the medical home to be fully situated in a practice, it follows that desired patient outcomes would not be observed for a period after initial implementation.
During MMPP, participating practices were given till the end of the first year to obtain initial accreditation as a medical home. They also had to attain an advanced PCMH certification by the following year. This implies that practices would have spent the first 2 years of the 3-year demonstration in transformation to meet rigorous certification requirements. In common with other statewide PCMH demonstrations, this study's short implementation period of 3 years may be insufficient to study the long-term impact of the well-situated medical home. 33,34 Because the patient data available for this study were limited to the duration of the demonstration, it was not possible to examine whether the observed effects were sustained after the demonstration ended.
Limitations
There are limitations to the inferences presented in this study. Participation in MMPP was not randomly assigned and, although practices in the comparison groups were matched to be similar on relevant observable characteristics, it is possible that there remain unmeasured differences among the groups studied that could influence performance on the outcome measured. For example, it was not possible to assess whether practices or payers implemented supplemental interventions during the study period to enhance patients' medication adherence, such as embedding of pharmacists, or incentives for patients to fill prescriptions timely.
Because the analyses were based on administrative data sources, it was not possible to verify whether patients used the medication as prescribed, and the impact on clinical outcomes was not studied. Determination of non-PCMH status was conducted at the onset of MMPP, and the medical home status of non-MMPP practices was not actively monitored as the study period progressed. Furthermore, the impact of important patient factors on medication adherence (eg, access to pharmacies, ability to pay for drugs, use of non-medication behaviors to treat hypertension) were not assessed.
Conclusion
This study demonstrated encouraging effects of multi-payer financing of the PCMH model over single-payer financing on medication adherence for hypertension, with the former having a positive impact on patients with different insurance types. Qualitative insights are warranted to understand the mechanisms by which providers in medical homes respond to incentives from payers that may not apply to all their patients. It is crucial to investigate whether the share of a provider or group's patient panel covered by alternative payment contracts affects the care and management of their patients not included in the contract. As the PCMH movement diffuses rapidly across the nation, this knowledge will be important in securing the benefits of this innovative model for all patients.
Footnotes
Authors' Contributions
Drs. Marsteller and Khanna led the study as principal investigators. Drs. Fakeye and Hsu extracted and prepared the insurance enrollment and claims data for analysis. Drs. Fakeye and Hsu analyzed the data and produced the results. Drs. Fakeye, Khanna, Hsu, and Marsteller interpreted the results and developed the discussion points. All authors contributed to the writing of the draft manuscript. Drs. Fakeye, Khanna, Hsu, and Marsteller formatted and submitted the manuscript for publication.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.