
Abstract
The purpose of this project was to survey rural, minority, and underserved Alabamians regarding their perceptions of COVID-19 information, testing, and vaccination. Community health workers surveyed 3721 individuals from October 20–December 31, 2020. Participants came from 46 of Alabama's 67 counties (35 rural and 11 urban counties) and were largely Black (69.6%), female (56.5%), and between the ages of 40–59 years (34.8%). The majority of respondents reported that recommendations from public health agencies were easy to understand, information on COVID-19 was easy to find, and they felt confident in keeping themselves safe from infection. Most also reported they would get tested for COVID-19 if they had been exposed to someone who tested positive. Hesitancy to receive a COVID-19 vaccine was very high among all respondents; only 38.7% said they would be vaccinated. Significant differences by sex, race/ethnicity, age, and/or rural/urban status were seen for all survey items. Findings from this survey differ from other published studies and will be of interest to states with large rural, underserved, and minority populations as they tailor messaging for those most vulnerable. Findings also are now validated by Alabama's poor response to vaccine administration, which falls far short of the national vaccination rate, putting Alabamians at even greater risk. Building vaccine confidence among low vaccine populations remains challenging yet is imperative, especially for those populations with preexisting economic, social, and physical conditions that place them at continued high risk for COVID-19 infection.
Severe acute respiratory syndrome coronavirus (SARS-CoV-2), the cause of coronavirus disease 2019 (COVID-19), was first detected in the United States on January 19, 2020. Just 20 months later, more than 42 million cases of COVID-19 have been diagnosed in the United States and more than 675,000 people have died. 1 Faced with the public health challenge of our lifetime, the coronavirus pandemic has revealed the frailty of our public health infrastructure after many years of decreased funding. It also has laid bare the weak safety net for struggling families and the long-standing health and social inequities that exist in this country, especially for minority populations who have been impacted disproportionately by the virus. 2 –5 In short, COVID-19 has been a wake-up call for all of America.
There are myriad reasons why minority communities in the United States have been hit hardest by the coronavirus pandemic. These reasons – mostly related to health and social disparities – have been well documented in the literature. 4,5 Less well documented is the impact of COVID-19 in rural communities, which tend to have older populations with more underlying conditions, higher levels of poverty, and less access to health care. In southern states like Alabama, many rural counties have large minority populations, potentially making the disparities in severe COVID-19 infection starker. 6 –9 And although reports of vaccine hesitancy among population groups have been documented, 10 –12 there is a lack of published literature on the perceptions of minority, underserved, and rural populations regarding COVID-19. 6
The Alabama Statewide Area Health Education Center (AHEC) Program received Coronavirus Aid Relief, and Economic Security Act (CARES Act) funding from the state of Alabama during 2020 to conduct free COVID-19 testing in rural and underserved communities across the state. As part of this funding, Alabama AHEC recruited, hired, and trained community health workers (CHWs) from targeted rural and underserved areas to assist with accurate COVID-19 messaging in their communities. These CHWs are trusted and respected locally and have multiple social and professional points of contact that help assure AHEC's credibility in COVID-19 prevention efforts.
A training curriculum with 3 modules was created for the CHWs and placed in Google Classroom. Modules included: (1) an introduction to AHEC; (2) COVID-19 training with links to Centers for Disease Control and Prevention (CDC) resources, a variety of videos, including YouTube videos on how to make masks and wear them correctly; and (3) survey outreach (how to reach individuals, administer the planned survey, and return results). More recently, a module on COVID-19 vaccine hesitancy information was added.
A variety of supplementary materials also are posted for CHWs, including locations of food pantries statewide, a listing of COVID-19 testing sites, information from the Alabama Department of Public Health (ADPH), Veterans Affairs resources, and handouts in Spanish. An AHEC staff member monitors the Google Classroom, responding to questions and comments from CHWs, and frequently posts messages and new information for them. Completion of the training required approximately 3 hours and CHWs were required to pass a quiz on the content. Training took place during September 2020.
Anticipating there may be a potential knowledge gap about COVID-19 and hesitancy among rural, underserved, and minority populations for both testing and vaccination, AHEC developed a questionnaire that CHWs used to survey people regarding their perceptions of COVID-19 information, testing, and vaccination. These surveys were conducted as a quality improvement (QI) effort. At the time, testing was still somewhat limited and COVID-19 vaccines were not yet available. Because AHEC expected to continue its role in COVID-19 testing as well as assist with vaccine administration in these same communities once vaccines became available, the goal was to gather information from Alabama's rural, underserved, and minority populations regarding their perceptions so that AHEC could better communicate the importance of COVID-19 recommendations, precautions, testing, and vaccination.
This article provides the results of CHW surveys, information that is helping Alabama tailor messaging for vulnerable populations and that also will be useful to other states with large rural, underserved, and minority populations.
Methods
A 7-item survey was developed with Likert-scale questions on: (1) ease or difficulty understanding recommendations and precautions of public health agencies regarding COVID; (2) ease or difficulty finding information you need on COVID; (3) confidence level in your ability to protect yourself from COVID; (4) likelihood of getting tested if you had been in close contact with someone who tested positive for COVID; (5) likelihood of getting vaccinated for COVID when vaccines become available; (6) level of trust in the ADPH; and (7) level of trust in the CDC. In addition, data were collected on sex, age range, race/ethnicity, county of residence, and insurance status.
CHWs were asked to target rural, minority, and underserved individuals from their communities for the surveys. Because of social distancing requirements at the time, surveys were conducted via telephone. Initially, responses were recorded on paper forms, but this was soon changed to an online format using JotForm (JotForm Inc., San Francisco, CA). In most instances, CHWs still asked the questions over the telephone and entered the responses into the online system. Sometimes the survey link was emailed to participants if they had smartphones or computers with internet capability.
Completed hard copy surveys were sent to North Alabama AHEC and data from online surveys were stored in a password-protected secure server. The master spreadsheet was downloaded into an Excel file and JMP statistical software (SAS Institute Inc., Cary, NC) for data analysis. Data were analyzed using descriptive statistics, bivariate chi-square analyses, and multiple multinomial logistic regression analyses including sex, age, race/ethnicity and rural or urban residence as independent variables.
This QI project was submitted for review to the Institutional Review Board at the University of Alabama at Birmingham, which determined that this project is not Human Subjects Research.
Results
Between October 20, 2020–December 31, 2020, a total of 3721 surveys were completed by 82 CHWs across Alabama. Participants came from 46 of Alabama's 67 counties (35 rural and 11 urban counties). The majority of the sample (n = 3021; 81%) were from rural counties; 631 participants (17%) lived in urban counties. A small number (<2%) did not respond to this question. Responses per county ranged from 1–754. Thirteen of the state's 18 Black Belt counties, some of the poorest counties in the country, were heavily represented with 69% of the participants (n = 2568) coming from these counties. Participants were largely Black, female, and between the ages of 40–59 years (Table 1). Of note, 13% of participants reported having no health insurance, which is much higher than the 9.7% uninsured rate for Alabama reported by the United Health Foundation in their 2020 America's Health Rankings report. 13 Table 1 provides a further breakdown of the demographics of the sample.
Demographics of Survey Participants
The first 3 survey questions focused on health literacy issues and respondents' ability to understand and obtain information on COVID-19 and to protect themselves from infection. Question 1 asked how easy or difficult it is to understand the recommendations and precautions of public health agencies regarding COVID-19. While the majority of participants (n = 2,791; 75.0%) responded that the information was easy or very easy to understand, 15% (n = 568) were unsure, and 10% (n = 362) said the information was difficult or very difficult to understand. There were statistically significant differences between sex, age, race/ethnicity, and rural/urban status. Females were significantly more likely than males to find the information easy or very easy to understand (P < .0001) (Table 2). Younger individuals, those younger than age 18 and 18–24 years of age, were significantly less likely to find the information easy or very easy (P = 0.04). Most White respondents (n = 658; 80.7%) and Black respondents (n = 1,934; 74.7%) found recommendations to be easy or very easy to understand. Latinx and Other respondents were significantly less likely to report that recommendations were easy or very easy to understand (P < .0001) (Table 2). Respondents from urban areas were significantly more likely than those from rural areas to find the information easy or very easy (P < .0001).
Responses to Questions 1–3 on Understanding and Obtaining COVID-19 Information and Confidence in Protection
Question 2 asked about the ease or difficulty finding needed information related to COVID-19. Responses here mirrored those from the prior question. While 77.1% (n = 2870) of participants responded that it was easy or very easy to find needed information, females were statistically significantly more likely to find it easier than males (P = 0.003) and older individuals were significantly more likely to find it easier than younger individuals (P = 0.0109) (Table 2). White and Black respondents were significantly more likely to say it was easy or very easy to find needed COVID-19 information than either Latinx or Other respondents (P < .0001), and urban respondents were significantly more likely to say it was easy or very easy to find needed information than rural residents (P < .0001) (Table 2).
The third question asked about how confident participants were in their ability to protect themselves from COVID-19. Again, the responses were similar to the first 2 questions with most (n = 2782; 74.8%) responding that they were confident in their ability to protect themselves; 17.5% (n = 653) were unsure, and 7.7% (n = 286) were not confident. Statistically significant differences were seen in sex, age, and race/ethnicity. Females were significantly more confident than males (P = 0.0498) as were older individuals over younger ones (P = 0.0200) (Table 2). White respondents reported more confidence than Black, Latinx, and Other respondents (P < .0001) (Table 2). On this item, there was no significant difference between rural and urban respondents (P = 0.6883). Complete participant responses from survey questions 1 through 3 can be found in Table 2.
Multiple multinomial logistic regressions were further conducted to explore the different responses of question 3 by sex, age, race/ethnicity, and rural/urban residence, controlling for each other. The adjusted odds ratios (ORs) and the 95% confidence intervals (95% CIs) are illustrated in Figure 1. The multiple regression analysis suggested results similar to the bivariate analysis, with significant sex, age, and race/ethnicity differences regarding responses to question 3 after controlling for other variables. For example, Blacks were more likely to respond unsure (OR = 1.66, 95% CI 1.31–2.12) or not confident (OR = 1.47, 95% CI 1.04–2.09) than to respond confident compared to Whites, regarding how confident participants were in their ability to protect themselves from COVID-19.
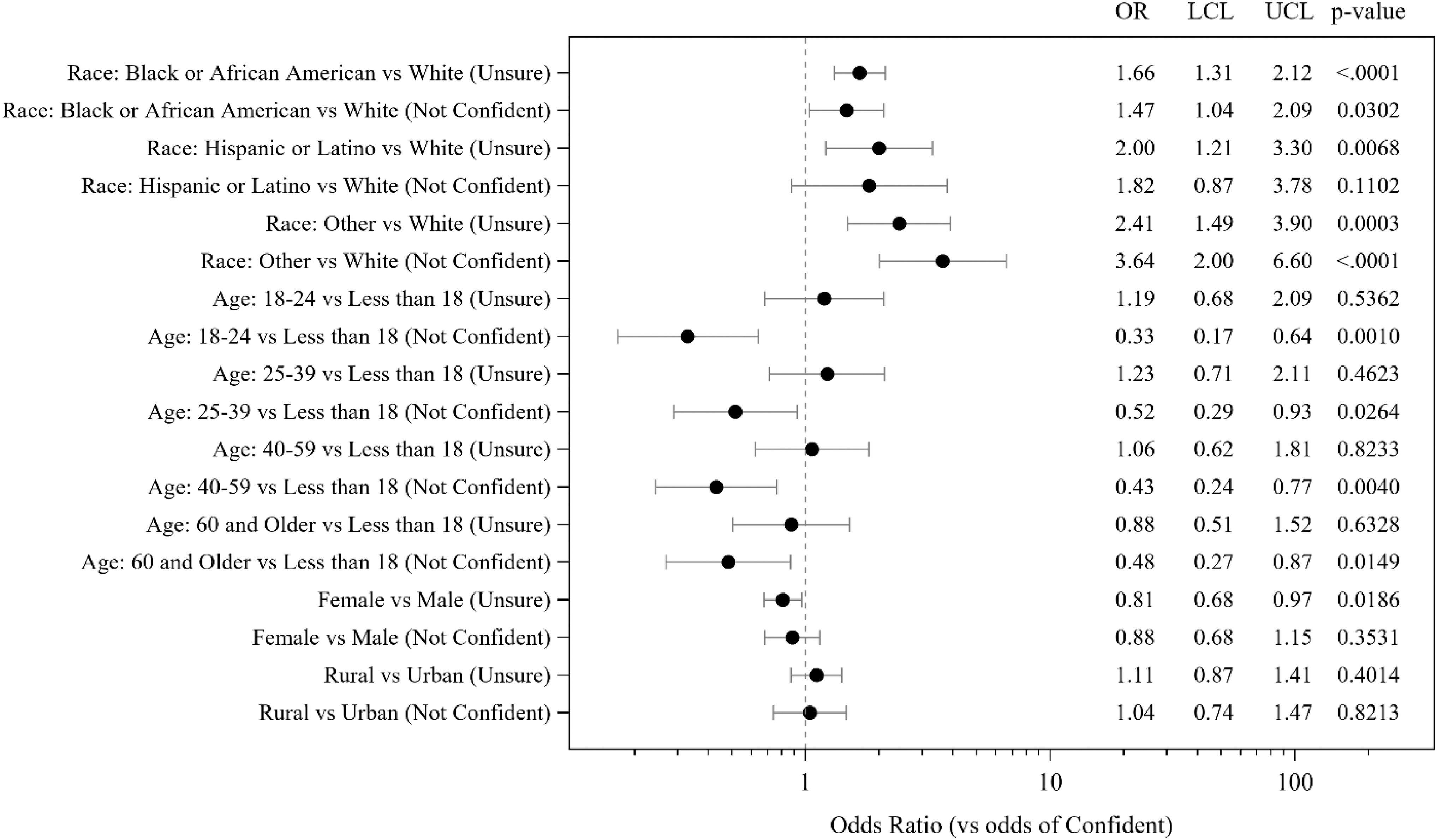
Multiple multinomial logistic regression analysis of responses to question 3. Adjusted odds ratios were calculated comparing to the odds of response “Confident in your ability to protect yourself from COVID-19.” OR, odds ratio; LCL, lower confidence limit; UCL, upper confidence limit.
Questions 4 and 5 dealt with willingness to be tested and vaccinated for COVID-19. Complete participant responses from survey questions 4 and 5 can be found in Table 3. Respondents were asked if they would be tested for COVID-19 if they became aware of being in close contact with someone who tested positive. The majority of participants (n = 2635; 70.8%) responded yes, while 20.9% (n = 779) were unsure, and 8.3% (n = 307) said no. There was no significant difference between males and females on this question (P = 0.1035). However, participants aged 60 and older were statistically significantly more likely to be tested than those of any other age group (P < .0001). Significant differences were noted by race/ethnicity with Latinx participants being far less likely to be tested than Black or White or Other participants (P = .0316) (Table 3). In fact, more than 40% of Latinx participants were unsure they would be tested and another ∼24% reported they would not be tested if they had been exposed to someone who tested positive for COVID-19. Statistical significance was also seen between rural and urban populations on this item with urban respondents more likely to be tested than rural respondents (P < .0001) (Table 3).
Responses to Questions 4 & 5 on Willingness to be Tested or Vaccinated for COVID-19
Further multiple multinomial logistic regressions were conducted to explore the different responses of question 4 by sex, age, race/ethnicity, and rural/urban residence, controlling for each other. The adjusted ORs and the 95% CIs are shown in Figure 2, Question 4. Again, the multiple regression analysis suggested results similar to the bivariate analysis with significant age, race/ethnicity, and rural/urban residence differences regarding the responses to question 4 after controlling for other variables. For example, Latinx participants were more likely to respond unsure (OR = 3.95, 95% CI 2.47–6.33) or no (OR = 3.61, 95% CI 2.12–6.13) than responding yes compared to Whites, when asked if they would be tested for COVID-19 if they became aware of being in close contact with someone who tested positive.
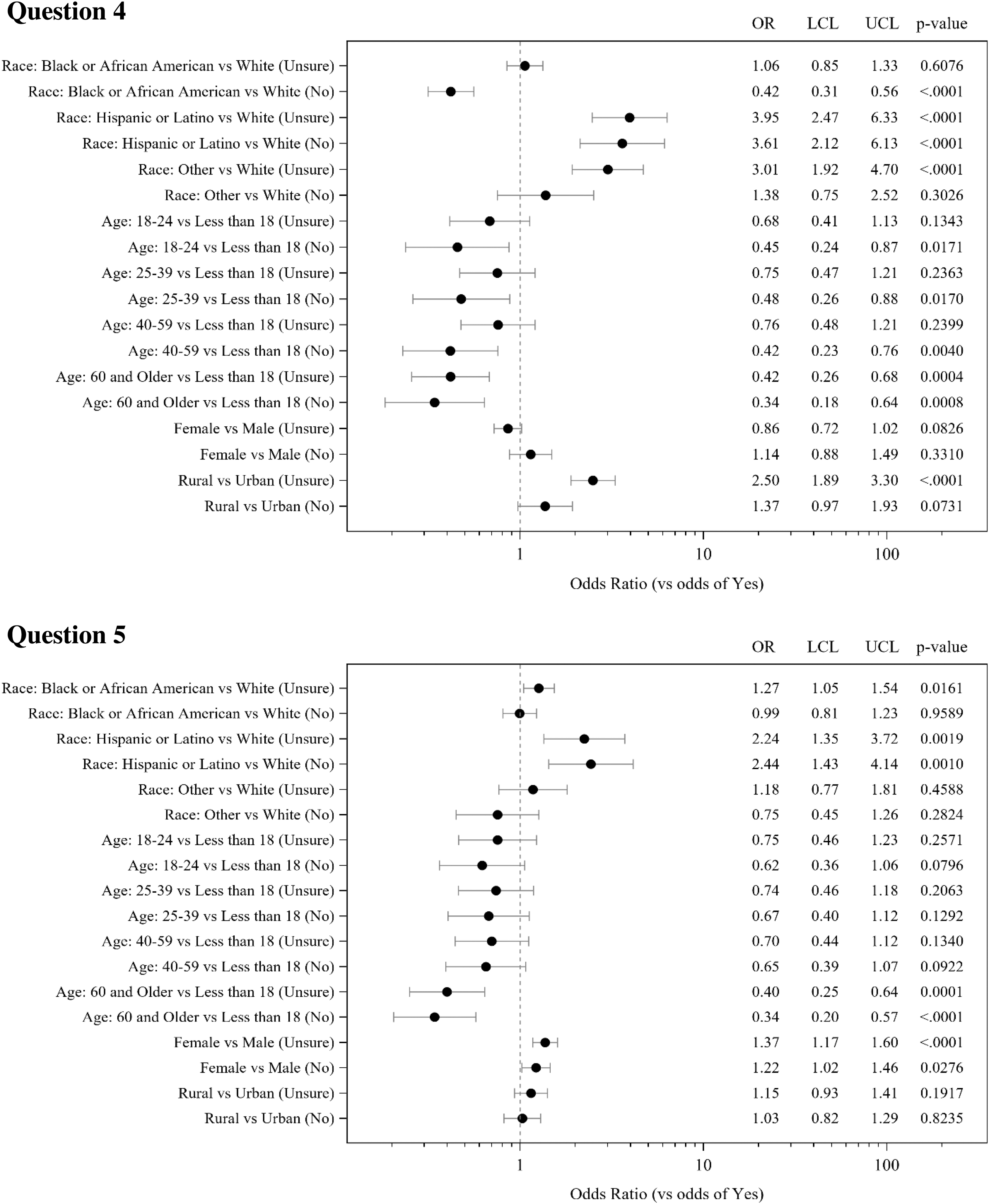
Multiple multinomial logistic regression analysis of responses to questions 4 and 5. Adjusted odds ratios were calculated comparing to the odds of a response of yes to being tested for COVID-19 (Question 4) or vaccinated for COVID-19 (Question 5). OR, odds ratio; LCL, lower confidence limit; UCL, upper confidence limit.
Question 5 asked participants if they would receive the COVID-19 vaccination, if given the opportunity to get vaccinated. It is important to note that none of the vaccines were available at the time of this survey. Overall, only 38.7% (n = 1439) of respondents said yes to this item, with 37.2% (n = 1382) unsure, and 24.1% responding no to receiving the vaccine. Males were statistically significantly more willing to receive a vaccination than females (P = 0.0004). Those aged 60 and older also were significantly more willing to receive a vaccination than any younger age group (P < .0001). Latinx participants were significantly less willing to receive a vaccine compared to Whites, Blacks, and Other (P < .0001) (Table 3). Large percentages of all racial/ethnic groups reported being unsure about being vaccinated. There was no significant difference in willingness to receive a vaccine between rural and urban respondents (P = 0.3157) (Table 3).
Further multiple multinomial logistic regressions were conducted to explore the different responses of question 5 by sex, age, race/ethnicity, and rural/urban residence, controlling for each other. The adjusted ORs and the 95% CIs are shown in Figure 2, Question 5. The multiple regression analysis suggested similar results to the bivariate analysis with significant age, sex, and race/ethnicity differences regarding the responses on question 5 after controlling for other variables. For example, Latinx participants were more likely to respond unsure (OR = 2.24, 95% CI 1.35–3.72) or no (OR = 2.44, 95% CI 1.43–4.14) than to respond yes compared to Whites, when asked if they would receive the COVID-19 vaccination given the opportunity to get vaccinated.
The final 2 survey questions were aimed at determining the level of trust participants had in state and federal public health agencies. Question 6 asked how much trust participants had in the ADPH. Two thirds of respondents (n = 2449; 65.9%) trusted the state health department while 23.9% (n = 890) were unsure, and 10.3% (n = 382) reported not trusting the ADPH. There was no significant difference between males and females (P = 0.4102). Whites (70.7%) and Blacks (65.5%) had statistically significantly more trust than Latinx and Other populations (P < .0001) (Table 4). Those aged 60 and older had significantly more trust than all other age groups (P < .0001). Rural respondents were more trusting than urban respondents (P < .0001) (Table 4).
Responses to Questions 6 & 7 on Trust in State and Federal Public Health Agencies
Responses to Question 7, trust in the CDC, were similar although more participants reported trust in the CDC (n = 2565; 68.9%). Reported trust was similar between males and females (P = 0.1829) (Table 4). Trust in the CDC was highest for Whites and Blacks. Latinx and Other populations had significantly less trust (P < .0001) (Table 4). Again, respondents aged 60 and older and those from rural areas were significantly more trusting (P < .0001 and P < .0001, respectively). Complete participant responses from survey questions 6 and 7 can be found in Table 4.
Discussion
Rural, minority, and underserved populations are frequently impacted by a variety of social determinants of health, including lower levels of education and lower incomes, which often lead to low health literacy. 14,15 This is certainly true in Alabama where up to 59% of adults suffer from low health literacy, a problem that is worse in the state's Black Belt counties. 16 Yet three quarters of participants in this survey said that recommendations and precautions of public health agencies regarding COVID-19 were easy to understand, information was easy for them to find, and they felt confident about keeping themselves safe. Mirroring the results of the 2003 National Assessment of Health Literacy, 14 women found the information easier to access and understand than men. Women also were more confident in their ability to protect themselves from COVID-19.
Urban residents found information and precautions about COVID-19 easier to understand and had less difficulty accessing information on COVID than their rural counterparts. This can be explained in part by improved health literacy and better access to health care and health care providers in urban areas of Alabama, as well as better access to broadband and internet capabilities where many people reportedly access health information. 17 White respondents were more confident in their ability to protect themselves from infection than Black, Latinx, and Other respondents. Minorities are more likely to live in multigenerational households, areas that are densely populated, and to hold more frontline “essential workforce” positions that make social distancing difficult, which could explain this difference. 4 Despite this, rural and urban respondents were equally confident in their ability to protect themselves from infection.
Both Black and White respondents reported ease in understanding and obtaining information on COVID-19, while Latinx and Other participants were much less sure. This could be because of a lack of information available in languages other than English. Younger respondents also expressed more difficulty in understanding and accessing COVID-19 content and in their ability to protect themselves. In general, younger individuals view themselves at less risk for severe infection and may not be paying as much attention to public health recommendations, which possibly could explain these findings.
Overall, most survey respondents said they would get tested for COVID-19 if they had been in close contact with someone who tested positive. Blacks were the most likely to say they would be tested (75.0%), compared to Whites (68.6%), Latinx (33.6%), and Other respondents (49.4%). These results are in contrast with a December 2020 Quest Diagnostics Health Trends nationwide study that found that 74% of Americans would either not be tested or would delay testing if they believed they needed to be tested for COVID-19. 18 However, the Quest study also showed that Latinx adults were the most likely to avoid or delay needed testing. 18 In the current survey, large percentages of both Latinx (42.1%) and Other participants (37.8%) were unsure whether they would get tested if needed. Because testing continues to play a vital role in controlling the COVID-19 pandemic, outreach to these communities in particular is needed to provide clear information from trusted sources to build confidence in the testing process.
Adults aged 60 and older were much more likely to say they would be tested, likely because this population understands they are at greater risk for severe disease, if infected. Unfortunately, rural residents reported much less willingness to be tested than urban residents. This may reflect the more limited access to COVID-19 testing seen in rural areas across the United States and Alabama as well as the barriers that exist for rural residents, including lack of transportation. Fear and misunderstanding, including the fear of contracting COVID-19 from getting tested, also may be an issue. 19 Again, education and information from trusted sources on the importance of COVID-19 testing is important in rural communities where residents are particularly at risk for severe infection.
Hesitancy to receive a COVID-19 vaccination was notable in this large survey where only 38.7% of the total respondents said they would be vaccinated, including just 19.7% of Latinx participants. These findings conflict with recent data from the Pew Research Center and others that indicate that 60%–78% of adults would definitely or probably get a vaccine and that Blacks stand out as less inclined to be vaccinated than all other racial and ethnic groups. 10,11,20 In the current survey, Blacks were no less likely than Whites to say they would get the vaccine (39.5% and 40.4%, respectively). More so than in the prior question about testing, greater percentages of all groups said they would definitely not receive a vaccine. Further, significant percentages of all racial and ethnic groups reported being unsure. This potentially “movable middle” must be a target for outreach efforts into rural, underserved, and minority communities.
In line with previous studies, adults aged 60 and older in the current survey were more willing to receive vaccine (50.5%). Females in this survey were significantly less willing and more unsure about vaccination than males. This is a surprising finding because women reported greater understanding of public health recommendations and precautions than men and they typically receive more preventive health services than their male counterparts. This finding is similar, however, to that found by Khubchandani and colleagues earlier this year. 20 There are reports from younger women about fertility concerns related to the vaccine; however, there are no published data to support this concern.
In a Kaiser Family Foundation COVID-19 Vaccine Monitoring Survey published in January 2021, 35% of rural Americans reported they probably or definitely would not get a COVID-19 vaccine, compared to 26% of urban respondents. 12 In the present survey, however, there was no difference between rural and urban respondents. Large percentages of both groups were either unwilling or unsure they would receive a vaccine (61.5% of rural participants and 58.8% of urban participants). The significant vaccine hesitancy noted in this survey could be related to a variety of reasons including preexisting vaccine hesitancy, persistent misinformation about the vaccine, lower health literacy, less interaction with health care providers, mixed messaging by federal and state officials, and medical mistrust by some populations. 19 It is important to note that this survey was conducted in Alabama, where much distrust remains as a result of the Tuskegee Syphilis Study that took place from 1932–1972.
Despite valid concerns of fear and distrust by Black populations regarding COVID-19 messaging, testing, and vaccination, 19,21 two thirds of survey respondents, the large majority of whom were Black, reported trust in both the ADPH and the CDC. While there was little media focus on the ADPH in the fall when surveys were collected, there was certainly focus on the CDC and its diminished role, which makes the CDC trust finding an interesting one. Latinx and Other respondents reported the least trust, perhaps because some may have been undocumented. Interestingly, respondents aged 60 and older and those from rural areas were significantly more trusting of both organizations. It is possible that survey respondents had little knowledge of either organization and, thus, no particular reason to distrust them.
Limitations
This project was conducted for QI purposes; therefore, the results cannot be generalized to other populations. Nevertheless, survey findings may be applicable to other states. Although the survey population was large, most participants were female, Black, and from rural counties, which could skew the results. Further, the survey developed was not validated prior to its use, which may limit the results. The first 3 survey questions focused on health literacy and the perceptions of respondents about ease or difficulty in understanding public health recommendations and precautions related to COVID-19, ability to access needed information, and confidence in keeping oneself safe from infection. Although the overall responses to these questions were quite positive, actual knowledge of public health measures or compliance with them was not measured.
Finally, CHWs were asked to target rural, underserved, and minority individuals from their communities for the surveys. No attempt was made to determine educational level, employment, income, or political affiliation of survey participants, which could have affected the results.
Conclusions
This large statewide survey of predominantly minority, rural, and underserved Alabamians, most from the Black Belt counties of the state, was conducted to assess perceptions of COVID-19 information, testing, and vaccination. Surveys were conducted for QI purposes as the Alabama AHEC had a role in COVID-19 testing in rural and underserved communities and anticipated involvement in vaccine administration in these same communities when vaccine became available. AHEC administrators understood that better understanding these perceptions would be important to the success of ongoing COVID-19 testing as well as to developing a successful vaccination strategy for groups most at risk for severe infection.
Results of this survey differ from other published studies. Most of those surveyed reported ease in understanding public health measures regarding COVID-19 and confidence in their ability to keep themselves safe from infection. Most also reported they would get tested for COVID-19 if they had been in close contact with someone who tested positive. In fact, Blacks reported more willingness to get tested than any other racial/ethnic group. Latinx respondents were least likely to get tested.
Vaccine hesitancy was great in this survey across all racial/ethnic groups, ages, and rural/urban status. The only respondents more willing than not to receive a vaccine were those aged 60 and older (50.5% said they would get a vaccine when available). Large percentages of those surveyed were unsure about receiving a vaccine. These results are now validated by Alabama's poor response to vaccine administration. Almost 10 months into the availability of vaccine, Alabama ranks the lowest in the nation in vaccinations with only 41% of the population fully vaccinated and only 52% who have had 1 or more doses of vaccine. 22 This compares to 63.9% of Americans who have received 1 or more doses and 54.8% who are fully vaccinated. 23 Older Alabamians do have the highest rate of vaccination in the state, and more women have been vaccinated than men (50.2% vs. 43.5%), but the percentages of vaccination by race and ethnicity remain low (38.2% of Whites, 39.3% of Blacks, and 37.1% of Hispanics). 24 Alabama is considered one of the most vulnerable states for further infection because of the low vaccination rate coupled with preexisting economic, social, and physical conditions that make it difficult to respond and recover from a COVID-19 outbreak. 22 As the pace of vaccination has slowed and the more contagious Delta variant is now the dominant variant causing infection in the United States, researchers are concerned about a surge in infection in low vaccine populations. 25 This includes Alabama as well as many of the states in the southeastern United States where cases and hospitalizations are rising again.
It is imperative to build vaccine confidence among populations who are disproportionately affected by COVID-19. Much work needs to be done in states such as Alabama, that have large rural, underserved, and minority populations, to promote clear and accurate messaging from trusted sources and to dispel the myths and fears that are prevalent. Targeting the “movable middle” who remain hesitant about receiving a COVID-19 vaccine is important and requires honest, respectful communication, using language to improve vaccine confidence, 26 as well as convenient and easy access to the vaccine. As mass vaccination sites across the United States are closing in favor of smaller, more local venues, finding ways to help at-risk individuals and communities make informed decisions about their health remains key to controlling the continued dire public health consequences of this pandemic.
Footnotes
Authors' Contributions
Substantial contributions to the conception or design of the work: Mr. Crozier, Mr. Christensen, Ms. Stanley. Acquisition, analysis, or interpretation of data for the work: Dr. Li, Ms. Clark, Dr. Selleck. Drafting the work or revising it critically for important intellectual content: all authors. Final approval of the version to be published: all authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: all authors.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.