
Abstract
Premedical students typically pursue undergraduate specialization in basic biological and other sciences, learning to understand living systems at a microscopic, genetic, or molecular level. However, curricula in the basic sciences do not traditionally include courses that enable students to learn about living systems at the macro level—understanding individuals within their environment, as well as understanding and managing the health of populations, especially those with underlying conditions or the underserved. This disconnect can be bridged by creating novel curricular programs intersecting medicine and business. Population health management is a multidisciplinary field that aims to improve the patient experience, reduce health care costs, and improve treatment outcomes. Though related to public health, the 2 fields differ in significant ways. Population health management emphasizes health outcomes and their measurements and seeks to improve health outcomes based on a full understanding of risk, behaviors, lifestyle, environment, and all social determinants of health. A shift in premedical education that connects the medical sciences with business requires curricular reform with the emerging field of population health management at their intersection, allowing students to be better prepared for future medical practices and to understand expectations, benchmarks, business, and economics in a new value-based health care system.
Introduction
According to a US News and World Report survey of 121 ranked medical schools, nearly 47% of premedical students accepted to medical schools in 2019 studied a major with a biological science emphasis. Nearly 24% of premedical students majored in the physical sciences. 1 However, with the most recent changes in 2015 to the Medical College Admission Test, there is increasingly more emphasis placed on topics in psychology and social science, as well as on quantitative reasoning, critical analysis, and communication.
The medical community, including the American Medical Association, has expressed the need to create programs at the intersection of medicine and business. 2 Karpman states, “if you're planning on a career in medicine, there is one subject you need to study on top of anatomy, biochemistry, and physics—business.” 3
Recently, a US News and World Report article by Ilana Kowarski stated “undergraduate majors in fields that are relevant to career success in medical practice but not frequently studied by premeds—such as business—can be assets in a medical school application.” 4
There are numerous factors motivating a curricular shift that integrates the disciplines of business and medicine; one of those is to improve the overall competency of students flowing into the valuable health care sector as well as into medical schools. Such structural and curricular innovations have the potential to tangibly improve the health care economy, and enhance the practice of medicine by training physicians who also understand the business of health.
Population health management can be a successful vehicle through which medical schools can work with business schools to create novel curricular programs that offer business skills and knowledge to premedical students.
Defining Key Terms: Public Health Versus Population Health
Although sometimes mistaken as interchangeable, there are key differences between the disciplines of public health and population health, especially in the context of this article. These differences are worth exploring because they greatly inform the choice of population health management as the point of intersection of medicine and business in the context of premedical curricula.
It is true that both disciplines share the common goals of improving the health of populations and reducing health disparities. It is more accurate to state that these 2 disciplines are more easily defined by their differences, and it is those differences that enable them to coexist and thrive as separate curricular programs at many of the top universities in the United States. 5
Public health
Public health is defined as “…what we as a society do collectively to assure the conditions in which people can be healthy.” 6 Further, as stated by the American Public Health Association, “public health promotes and protects the health of people and the communities where they live, learn, work and play. While a doctor treats people who are sick, those of us working in public health try to prevent people from getting sick or injured in the first place.
We also promote wellness by encouraging healthy behaviors. Public health works to track disease outbreaks, prevent injuries and shed light on why some of us are more likely to suffer from poor health than others. The many facets of public health include speaking out for laws that promote smoke-free indoor air and seatbelts, spreading the word about ways to stay healthy and giving science-based solutions to problems.” 7
Dr. David Nash commented on the focus of public health, noting that the “focus is certainly admirable. Clean water, vaccinations, AIDS reduction, driving 55 miles per hour… They have done more for health in society than all 140 academic medical centers combined. But the public health community [typically] ignores three important questions: What does care cost, what's the quality and safety of that care, and what are the tradeoffs that a society has to make?” 8
Population health
Population health, in contrast, is grounded in the Triple Aim framework that proposes 3 linked goals—improving the individual experience of care, reducing per capita cost of care, and improving the health of populations. 9 Bodenheimer and Sinsky later expanded the framework to the Quadruple Aim by adding a fourth aim—improving the work life of health care providers, including clinicians and staff. 10 Population health is defined in the American Journal of Public Health as “…an approach that focuses on interrelated conditions and factors that influence the health of populations over the life course, identifies systematic variations in their patterns of occurrence, and applies the resulting knowledge to develop and implement policies and actions to improve the health and wellbeing of those populations.” 11
Thus, population health and public health are complementary, but differ in this respect: population health is focused on the cost, quality, and outcomes of care among “populations” defined as every one resident in a primary geospatially defined market area served by a health care provider, or a group of patients such as a practice, ethnic groups, employees, or a group of individuals with a specific health condition. 11,12 Thus, it focuses on well-defined groups of people, but ultimately on the cost of care, quality, and outcomes of care delivery. 13
The promotion of the field of population health by the Institute for Healthcare Improvement and the Centers for Medicare and Medicaid Services has led many health care organizations to use it to describe the clinical (often chronic disease) outcomes of enrolled patients. Many clinicians and medical managers have begun to use the term population health management, that is, the iterative process of strategically and proactively managing clinical and financial opportunities to improve health outcomes and patient engagement, and reducing health disparities, while also reducing costs. 14
Curricular coexistence and its implications
Mirroring the growth of the field of population health, from an academic program perspective, population health curricula as well as population health competencies have been defined and implemented and serve to further differentiate these academic programs from programs in public health. For example, Harris et al proposed a well-defined curricular framework for the population health discipline. 15 Subsequently, the Association for Prevention Teaching and Research developed a framework that provides a common core of population health knowledge for the health professions. 16 Kaprielian et al provided a competency map for integrating population health into clinical education. 17
Not only do population health and public health curricular programs differ substantially, they can and should coexist in a complementary manner. This ability for population health programs to emerge alongside existing public health programs occurs because it is clear that the mission and focus of such academic programs in population health complement the mission and focus of their counterparts in the schools of public health. Indeed, it is actually a strength for a university to have both.
For example, The Harvard Medical School Department of Population Medicine “is a research and teaching partnership between Harvard Pilgrim Health Care and Harvard Medical School. As the nation's first medical school appointing department based in a health plan, [it is] strategically positioned to improve population health and health care delivery locally, nationally, and internationally. [Its] mission and activities are highly consonant with the National Academy of Medicine's advocacy for a national Learning Health System—one that incorporates evidence-based practices into routine care, captures new knowledge as part of the ongoing delivery of care, and then applies new knowledge in a timely manner.” 18
As noted by Tierney, in its in-depth analysis of departments of population health: “Is population health different from public health? Apparently so: five of the existing nine Departments of Population Health are in universities with Schools of Public Health. Although the definition and role of population health in schools of medicine and public health are evolving, two differences stand out: medical schools include patient management in their population health mission, and community health improvement efforts are more focused on individuals in medical schools vs. policy-focused in public health schools.” 19
With this medical and cost-oriented distinction from public health, the field of population health management has, therefore, been clearly and unambiguously defined. It thus serves as the preferred disciplinary intersection for premedical education that is fully integrated with business.
Health is a (Big) Business
To elucidate the shift that is needed in premedical curricula, it is important to consider the evolving nature of the American health care sector. Basic sciences certainly provide important educational underpinnings in premedical education for individual patients, but an interdisciplinary population health management approach that combines science with business acumen is better suited for the growing modern health care sector.
As stated by Nunn et al, “[the health care] sector is in many ways the most consequential part of the United States economy. It is a fundamental part of people's lives, supporting their health and well-being.” 20 From both business and economic perspectives, the health care sector is critically important because of its sheer size and its extraordinary budgetary, financial, and workforce implications. According to the US Bureau of Labor Statistics, the health care sector now employs 11% of American workers. 21 In fact, in the last quarter of 2017, for the first time in US history, health care has surpassed manufacturing and retail, the most significant job engines of the 20th century, to become the largest source of jobs in the United States. 22
In 2020, health expenditures totaled $4.1 trillion and comprised the largest share, among all industry sectors, of the US Gross Domestic Product (GDP) with 19.7%. 23 Over the next 10 years, health expenditures are projected to grow at an annual rate of 5.4%. By 2028, US health expenditures will exceed $6.2 trillion and are projected to comprise about 20% of the US GDP.
This growth is due to a range of factors, from new health care treatments, services, and technologies, to better coverage, higher utilization, and rising prices. For example, as a nation gets richer, spending a higher share of income on health may be optimal. 24 In addition, as the population ages, health deteriorates, and health care spending naturally rises. Also, if productivity increases faster in tradable goods such as agriculture or manufacturing than in services such as health care or education, the latter will tend to rise in relative price and as a share of the GDP. With an emphasis on improving patient outcomes, population health management offers promising and competing increases in productivity in the health care sector.
Compared with the 36 high-income member countries comprising the Organization for Economic Co-operation and Development (OECD), as a percentage of the GDP, health expenditures in the United States are twice as much as the average OECD country. 25 It is clear that the American health care sector is a massive business. This large American business faces unique challenges, which require innovative solutions.
American health care faces various critical challenges
Given its size and importance in the US economy, a well-managed and well-functioning health care sector is a prerequisite for a well-functioning economy. Although it is not hard to make the case that American health care is the worldwide leader, with its phenomenal biomedical advances, technology, research and development, workforce, facilities, etc., it is also well known that the problems with US health care are substantial. 26 For example, although the United States spends more than other high-income countries, it is not obtaining better health outcomes. 27 There are various causes of these critical challenges, which are explored in depth below; a shift toward population health management offers solutions to the inefficiencies of the system.
As stated by Sainfort, “[h]ealthcare providers and healthcare systems have common fundamental goals—improving clinical and health outcomes, expanding and facilitating access to all health care services across the full continuum of care, and optimizing cost and efficiency. The ability to achieve these goals, however, is severely constrained by a range of critical challenges. These include, but are not limited to, an aging population, an increasing burden of chronic diseases, payment and delivery systems with misaligned incentives, and government policies and regulations that, at times, can be cumbersome.” 28
What has made tackling these challenges even more difficult is the disjointed and inefficient nature of how health care is delivered. Health care practitioners operate in health care systems that have traditionally rewarded volume of care over value of care. Although there is a push to move away from fee-for-service (FFS) or procedure-based payment and delivery systems to focus on value-based systems, the overall system remains typically highly fragmented, siloed, and disconnected—leading to inefficient, uncoordinated care and a waste of scarce resources.
In a recent analysis, Tikkanen and Abrams assessed US health care system spending, outcomes, risk factors and prevention, utilization, and quality, relative to 10 other high-income countries and concluded 4 major points. 29 First, the United States has the highest chronic disease burden and an obesity rate that is 2 times higher than the OECD average. Americans also had fewer physician visits than peers in most countries, which may be related to a low supply of physicians in the United States. Third, Americans use expensive technologies such as magnetic resonance imagings, specialized procedures, and hip replacements more often than our peers. Finally, compared with peer nations, the United States has among the highest number of hospitalizations from preventable causes and the highest rate of avoidable deaths. 29
The health care system experiences high levels of unnecessary care. There are issues of overprescribing of medications that sometimes leads to addiction or drug resistance. Persistent risk of infection and preventable readmissions in hospitals linger. Economic inefficiencies are caused by mismatched provider incentives and payment systems in addition to misaligned pharmaceutical, medical devices, and industry practices and pricing. There are wide disparities in patient access to and quality of care as well as a general lack of preventive focus on the social and behavioral determinants of health. In short, the current health care system is struggling to deliver high-quality, affordable, and easily accessible care that maintains and/or returns people to fuller, more productive lives.
Key trends in the American health care system
There are 5 key trends revealed in a critical analysis of the American health care system that students enrolled in a premedical program should know about; a discussion of inefficiencies in the health care system would be incomplete without acknowledging the influence of these trends on the practice of medicine. These trends are an aging population, a prevalence of chronic conditions, millions of uninsured Americans, notable waste in the US health care system, and imbalanced determinants of health, all indicative of the criticality of population health management (summarized in Table 1). These trends lead to a few key conclusion, notably that the evolving health care sector is projected to continue growing alongside a concerning expansion in economic waste and inefficiency.
Five Key Trends in the American Health Care System
Health is influenced by many different factors—clinical care, health behaviors, socioeconomic factors, the physical environment, and genetic predisposition. 30 Although health is often thought of in terms of diagnosed medical conditions, only about 10% of the variability in life expectancy is associated with health care. 31 Over 40% of health outcomes are associated with health behaviors 32 and another 40% are explained by nonmedical factors such as social determinants and economic and environmental factors, along with genetic factors.
In addition, modifiable risk factors contribute substantially to overall health care expenditures. Risk factors are associated with 25% of total expenditures. 33 As shown in the widely used Wisconsin County Health Rankings Model 34 (Fig. 1), the greatest opportunities for policies and programs to improve health and reduce premature death are modifiable behavioral risk factors as well as social determinants of health.
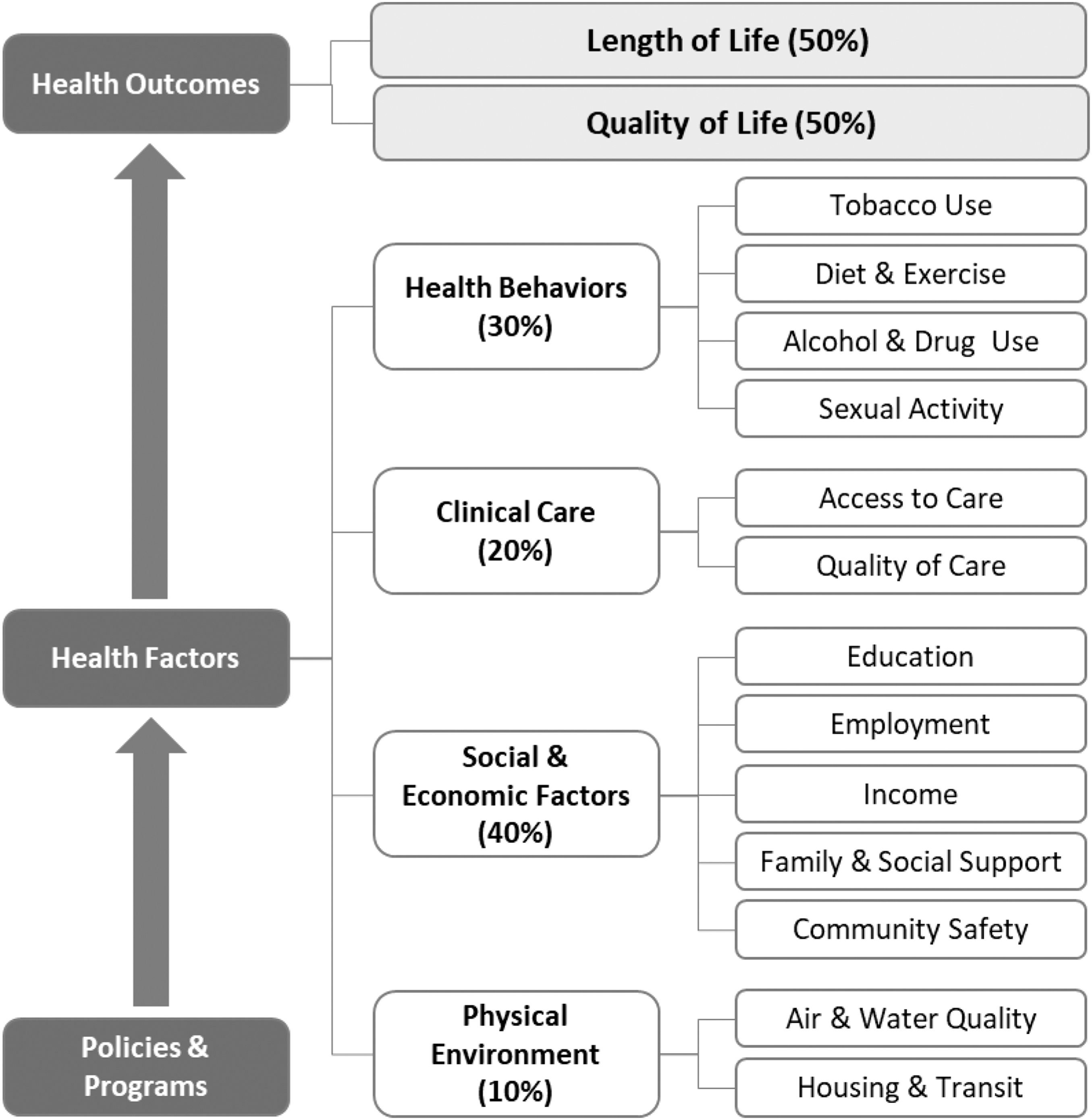
County health rankings model.
Intersection of Medicine and Business: Population Health Management
The challenges faced by the US health care system are substantial. Solutions to these challenges are complex. From a business and population health perspective, possible solutions are at least 4-fold. 26 First, eliminate or substantially reduce waste in the health care system. Second, slow the rate of growth in health care spending. Third, spend the resources allocated to health care more efficiently. Fourth, reduce modifiable behaviors, improve access to and use of health services, and address upstream social determinants such as education, income, social and welfare services, affordable housing, job creation, labor market opportunities, and transportation. 35
That is, US society must (1) address social determinants, (2) modify/reduce risky behaviors, and (3) realize greater value from the resources dedicated to health care. These principles and efficiency are guiding principles of population health management.
Value in health care is defined as outcomes relative to costs, and as such encompasses efficiency. 36 The Institute of Medicine has developed a widely accepted approach that describes high-value health care as safe, timely, effective, efficient, equitable, and patient-centered—STEEEP for short. 37 The Institute for Healthcare Improvement later translated this into a framework for action, the Triple Aim, which is made up of better patient outcomes, improved patient satisfaction, and lower costs. 9 The Triple Aim has since been expanded to the “Quadruple Aim,” which adds physician and health care professional well-being to the equation. 10
As described by Sainfort et al, 38 the health care system needs to move from a volume-based, FFS model of care delivery and payment where providers are paid per person per service to a value-based system that provides differential payments based on measures of value, that is, clinical outcomes and quality divided by cost. Reimbursement can be tied to specific performance criteria or can be negotiated through shared risk contracts. Value-based models of care, such as population health management, are heavily outcome focused and tend to be more integrated along the care continuum. Volume-based, FFS systems of care, in contrast, tend to be focused on service, independently of outcome, and tend to be more fragmented. 39
Achieving value in health care and successfully managing the health of populations require a wide range of interested parties to focus most notably the health and well-being of the patients they serve. Future success mandates achieving a collection of important goals that speak of the business of health, meaning they collectively lead to improved outcomes and reduced costs: cost accounting, measurement of health outcomes and quality, coordination of care, waste reduction and productivity improvement, business efficiencies, patient centeredness, and effective population health management.
Every organization's future success in the health ecosystem depends on redefining the health care model, which includes intentionally focusing on best business practices to achieve these high-value goals. 40 Put differently, the new mindset needed to produce a meaningful value-based health care system is one that augments medicine with business. Population health management is a successful vehicle through which medical schools can work with business schools to create curricular programs that offer novel and needed preparation for premedical students in the business of health.
Such a complex shift presents an opportunity for developing and implementing novel premedical educational programs at the critical intersection of the business of health and medicine, that is, population health management. With such programs, it would be possible to train a new generation of clinicians equipped with the skillsets and knowledge necessary to transform the current complex health care system into a true value-based and value-driven health system. Such skillsets and knowledge require a unique understanding of population health and the business of health, in addition to medical science.
A curricular shift with population health management at the intersection of medicine and business provides a comprehensive, flexible, transdisciplinary solution, exposing students to the full continuum of the US health ecosystem—taking a look at the upstream, midstream, and downstream factors impacting population health and health care delivery in the United States. Such programs would prepare tomorrow's clinical leaders to be agents of change who will develop innovative approaches to successfully tackle health and health care management challenges of today and tomorrow.
The proposed curricula will also prepare students to enter the health care industry in management positions, including analytical and administrative leadership positions. According to the Bureau of Labor Statistics Occupational Outlook Handbook, employment of medical and health services managers is projected to grow 42% over the next 10 years, much faster than the average for all occupations (7%). 41 Modern premedical students with a population health and business focus will be able to find employment across all job types within the health ecosystem.
The proposed novel curricula are just examples of innovative pathways that can be used to better align premedical and medical education with the nation's health priorities and challenges. 42 Other approaches can focus on social and behavioral sciences, health systems sciences and engineering, and/or health analytics and informatics.
A Framework for a Premedical Curriculum at the Intersection of Medicine and Business
Although various population health programs are emerging at the graduate level, very few programs exist within the premedical curricular sphere. There are currently very few bachelor of science (BS) degree programs in population health or population health management. The Oregon Institute of Technology was the first university, in 2015, to create a BS degree in population health. 43 Since then, there has been a handful of programs launched.
A framework for effective novel curricula
Population health management is a successful vehicle through which medical schools can work with business schools to create novel curricular programs that offer business of health knowledge to premedical students. An effective population health management curriculum combines the premedical core courses in basic sciences and general education with a core of population health courses alongside a business concentration. Figure 2 illustrates 2 parallel population health management curriculum plans—1 based in business and the other based in medicine—that fully meets premedical requirements and thus fills a curricular gap for premedical education where little emphasis is traditionally placed on population health and/or business.
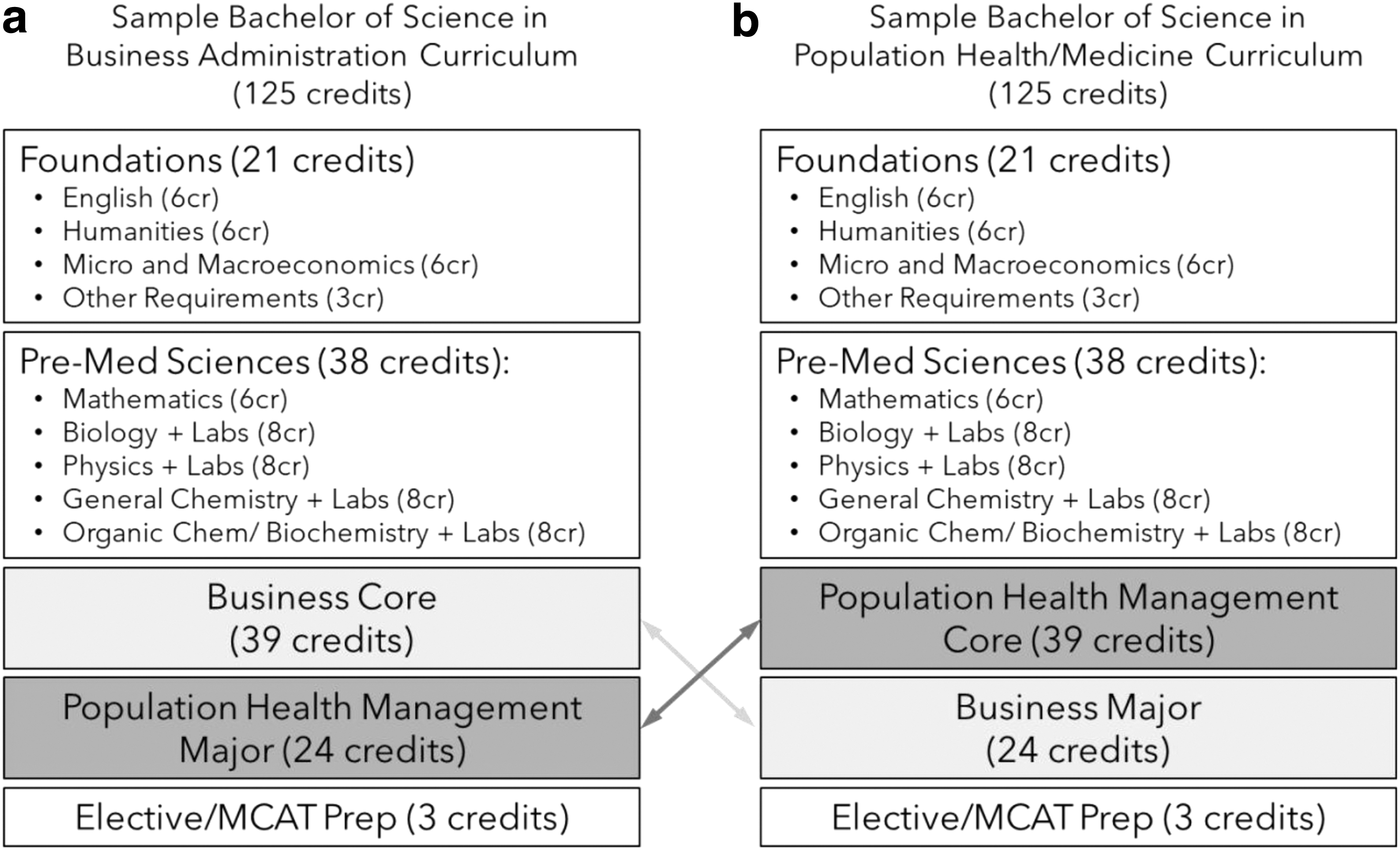
Sample curricula for
An effective and comprehensive population health curricular framework was proposed by Harris et al. 15 This framework is grounded in 6 key population health domains, combining a population health science core with a foundation in the business of health. The 6 domains and sample topics depicted in Figure 3 provide an operational guide for developing and implementing novel, comprehensive curricula.
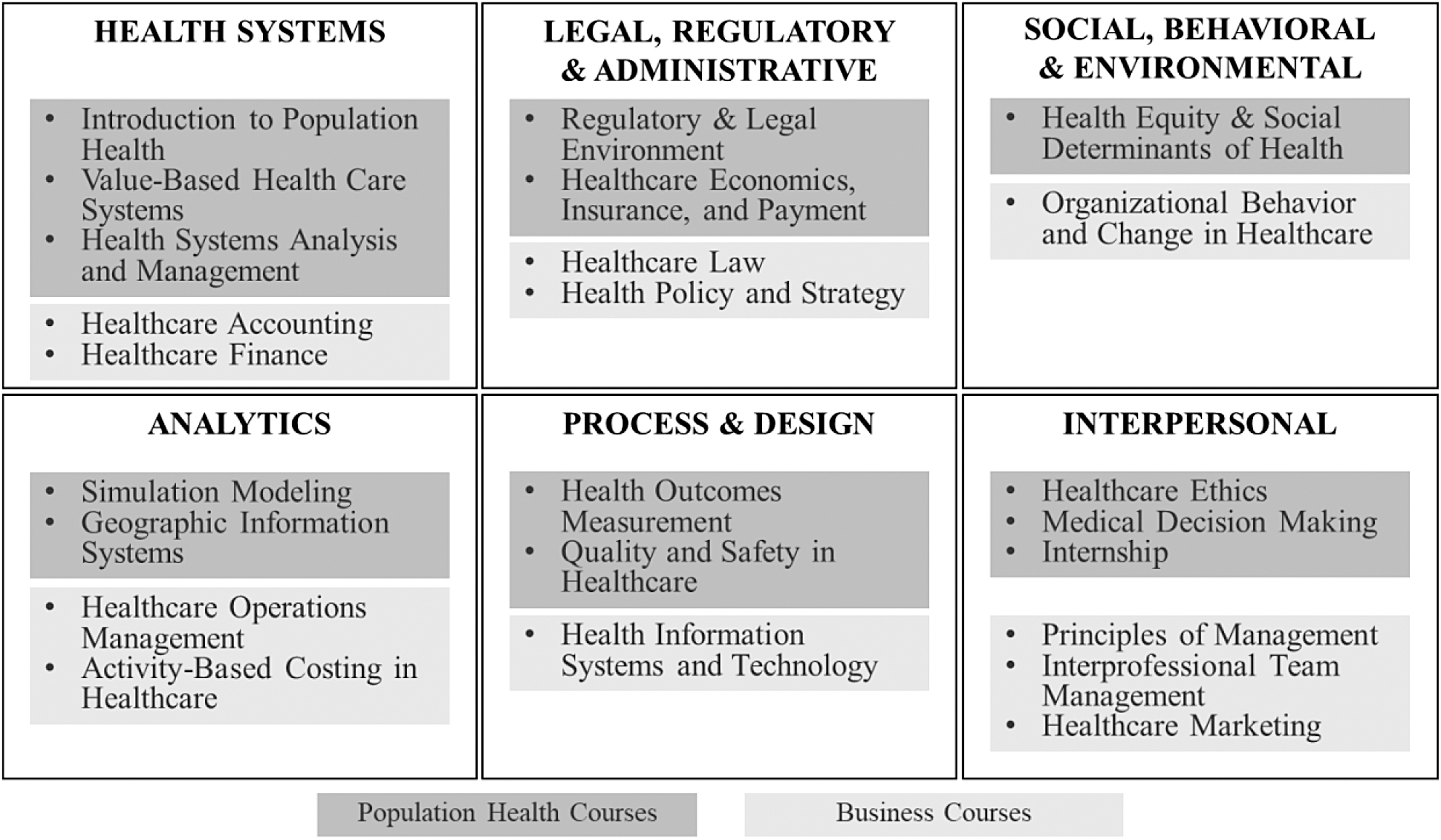
Six curricular domains and examples of courses for a population health management program.
By studying health systems, students develop a practical understanding of value-based health care systems. Legal, regulatory, and administrative topics combine business law fundamentals with important regulatory, legal, and insurance aspects of care. A third domain, the social, behavioral, and environmental determinants of health, informs students about influential determinants of health while also providing them with the business acumen to carry out organizational change to improve the system. With an emphasis on improving patient outcomes, a strong decision making and modeling core in analytics is also vital. Finally, process design and interpersonal skills provide students with the skills to manage, market, and measure outcomes.
Students with the mentioned coursework will be leaders in their field by combining an ability to recognize system inefficiencies with the interpersonal and organizational skills to effectively combat that efficiency. When paired with the core basic sciences in a premedical curriculum, population health management students will have a diverse skillset to become effective agents of positive change. The proposed curriculum can provide a needed pipeline of new students into numerous fields within the health professions including allopathic medicine, osteopathic medicine, dentistry, optometry, pharmacy, and other health care programs.
Conclusion
There must be a shift in the curricular path toward medical school. A shifting and modernizing health care market recognizes that (1) the basic sciences, as an exclusive pathway to medicine and other health professions, constitute a dated concept and (2) awareness and understanding of population health management along with business acumen have become critically important to all health care delivery organizations in today's competitive and rapidly changing health care environment. A twin-track approach to premedical education as shown in Figure 2 can serve as a national model for how to create new premedical curricula at the intersection of medicine and business, preparing students who aspire to medical school to have high potential to becoming effective and innovative practicing physicians and health care administrators.
Footnotes
Authors' Contributions
François Sainfort: conception and design, literature review, drafting the article for critically important intellectual content, and final approval of the version to be published.
Julie A. Jacko: substantial contributions to conception and design, drafting the article, and final approval of the version to be published.
Katherine Cohen: literature review and drafting portions of the article.
Andrew Rosman: important contributions to conception and design, drafting the article, review, and final approval of the version to be published.
Johannes Vieweg: important contributions to conception and design, drafting the article, review and final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.