
Abstract
This study aimed to determine whether there are disparities in the utilization of home-based care services according to income level among people aged 75 years or older in Japan. The research team used administrative claims data from April 2014 to March 2018 for people aged 75 years or older in Fukuoka Prefecture. Subjects were categorized according to income level using medical insurance claim data. Associations between income level and usage days of inpatient care, outpatient care, home medical care, and usage number of home-based long-term care (LTC) services were evaluated. Furthermore, medical and LTC costs were evaluated and adjusted for gender, age, and level of LTC needs. The team used generalized linear models (GLMs) to estimate medical and LTC services utilization, as well as the potential influence of gender, age, care needs level, and death as risk factors. The study analyzed 31,322 subjects, among whom 17,288 were in low-, 12,755 were in middle-, and 1399 were in high-income groups. The results of GLMs showed the number of home medical care days was 59.45, 62.24, and 69.66 days for users from low-, middle-, and high-income groups, respectively. Correspondingly, the number of home-based LTC services used was 668.84, 709.59, and 833.14 times. This study suggests that older adults with lower incomes had relatively low utilizations of home-based care services and high utilizations of nonhome-based LTC services. Policymakers should implement policies focused on people who need care to tackle socioeconomic inequalities in home-based care.
Introduction
The dramatic increase in the population aged 65 years and older is a global social phenomenon faced by the majority of countries. 1 This age group is projected to reach 1.4 billion people by 2030 and to exceed 2 billion by around 2050. 2 Japan is facing one of the most rapidly aging societies in the world, with adults over 65 years accounting for 28.70% of the entire population in 2020, and this percentage is expected to surpass 30% in 2025. 3
Japan has 3 major public health care insurance systems that provide universal coverage. 4 The Employees' Health Insurance system (59.00% of the population), the National Health Insurance system for individuals under 75 years of age (27.00% of the population), and the late-stage medical care system for individuals aged 75 years or over (12.70% of the population). In 2008, the Japanese government established the late-stage medical care system as a new, independent health insurance scheme to maintain the universal insurance system and make it a sustainable insurance system for the future. 3
The long-term care (LTC) insurance system was introduced in 2000, thus making it easier for individuals certified as needing LTC to use home and community-based services. Services provided under this system aim to prevent decline of functional level, thus allowing elderly people to live independently in their homes for as long as possible. 5 In brief, Japan's insurance system for older adults is divided into LTC insurance and medical insurance that categorizes those aged 65–74 years as “early-stage elderly” and those aged 75 years and older as “late-stage elderly.” Correspondingly, the coinsurance rates for medical and LTC services are generally 10% for people aged 75 years or older, and up to 30% for high-income earners based on established income criteria. 4
In view of the Japanese government policy on aging, the current focus is on the “late-stage elderly.” This is because the rates of medical and LTC services utilization are significantly higher with late-stage elderly when compared with early-stage elderly. 6 The average annual medical expenditure in 2018 was JPY 553,000 (USD 5246.68) for early-stage elderly patients and JPY 910,000 (USD 8633.78) (1.65 times higher) for late-stage elderly patients.
In contrast, the average annual LTC expenditure was JPY 50,000 (USD 474.38) for early-stage elderly patients and JPY 480,000 (USD 4554.08) (9.60 times higher) for late-stage elderly patients. 6 Late-stage elderly patients tend to be relatively frail and have multiple chronic conditions that require frequent use of both medical and LTC services. 7 Moreover, the number of people aged 75 years or older is projected to increase remarkably and should reach nearly one-fifth of the population by 2025 in Japan. 3
To efficiently provide integrated care for these individuals, Japan has implemented the Community-based Integrated Care System (CICS), with the aim of moving away from the conventional hospital-centered health care delivery system toward a system that is focused on patients' residences and local facilities. 8 The CICS comprehensively provides medical care (which is provided at medical facilities), home care (which is provided at a patient's own house or nursing home by medical professionals), and LTC services such as day care at LTC facilities or home visiting by care workers, in addition to preventive care and daily living support. These services enable older adults to “age in place” until the end of life, even when they become increasingly care dependent. 9
It has already been confirmed through previous studies that the use of home-based care reduces the number of hospitalization days for older adults. 10,11 Kim et al showed that as the system for providing home medical care for older adults is further strengthened, the use of hospitalization significantly decreased, the rate of home-based end-of-life care increased, and the rate of death at medical institutions decreased. 10 The findings suggested that the role of home-based care services is a critical component in the construction of CICS, which is a policy issue for Japan's aging society.
Also, Tomita et al found that users of home- and community-based services were less likely than nonusers to be hospitalized or institutionalized. 11 Several studies conducted in the past have also confirmed that home- and community-based services influence the utilization of medical and LTC services among older adults, but studies on the factors that influence the use of home- and community-based services have been rarely conducted.
In contrast, socioeconomic status is an important determinant of health, as poverty or lower income is one of the most important components or representation of lower socioeconomic status. 12 Therefore, considering income disparity as a factor that affects the utilization of health care services, it is necessary to identify how income disparity affects health care services utilization, especially home-based services among older adults.
There is a body of literature on the effect of income level on health care services utilization. 13 –16 Fujita et al analyzed the effect of income for the 0–74 years old population in Japan on the utilizations of medical care, and found that lower income groups had a significantly higher rate and longer episode of hospitalization, with higher utilizations of outpatient care. 13 Hamada et al examined medical and LTC insurance claims data and found that older adults with low income were more likely to be functionally dependent, as they were associated with fewer physician visits, had longer hospital stays, and had higher total expenditures. 14
Also, in a number of countries, hospitalization and institutionalization have been used as outcome measures to observe the impact of preventive interventions such as education, counseling, and evaluation, 15,16 but studies on the effectiveness of home-based care services have been limited. Moreover, the actual differences in access to home-based care, not only medical but also LTC services, owing to income disparity have not been sufficiently clarified. In addition, it is necessary to establish integrated data of medical insurance and LTC insurance to analyze the use of home-based care services for adults aged 75 years and over, who have relatively high utilization of medical and LTC services.
However, owing to the separate implementation of the medical and LTC insurance systems and the absence of common personal identification numbers in the health care system, a limited number of studies had hitherto evaluated medical and LTC services together. 17 Therefore, the purpose of this study is to verify whether there is a difference in the utilizations of health care services, especially home-based care services, among those aged 75 years or older according to income level by integrating and using the medical insurance and LTC insurance claim data.
Methods
Database
The study was conducted using data from a medical claims database and an LTC insurance claims database provided by the Fukuoka Prefecture Association of Late-stage Elderly Healthcare. Medical claims included information on patient characteristics, medical treatments, disease diagnoses, and medical expenses for all individuals who received insurance-covered care. 18 LTC insurance refers to the public insurance for older adults aged ≥65 years and adults aged ≥40 years with specific diseases. These claims include information on LTC service utilization and the corresponding expenses for all individuals with certified care needs.
Under the LTC insurance system, care needs are categorized into 7 levels (support needs levels 1–2 and care needs levels 1–5), with increasing levels signifying higher degrees of dependence. 18 The certification process starts with an initial assessment conducted mainly by a trained local government official or by a private care manager's referral from the government, who visits the home to evaluate nursing care needs using a national standardized questionnaire on current physical and mental status (73 items) and use of medical procedures (12 items). 18
To maintain patient data confidentiality, the administrative claims data were deidentified by constructing specific databases using a workstation with no connection to any networks.
Study design
This retrospective cohort study used claims data from April 2014 to March 2018. As of April 2014, the Fukuoka Prefecture Latter-stage Elderly Healthcare Association had 574,202 beneficiaries aged 75 years and over. 19 The study subjects were Fukuoka Prefecture residents aged 75 years and older with certified care needs of level (CNL) 1 or higher in April 2014 who used home medical care between April and June 2014.
To meet the objective of this study, that is, to examine the utilization of medical and LTC services according to income class, authors used information on the income category of insured individuals specified in the medical claims database. The medical claims database included the following income categories: low income 1, low income 2, modest income, and income comparable with income of the current workforce. These categories are applied by insurance associations operated in all prefectures in Japan. 20
In this analysis, subjects classified in the 2 former categories were designated as the low-income group, and those with modest income and income comparable with that of the current workforce were designated as the middle- and high-income groups, respectively. The exclusion criteria applied to people who have migrated to other prefectures during the study period, duplicated data in the CNL and income categories on the medical claims database as of April 2014.
The main indices of this study were utilizations of home-based medical care and LTC services over a 4-year period against income disparity. The team also examined the number of days that subjects received inpatient and outpatient care across the 3 groups. Costs for inpatient care, outpatient care, home-based medical care, prescription, home-based LTC, and other (except for home-based services) LTC services were calculated for each group. Costs were converted from Japanese yen to US dollars using the 2017 purchasing power parity rate (USD 1 = JPY 105.40).
Information was obtained on subject gender, age, and CNL as of April 2014. Age was divided into 4 categories (75–79, 80–84, 85–89, and ≥90 years). The CNL included in this study were levels 1 to 5 (with level 5 representing the highest level of dependence).
Statistical analysis
The distributions of gender, age, CNL, and death were examined across the 3 income level groups.
The research team calculated the mean number of annual days of inpatient care, outpatient care, home-based medical care, and utilization counts of home-based LTC services as well as the mean annual costs for inpatient care, outpatient care, home-based medical care, drug prescription, home-based LTC services, and other LTC services for each income level group. The intergroup differences were compared using the analysis of variance. Each subject's services utilization was calculated over the number of years a person lived during the study period, and annual utilization rates per person-year of observation were estimated. This method allowed the inclusion of data from subjects who died during the study period, which was useful because the study population comprised individuals with an elevated mortality risk due to advanced age and certified CNL.
To evaluate the influence of income disparity on the use of medical and LTC services, the team constructed generalized linear models (GLMs). Here, the dependent variables were the number of inpatient care days, outpatient care days, home medical care days, and utilization counts of home-based LTC services, as well as the costs for inpatient care, outpatient care, home-based medical care, drug prescription, home-based LTC services, and other LTC services. The exposure of interest was the income disparity. The covariates were gender, age, CNL, death, and the number of years the participant lived.
The dependent variables data were highly skewed and overdispersed. Thus, analyzing these data using a conventional regression method might violate the data normality assumption. Furthermore, the data containing the number of days are commonly regarded as a “count” variable, and the use of statistical techniques based on normal distribution might not be appropriate. 21,22 Many researchers have suggested that the use of the GLM by assuming such data has a negative binomial or a Poisson distribution. 23 –25 In contrast, the use of GLM with a gamma distribution is recommended when analyzing data involving health care costs. 26,27
In this study's preliminary analyses, dependent variables containing the number of days were fitted in 2 separate models: GLM with a negative binomial distribution and GLM with a Poisson distribution. Diagnostic statistics, however, identified GLM with a negative binomial distribution as providing better estimates than the model with an assumed Poisson distribution. The results of the analysis presented in this study are, therefore, based on the estimates of GLM with a negative binomial distribution with log-link function and robust standard errors, for the analyses involving the number of days. In contrast, for the results of analyses involving care costs, the estimates of GLM with a gamma distribution with log-link and robust standard errors are presented.
The marginal means of the dependent variables were calculated to indicate the estimated values of number of care utilizations and costs for the examined care services. These were calculated by substituting the mean of the estimates into GLMs with a negative binomial distribution for care days and a gamma distribution for care costs.
Because the patterns of use for medical care and LTC services would be markedly different from those at the terminal stage, the team constructed pooled cross-sectional time-series panel data by excluding individuals who died during the observed period. The team conducted Hausman–Taylor estimation 28 and found that the random effects estimation fits in this study model. According to Bell et al, 29 random effects models are readily extendable, with random coefficients, cross-level interactions, and complex variance functions. The advantages of within–between random effects over the more restrictive fixed effects are at odds with the dominance of fixed effects as the “default” option in a number of social science disciplines.
SQL Server 2014 was used to extract the data, and Stata, V.14.2, was used for all analyses.
Results
The study subjects' characteristics by income levels are summarized in Table 1. The included subjects were 31,322 Fukuoka Prefecture residents who used home medical care between April and June 2014, as well as being 75 years or over and having a CNL of 1 or higher as of April 2014. The follow-up on the utilizations of medical and LTC services by the subjects was carried out from April 2014 to March 2018. The subjects were classified into a low-income group with 17,228 subjects, middle-income group with 12,755 subjects, and high-income group with 1339 subjects who had both medical claims data and an LTC insurance claims data.
Comparison of Characteristics by Income Level
“Death” refers to subjects who died during the study period.
CNL, care needs level; SD, standard deviation.
The team observed significant intergroup differences in gender (P < 0.01) and age (P = 0.03). However, there were no significant differences in care needs level (P = 0.18) or death (P = 0.63). During the 4-year study period, 47.24% of the subjects died; the low-income group had the highest percentage of deaths (50.03%).
The distribution of medical and LTC services utilization per person-year across the groups is given in Table 2. The mean usage days of inpatient care showed no significant differences across the 3 groups (P = 0.36): low- (31.89 days), middle- (36.38 days), and high-income group (34.95 days). Meanwhile, there were significant intergroup differences when the number of days was categorized into outpatient care, home-based medical care, and utilization counts of home-based LTC services.
Medical and Long-Term Care Utilization Per Person-Year by Income Level
Care costs were converted from Japanese yen to US dollars using the 2017 purchasing power parity rate (US$1 = 105.40). The values were calculated over the number of years each subject lived during the study period and are reported here as the annual rates per person-year of observation.
LTC, long-term care.
The mean annual number of outpatient care days was highest in the high-income group (16.14 days), followed by middle-income (13.31 days) and low-income groups (12.95 days). The mean annual usage days of home-based medical care was highest in the high-income group (23.93 days), followed by middle-income (21.02 days) and low-income groups (20.65 days). The annual usage number of home-based LTC services used was also highest in high-income group (299.22 times), followed by middle-income (243.91 times) and low-income groups (225.08 times). The mean annual costs showed similar results as the number of care utilizations.
The mean annual inpatient care costs were highest in the high-income group (USD 10293.78) followed by middle-income group (USD 10192.14), and lowest in the low-income group (USD 8746.90), but there were little differences across the 3 groups (P = 0.03). The mean annual outpatient care costs were highest in the high-income group (USD 1444.95) and lowest in the low-income group (USD 904.17). The mean annual home-based medical care costs were highest in the high-income group (USD 3940.30), followed by middle-income group (USD 3512.79), and lowest in the low-income group (USD 3144.16).
The mean annual prescription costs were highest in the high-income group (USD 2498.76) and lowest in the low-income group (USD 2044.56). The mean annual home-based LTC home service costs were also highest in the high-income group (USD 12467.87) and lowest in the low-income group (USD 9455.34). In contrast, costs for other LTC services were highest in the low-income group (USD 14116.09) and lowest in the high-income group (USD 11234.77).
Table 3 gives the marginal means estimated from the GLMs evaluating the associations of income disparity with medical and LTC services utilization over the study period. The number of inpatient care days was highest in the middle-income group (101.70 days), followed by high-income (97.81 days) and low-income groups (95.97 days). The number of outpatient care days was highest in the high-income group (44.62 days), followed by low-income (38.82 days) and middle-income groups (37.75 days). The number of home-based medical care days was highest in the high-income group (69.66 days), followed by middle-income group (62.24 days), and lowest in the low-income group (59.45 days).
The Marginal Means of Medical and Long-Term Care Utilization Estimated from Generalized Linear Models
Care costs were converted from Japanese yen to US dollars using the 2017 purchasing power parity rate (US$1 = 105.40). The table shows the results (marginal means) of GLMs assuming a negative binomial distribution for care utilization and a gamma distribution for care costs. Analyzed, dependent variables include inpatient care days, outpatient care days, home-based medical care days, counts of home-based LTC services, inpatient care costs, outpatient care costs, home-based medical care costs, prescription costs, home-based LTC costs, and other LTC costs. The exposure of interest was the income level. The models adjusted for the following covariates: gender, age, CNL, death, and the number of years the subjects lived during the study period. The marginal means of the dependent variables were calculated by substituting the means of the estimates into the generalized linear regression models.
Similarly, the usage number of home-based LTC services was most frequent in the high-income group (833.14 times), followed by middle-income group (709.59 times), and lowest in the low-income group (668.84 times). In terms of expenses, the high-income group had the highest, and the low-income group had the lowest in all categories except for other LTC services. Inpatient care cost was highest in the high-income group (USD 28677.48), followed by middle-income (USD 28070.04) and low-income groups (USD 26470.49). Outpatient care cost was highest in the high-income group (USD 3921.75), followed by middle-income (USD 3019.31) and low-income groups (USD 2791.72).
Home-based medical care cost was highest in the high-income group (USD 10971.16), followed by middle-income (USD 9979.69) and low-income groups (USD 9357.09). Prescription cost was highest in the high-income group (USD 7337.23), followed by middle-income (USD 6379.65) and low-income groups (USD 6020.82). The cost of LTC home services was also highest in the high-income group (USD 35215.53), followed by middle-income (USD 29311.41) and low-income groups (USD 28168.24). On the contrary, the cost of other LTC services was highest in low-income group (USD 40165.52), followed by middle-income group (USD 37828.03), and lowest in the high-income group (USD 33774.55).
The research team constructed time-series panel data for the survivor-only subgroup over the 4-year study period, as approximately 47% of the subjects died during the study period. And the team analyzed using random effect models to estimate the influence of income disparity on home care utilization. Table 4 gives the descriptive statistics of survivors.
Characteristics of Surviving Subjects by Income Level
“Surviving Subjects” refer to subjects who did not die during the study period.
The results of covariates and coefficients of each model are presented in Table 5. According to the results of random effect models shown in Table 5, the number of inpatient care days tended to be longer as the income increased, shorter with older age, and longer with higher CNL. The number of outpatient care days tended to be longer as the income increased, and shorter with older age and higher CNL. The number of home-based medical care days tended to be longer as the income increased, longer for women than for men, longer when the age was higher, and gradually increased when the CNL was higher.
Comparison of Surviving Subjects' Medical and Long-Term Care Utilization by Random Effect Model
“Surviving Subjects” refer to subjects who did not die during the study period. Care costs were converted from Japanese yen to US dollars using the 2017 purchasing power parity rate (US$1 = 105.40). The table shows the results of random effects generalized least square regression. Four-year panel data were constructed for 14,795 subjects and the total number of observations was 59,180. Analyzed dependent variables include inpatient care days, outpatient care days, home-based medical care days, counts of home-based LTC services, inpatient care costs, outpatient care costs, home-based medical care costs, prescription costs, home-based LTC costs, and other LTC costs. The models adjusted for the following covariates: income level, gender, age, and CNL.
SE, standard error.
The usage number of home-based LTC services tended to increase as the income level was higher, decrease for women compared with men, decrease with aging, and increase with higher CNL. The costs of inpatient care tended to be similar to the number of days, but significant difference between covariates could not be confirmed. Outpatient costs also tended to be the same as the number of utilization days, increased with the income level, but no statistically significant difference was found. In contrast, the results showed that home-based medical care costs were significantly increased as the income level was higher.
Prescription costs tended to be higher as the income level was higher, lower with older age, and lower as the CNL was higher. In terms of LTC costs, the cost of home-based services increased as the income level was higher, while the other LTC services tended to be significantly decreased. And home-based LTC service costs were lower for women than for men, but other LTC service costs were higher. Furthermore, the home-based service costs decreased with older age, and the other services tended to be increased. The CNL showed that the higher the level, the higher the cost of both. The results of the marginal means of Table 5 are also presented visually in Figure 1.
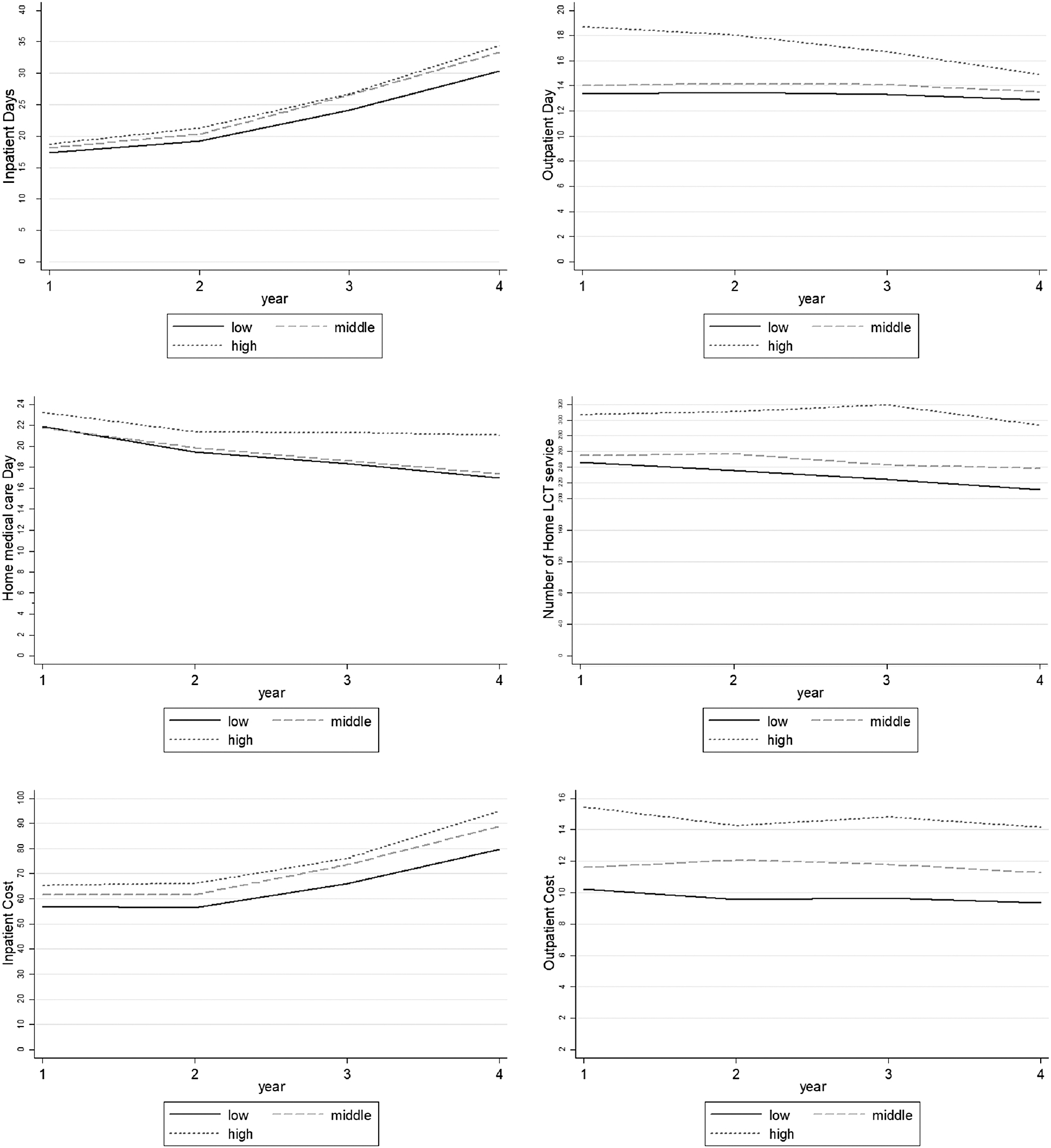
Comparison of medical and long-term care utilization using marginal means by income disparity. This shows the 4-year follow-up of care utilization by income level, which is the result of Table 5. Care costs were converted from Japanese yen to US dollars using the 2017 purchasing power parity rate (US$1 = 105.40) and is in units of US$100.

Discussion
In this retrospective study of older adults with CNL residing in Fukuoka Prefecture in Japan, the team compared the difference in the rates of utilization of medical care and LTC services according to the individual's income level. The team found that subjects in the high-income group had the highest utilization of home-based medical care and home-based LTC services. In contrast, the low-income group had the lowest number of days of home-based medical care and usage number of home-based LTC services, but the highest in terms of utilization of nonhome-based LTC services. This result confirms that the income level, which is considered a socioeconomic factor, had a significant effect, not only on the utilization (amount) of home-based services, but also on the possibility of choosing home-based services.
Japan's statutory health insurance system covers 98.3% of the population, whereas the separate Public Social Assistance Program, for impoverished people, covers the remaining 1.70%. 30 As for premiums, people pay 30% coinsurance for most services, and some copayment. Young children and low-income older adults have lower coinsurance rates, and as described earlier, there is an annual household out-of-pocket maximum for medical care and LTC services based on age and income. There are also monthly out-of-pocket maximums, which vary according to enrollee age and income. 20 For example, the monthly maximum for people aged 75 years and over with modest incomes is JPY 57,600 (USD 546.49); above this threshold, a 1% coinsurance rate applies.
Low-income older adults do not pay more than JPY 24,600 (USD 233.40) a month. In addition, there is an annual household health and LTC out-of-pocket ceiling, which varies between JPY 340,000 and 2.12 million (USD 3225.81–20113.85) per enrollee. For people aged 75 years and over, it varies between JPY 190,000 and 670,000 (USD 1802.66–6356.74) per enrollee, according to income. 31 Above this ceiling, all payments can be fully reimbursed.
So, despite the generally high copayment rate, the proportion paid by patients is only 14% of national medical expenses, because of the reduced rate for elderly people and the provision of catastrophic coverage. 32 This means that in terms of Japan's insurance system, it is unlikely that there will be restrictions on the use of health and LTC services due to economic reasons.
Despite the background of this insurance system, the research team confirmed that there is a significant difference in care utilizations, especially home-based services, according to income levels. This study showed that the utilizations of home-based medical and LTC services significantly increased with higher incomes, and these results suggested that socioeconomic factors clearly influence the utilization of home-based care services, not only medical care but also LTC services, among older adults.
Moreover, subjects of this study were adults aged 75 years or older who have a CNL on LTC insurance, and approximately 50% of them died during the observed period of 4 years. In the analysis using the person-year methods considering the individual's survival period, the team also found that the use of home-based medical and LTC services significantly increased with higher income. This suggests that economic factors are highly likely to influence the choice of home-based end-of-life care.
According to studies mentioned earlier, those who use home-based services are less likely to be hospitalized or institutionalized than nonusers. 10,11 In particular, the results showed that the enhanced home service provision system reduces the utilization of hospitalization and medical institutional deaths and, moreover, increases the utilization of home-based end-of-life care.
As such, the improvement of home-based services is an obvious factor that can reduce the use of care that takes place outside of home, such as inpatient care for older adults. Through this study, the team confirmed that economic factors have a significant effect on the older adult's utilizations of home-based services. This suggests that low-income older adults have relatively limited (unable to) access to home-based services, which indicates that low-income older adults are more likely to stay in hospitals or facilities rather than at home for the long term. As is the goal of Japanese CICS, to support older adults especially those aged 75 and over, who will increase rapidly in the future, home-based medical and LTC services should play a very important role.
Therefore, it is a very important task to identify the factors that influence the use of home-based services in terms of CICS policy, and through this study, it was confirmed that one of the factors is the economic circumstances of older adults. As mentioned earlier, however, under Japan's insurance system, it is unlikely that the low-income population will be able to use the services they want on their own due to the burden of copayments. The results of this study show that economic factors had an effect on the utilization of home-based services, but it is necessary to take into account other factors that indirectly affect income disparity, such as the presence or absence of family members living together or the level of education, and other living environments.
Therefore, authors suggest that policymakers should increase the availability of home-based services by considering the possible derivative factors included in economic resources, such as the presence or absence of family members and the structural situation of the living arrangement. Authors also propose a large-scale health literacy campaign to increase understanding of home care services for low-income people with relatively low health literacy.
This study has several limitations. First, the study was conducted using data only on Fukuoka Prefecture residents, which limits the generalizability of the findings of this study. 33 This prefecture has a relatively high number of hospital beds and relatively high medical expenses per person, and this study's results, therefore, may be overestimated. Second, the claims data did not include detailed information about living conditions, reflecting the subjects' family structure or characteristics of living, which may influence the individual's income level.
Third, although the statistical analysis incorporated characteristics such as gender, age, and care needs level, the specific diseases of each subject were not taken into consideration. Fourth, no clinical data (eg, disease progression or laboratory test results) for individual subjects were included because this study focused on the subject's income level. Finally, care needs level was used as a covariate, but unable to account for any changes in this level over the study period.
Conclusions
In this study, the research team showed the difference of household income level in Japan's CICS on the use of medical and LTC services among older community-dwelling adults. A key policy objective of the Organization for Economic Cooperation and Development (OECD) member states is to ensure that all people have access to adequate health care according to their basic needs. 12 In most countries, with the same health care needs, people with higher incomes are more likely to consult a doctor than those with lower incomes. Most OECD countries have endorsed as major policy objectives the reduction of inequalities in health status and the principle of adequate or equal access to health care based on need.
Equity of access is a key element of health system performance in OECD countries. Given the current trend of an aging global population, it will be necessary to increase the accessibility of all elderly people to the use of home services, which is the basis of “aging in place.” Based on this study, additional research is needed to scrutinize factors that influence the older adult's decision to use home-based care services.
Footnotes
Acknowledgments
We thank the Fukuoka Prefecture Association of Latter-Stage Elderly Healthcare for the provision of health care claims data and LTC insurance claims data.
Authors' Contributions
Dr. Kim led the study design; conducted the literature search; acquisition of data, analysis, and interpretation of data; and wrote the article. Dr. Babazono helped with conception and study design, critical revision of the article, and administrative and material support. Dr. Fujita and Dr. Aziz helped with revision of the article.
Ethics Approval
This study was approved by the institutional review board of St.Mary's hospital and Kyushu University (Research Ethics Review Board of St.Mary's hospital, Approval No. 22-0701), (Clinical Bioethics Committee of the Graduate School of Healthcare Sciences, Kyushu University, Approval No. 20209).
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.