
Abstract
As health systems attempt to contain utilization and costs, care management programs are proliferating. However, there are mixed findings on their impact. In 2018, Rhode Island initiated a care management program for dually eligible Medicare and Medicaid beneficiaries at high risk of hospitalization or institutionalization. The objective of this study is to evaluate the association between health care utilization and costs and care management for dual-eligible participants (n = 169). The authors employed an interrupted time series analysis of administrative claims data using the Rhode Island All Payer Claims Database, which includes data from all major payers in the state, for 11 quarters (January 1, 2017 until September 1, 2019). On average, participants were younger (46.2% were 19–64 years of age vs. 41.9% of non-participants), female (71% vs. 62.6% of non-participants), and had a higher comorbidity burden (more commonly had anemia, atrial fibrillation, chronic kidney disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hyperlipidemia, hypertension, ischemic heart disease, and stroke). Participation was associated with significantly fewer hospital admissions (118 fewer admissions per 1000 admissions per quarter; 95% confidence interval [CI] −11 to −22), and a reduction in Medicaid ($1841 less spent per quarter, 95% CI −2407 to −1275) and total ($2570 less spent per quarter; 95% CI −$4645 to −$495) costs. Participation was not significantly associated with a change in Emergency Department (ED) visits, preventable ED visits, Skilled Nursing Facility stays, or Medicare costs. These results suggest that targeted care management programs may provide dual-eligible beneficiaries with needed services while diverting inefficient health care utilization.
Introduction
Nationally, there are 12.3 million dual-eligible beneficiaries for Medicare and Medicaid on the basis of age and/or disability status and lower income. 1 Dual-eligible beneficiaries are more likely to be medically high-need and high-cost and account for a disproportionate share of both programs' spending. 2 –4 In 2019, dual-eligible beneficiaries accounted for 19% of Medicare beneficiaries and 14% of Medicaid beneficiaries, but 34% and 30% of spending, respectively. 1
Dual-eligible beneficiaries are often more medically complex: They are more than 3.5 times more likely to have 3 to 6 limitations in their activities of daily living versus non-dual fee-for-service (FFS) Medicare beneficiaries (25% vs. 7%), 3.2 times more likely to rate their health as poor (13% vs. 4%), and 4.3 times more likely to be institutionalized (13% vs. 4%). 1 They also manage a higher burden of chronic disease: among FFS dual-eligible beneficiaries, 14% have Alzheimer's disease or related dementia, 29.2% have diabetes, and 19% have more than six chronic conditions. 1,5 While researchers have observed low persistence of high-cost status among non-dual FFS Medicare beneficiaries, the majority of high-cost, dual-eligible beneficiaries are persistently high-cost over three years, driven mostly by long-term care costs. 6,7
While Medicare and Medicaid cover unique services for dual-eligible beneficiaries (eg, Medicare covers hospitalization and post-acute care while Medicaid covers out-of-pocket costs and long-term care), there is overlap between covered services (eg, both programs cover acute and ambulatory care services). 8 In some states, Medicaid also covers long-term home and community-based services for dual-eligible beneficiaries. Care management for patients with complex care needs is a valuable tool for government agencies, health systems, provider groups, and payers to improve outcomes while controlling costs. Broadly, care management is defined as a team-based, patient-centered approach to aid patients and their families or care teams in managing their medical conditions more effectively. 9 Care management programs may be particularly valuable for dual-eligible beneficiaries to navigate the breadth of social supports and medical benefits they receive, as well as the dual administration of their coverage.
Research shows mixed results on the efficacy of care management interventions. 10 –20 Recently, a high-profile randomized-control trial of the Camden Coalition of Healthcare Providers found no association between care management assignment and a change in readmission rates among health care “super-utilizers” versus individuals who received their usual care. 12 However, while there are mixed results, care management interventions in specific populations have been associated with improving disease management and outcomes, including reductions in all-cause mortality, inpatient admissions, and overall health care costs. 11,14,15 Further, qualitative findings suggest that care management programs tend to be rated favorably among high-risk patient populations. 21 Currently, the research and policy community lacks sufficient information on effective efforts to manage the care of dual-eligible beneficiaries.
In 2018, the state of Rhode Island contracted with a community-based care management program to coordinate the social, environmental, and health needs of high utilizing dual-eligible beneficiaries. Individuals were assigned to the program if they were categorized as high-risk for hospitalization or nursing home admission by the state of Rhode Island's Executive Office of Health and Human Services (EOHHS) based on a prior inpatient emergency department (ED) or hospitalization stay or high-risk of nursing home admission. Study authors did not participate in defining program participation criteria. Community health workers employed by the community-based care management program assessed dual-eligible clients' care goals and connected them to resources, provided health education, and supported their physical and behavioral health needs. The objective of this study is to evaluate the impact of the community-based care management program on the participant's health utilization and costs.
Material and Methods
The community-based care management program
In 2018, the Rhode Island EOHHS contracted with a community-based care management program to coordinate the social, environmental, and health needs of high utilizing dual-eligible beneficiaries. The care management team included community health workers, nurse case managers, clinical care managers, program managers, and a program director (Fig. 1). The program employed a peer-to-peer model, which allowed community health workers with experience navigating the health care system to serve as mentors and patient advocates to help dual-eligible clients. The community health workers' role included addressing medical, educational, and socio-economic needs, providing education on the proper use of medical resources, removing barriers to care, assisting in care coordination, providing access to community-based support services, and linking individuals to a broader suite of services to support clients' health, social, and personal needs. The nurse case managers and clinical care manager sign off on care plans, support the community health workers, provide case reviews, and work directly with EOHHS to access services for clients. The program manager runs program staffing, facilitates regular communication across program staff, and structures staff development. The program director sought program support and funding and provided strategic guidance and oversight for all clinical and program staff members. The program's objective was to support clients in their efforts to continue to live at home while avoiding the need for unnecessary hospital and nursing home care.

Care management program workflow. All interactions detailed in CMP's secure database.
The initial cohort of dual-eligible beneficiaries were flagged for program assessment and enrolled in the program in the third quarter of 2018 (July–September). Eligibility for the community-based care management program was assessed by Rhode Island's EOHHS; dual-eligible beneficiaries were flagged for program referral based on a retrospective claims analysis, social risk factors (eg, homelessness), or other factors, indicating a high risk of hospitalization or nursing home admission. Clients were deemed eligible based on prior participation in a care management program run by a managed care organization that enrolled dual-eligible beneficiaries. Finally, other health or social service agencies could flag dual-eligible beneficiaries for assessment.
As shown in Figure 1, once a dual-eligible beneficiary was flagged as high-need, a community health worker was tasked with 3 rounds of phone or text outreach to assess program eligibility. If an individual was ineligible, they were connected to other community resources. If an individual was determined eligible, the community health workers conducted a home visit where they performed a health risk assessment. If the community health worker flagged that a dual-eligible beneficiary's care plan would require additional medical expertise, a nurse case manager would schedule an additional home visit to conduct a comprehensive functional needs assessment. If the community health worker noted that the dual-eligible beneficiary was managing behavioral health needs or intensive social needs, then a social worker was assigned to the case for consultation and direct client contact. After the assessment, the community health worker would create a care plan and document the participant's care goals. Goals included support with understanding how to utilize a primary care provider and accessing durable medical equipment, home care, transportation, food, clothing, housing, long-term services, etc. (Table 1). The care plan was reviewed and approved by the team's clinical care manager. Then, the community health workers, assisted by the nurse case managers and social workers, connected clients with resources based on their care plan (eg, home care services, durable medical equipment, housing, home visits, transportation) (Table 1). The team would assist a dual-eligible beneficiary until there are no other immediate needs identified in their care plan.
Community-Based Care Management Participants' Care Goals and Program Activities
Care management goals and activity arranged from most frequent to least frequent; participants can have >1 care management goal and activity.
Once no immediate needs remained, a client would transition from active management to maintenance status. In maintenance, clients would receive monthly contact from the community health workers. If on these monthly calls, a client or the community health worker identified a new need, the client would re-initiate into active care management status. Throughout each step in the client engagement process, all steps were documented by the community-based care management team's staff in their secure database.
Data
This analysis was conducted using the administrative claims files from the Rhode Island All Payer Claims Database (APCD), which includes data from all major payers in the state, including commercial plans, Medicare Advantage plans, Medicaid FFS, and Medicare FFS. The authors analyzed utilization and cost data available from January 2017 through September 2019. These data were reported at the individual-level and analyzed at the person-quarter level. The final sample size includes 1183 patient-quarters representing 169 unique dual-eligible beneficiaries (Table 2).
Sample Characteristics
Community-based care management participants defined as individuals assessed and receiving active treatment (n = 102), received treatment, but had case closed (n = 17), receiving stable treatment (n = 108) as of October 2018 (n = 169; n = 58 removed from the sample given later treatment initiation).
Other dual-eligible beneficiaries were unassessed by the care management program (n = 40,920); the authors removed enrollees who were institutionalized during the pre-period (n = 2952), had incomplete Medicaid eligibility (n = 709), lacked data on their original eligibility for Medicare (n = 718), had incomplete demographic data (n = 108), had unavailable ZIP code data (n = 21), were younger than 18 years of age (n = 599), and were enrolled in a Medicaid managed care organization during the study period (n = 23,043).
Indicates statistically significant difference from comparison beneficiaries; P-value <0.05 P-value <0.01 P-value <0.001.
DIB, disability insurance benefits; ESRD, end-stage renal disease.
Participants
The authors defined dual eligibility as 9 or more months of Medicaid and Medicare enrollment during the intervention period (October 1, 2018–September 30, 2019). Community-based care management participants were assigned to the treatment group if they were dual-eligible beneficiaries referred to the program who were deemed eligible for the program by the program's staff. Participants were excluded if they were not dual-eligible at the time of assessment or were referred to the community-based care management program but deemed ineligible because they were enrolled in a different care management program or unable to be contacted. Of the n = 686 dual-eligible beneficiaries referred to the program by the Rhode Island EOHHS, the authors included n = 169 in their sample analysis.
The authors excluded dual-eligible beneficiaries who refused assessment or treatment (n = 2), were referred, but could not be contacted (n = 155), were found ineligible due to participation in a different community-based program or moving out of state (n = 247), or were assessed, but then found ineligible (n = 35). The authors utilized the referral date to indicate treatment initiation and matched it to the study quarter.
The study population included dual-eligible beneficiaries who initiated the program between July 1, 2018 and September 30, 2018. The authors excluded dual-eligible beneficiaries who were referred to community-based care management program after this period (n = 58) given the use of an interrupted time series design. The authors defined the pre-intervention period as January 1, 2017, until July 1, 2018. The authors defined the post-intervention period as October 1, 2018, until September 1, 2019. Dual-eligible beneficiaries were included in the treatment group if they had a completed care plan and a record of 1 or more clinical or social care coordination activities in the care management group's database (n = 169). Participants were either receiving active treatment (n = 74), received treatment but had their case closed (n = 14), or receiving stable treatment (n = 81). Active treatment is defined as an open case where a participant continues to receive active assistance from the care coordination team, a closed case means an individual either died (n = 9), moved out of state (n = 2), or entered a skilled nursing facility (SNF) (n = 3), and stable treatment means that the client has completed the goals of their care plan. The length of program participation varied, and approximately half of the sample remained in active management by the end of the study period. For the purposes of the evaluation, the authors considered an individual as within the treatment group throughout the entire study period if they met the inclusion criteria.
Main measures
The outcomes of interest were person-quarter level utilization rates and costs. For utilization outcomes, the authors calculated quarterly inpatient utilization, which included all-cause inpatient hospital admissions, all-cause ED visits, and preventable ED visits. The authors characterized preventable ED visits by applying the New York University algorithm. 22 Preventable ED visits are of particular interest, because these visits may be most sensitive to care coordination aimed at educating dual-eligible beneficiaries on primary providers' services and better coordinating patient care. For SNF utilization, the authors evaluated the quarter-level number of SNF stays. The authors also analyzed the number of SNF stays that were 20 days or greater, as a key objective of the community-based care management program was to reduce longer-term nursing home admissions and the associated costs to the Medicaid program.
For cost outcomes, the authors calculated the total costs of care for each patient, quarterly, excluding drug costs. Drug costs were excluded, as pharmacy benefit managers are not required to report data to the APCD. Therefore, the authors calculated all other medical costs as the total allowed amounts, which includes patient copayment or coinsurance amounts in addition to the health plan paid amount. The authors summarized costs for a patient's medical services within a quarter. The authors ran separate models for Medicaid costs, Medicare costs, and total costs.
The authors included a set of control variables including sex; age group (19–64, 65–84, 85 and older); years of Medicaid enrollment; original reason for Medicare entitlement (old age and survivor's insurance, disability insurance benefit, end-stage renal disease, or disability insurance benefits and end-stage renal disease); chronic condition diagnoses (anemia, atrial fibrillation, cancer, chronic kidney disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hyperlipidemia, hypertension, ischemic heart disease, stroke, and Alzheimer's disease and related dementia); and ZIP code. The authors assigned a person's ZIP code based on where they lived during the seventh quarter of the study (July 2018 through September 2018), which was the timing of the community-based care management program initiation per the study definition.
Design
The study period spanned 11 quarters beginning on January 1, 2017, until September 1, 2019. Pre- and post-period characteristics were compared between dual-eligible beneficiaries who participated in the community-based care management program versus those who did not participate using t-tests. For each dual-eligible beneficiary in the study population, the authors calculated quarter-level outcome measures.
The authors employed an interrupted time series design to evaluate whether participation would reduce utilization and costs. The identifying assumption of this analysis is that the outcomes of interest (all-cause inpatient hospital admissions, ED visits, preventable ED visits, SNF stays, longer-term SNF stays, and Medicaid, Medicare, and total costs) would have remained unchanged without the intervention. Using the pre-intervention period as the control, in this analysis the authors assessed whether the community-based care management program intervention had an effect significantly greater than the underlying trends in utilization and costs.
Employing an interrupted time series analysis allowed the authors to compare an individual's health utilization and spending trajectories after the intervention to the individual's expected utilization and spending based on their prior history. 23 –27 Given the baseline differences between community-based care management program participants and non-care management participants that are dual-eligible, the past utilization and spending of care management participants may serve as a more valid comparator (Table 2).
The authors ran unadjusted and adjusted models that accounted for the earlier cited control variables and used general estimating equations for all analyses. For utilization measures, the authors modeled quarter-level utilization counts, including all-cause inpatient hospital admissions, ED visits, and preventable ED visits, SNF stays, and longer-term SNF stays (20 days or greater) using interrupted time series models assuming a Gaussian distribution with an identity link. For cost measures, the authors modeled quarter-level costs using interrupted time series models assuming the Gaussian distribution and identity link. To account for repeated measures, the authors used robust standard errors and individual-level clustering. The analyses were conducted in Stata version 16.1. The Brown University Institutional Review Board approved the study protocol.
Results
The study cohort included a sample of 169 dual-eligible beneficiaries who participated in the community-based care management program. Community health workers conducted an average of 5.3 in-person visits (ranging from 1 to 27) and 35.1 phone calls (ranging from 2 to 187) with program participants while in active management (Supplementary Table S1). At baseline, 63.3% of care management participants rated their physical health as fair or poor and 40.2% of participants rated their mental health as fair or poor (Supplementary Table S1).
On average, participants were more likely to be entitled to Medicare benefits due to disability (61.5% vs. 48.7% of non-participants), female (71% vs. 62.6% of non-participants), and have a higher comorbidity burden (participants were more likely to have atrial fibrillation, chronic kidney disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hyperlipidemia, hypertension, and stroke) (Table 2).
During program initiation, community health workers assessed participants' program goals. Of the 931 documented goals across all community-based care management participants, participants most frequently sought support with accessing primary care provider education and support (21.2%), durable medical equipment (14.6%), home care (11.3%), transportation (8.1%), food and clothing security (6.0%) (Table 1). Of all activities performed, and there were 14,797 separate logged activities performed during the initial 4 quarters of the program, community health workers most frequently provided participants with support with home care services (12.5%), durable medical equipment (11.3%), housing (10.2%), and administrative challenges (10.0%, and assistance with the Medicaid Management Information System (6.0%) (Table 1). If included in the care plan, community health workers provide primary care provider education programs to ensure participants have a primary care provider, access their primary care provider appropriately, and accurately represent their medical and social needs during routine appointments. In addition, community health workers assisted program participants with completing forms necessary to access additional services (eg, food, housing, transportation benefits) and obtain medical equipment or home improvement supplies. Further, the community health workers partner with program staff to communicate with EOHHS about specific client needs and escalate requests for additional services or medical or home supplies. Additional data about the community-based care management program participants are available in Supplementary Tables S1 and S2.
This interrupted time series analysis showed that community-based care management participation was significantly associated with lower inpatient hospital admissions (an average of 118 fewer per 1000 visits per quarter; 95% confidence interval [CI] −226 to −11; P = 0.03), and a reduction in Medicaid costs (an average of $1841 per quarter, 95% CI −2407 to −1275; P ≤ 0.001) and total costs (an average of $2570 less spent per quarter; 95% CI −$4645 to −$495; P = 0.02) (Table 3 and Fig. 2).
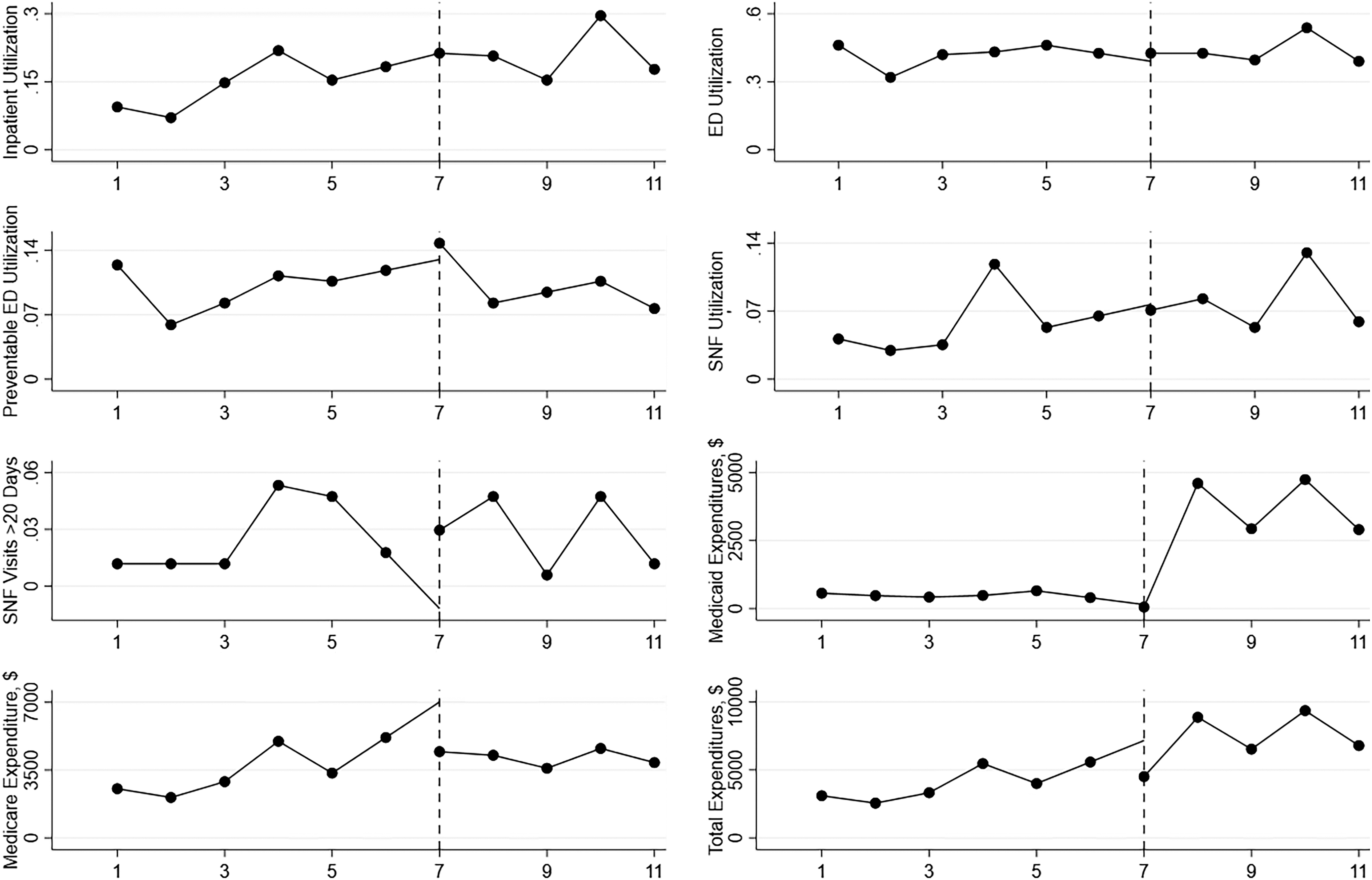
Adjusted interrupted time series analysis. Models adjusted for member age, gender, original reason for Medicare entitlement, years of Medicaid eligibility, Alzheimer's disease and related dementia, anemia, atrial fibrillation, cancer, chronic kidney disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hypertension, ischemic heart disease, stroke status, ZIP code, and a quarter-level time fixed effect. Time period 7 reflects Quarter 7 of the study (June 2018–September 2018), where the program began for the n = 169 participants.
Interrupted Time Series Analysis (Quarter-Level Outcomes), January 1, 2017–September 1, 2019
The coefficient for utilization indicates the change in the average number of visits per 1000 visits per quarter; the coefficient for costs indicates the change in average spending per quarter.
Indicates statistically significant difference from comparison beneficiaries; P-value <0.05 P-value <0.01 P-value <0.001.
Models adjusted for member age, gender, original reason for Medicare entitlement, years of Medicaid eligibility, Alzheimer's Disease and related dementias, anemia, atrial fibrillation, cancer, chronic kidney disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hypertension, ischemic heart disease, stroke status, ZIP code, and a quarter-level time fixed effect. ED, emergency department.
Participation was not significantly associated with a change in ED utilization (an average of 148 fewer per 1000 visits per quarter; 95% CI −335 to 39; P = 0.12), preventable ED utilization (an average of 30 fewer per 1000 visits per quarter; 95% CI −106 to 47; P = 0.45), SNF stays (an average of 71 fewer stays per 1000 visits per quarter; 95% CI, −149 to 7; P = 0.08), long-term SNF stays (an average of 36 fewer stays per 1000 admissions per quarter; 95% CI, −72 to 0; P = 0.06), and Medicare costs (an average of $729 less spent per quarter; 95% CI, −$2741 to $1283; P = 0.48) (Table 3 and Fig. 2). Additional data on the unadjusted results is available in Supplementary Figure S1.
Discussion
In this study, the authors evaluated the impact of a community-based care management program on the utilization and costs of dual-eligible beneficiaries. Utilizing the comprehensive Rhode Island APCD, the authors observed that dual-eligible beneficiaries enrolled in the community-based care management program were more medically complex. In the adjusted interrupted time series analysis, participation was associated with a statistically significant reduction in inpatient hospital admissions, Medicaid costs, and total costs. In addition, participation was associated with a reduction in SNF visits, including SNF visits that exceeded 20 days; however, these findings did not reach statistical significance at the P < 0.05 level.
The association between care management participation and reductions in inpatient hospital admissions and Medicaid and total costs aligns with prior work that has documented cost reductions among high-need, Medicaid participants. 15,28 These findings align with prior studies that show that care management programs can reduce health utilization and costs when targeted to specific patient populations. 29 –32 The authors observed that participation was not significantly associated with reductions in ED visits, preventable ED visits, Medicare costs, and SNF stays. These findings align with prior studies that document the lack of association between care management participation and a reduction in ED visits among medically complex patients. 12,16,17,33
Research links care management programs to improved outpatient follow-up, participant quality of life, access to medical equipment, and linkages to long-term services and supports, depressive symptoms, self-rated health, and disease control. 18 –20,33,34 Given these findings, future research should investigate the impact of the community-based care management intervention on these additional outcomes accounting for patient care experience, disease management, and quality of life. Future research could include an analysis of the cost-effectiveness of these interventions evaluating the potential savings versus program costs. Finally, future research could be designed to include a randomization component that would allow for a comparison between dual-eligible beneficiaries who did and did not participate in the care management program.
This research faces several limitations. First, dual-eligible beneficiaries in the community-based care management program were not randomly selected, but instead included in the program by the State of Rhode Island's EOHHS based on an individual's high risk of hospitalization, ED admission, or nursing home admission. While the authors tested the use of comparative interrupted time series based on a control group created using inverse probability of treatment weighting, the authors could not achieve adequate balance on the covariates given baseline differences between program enrollees and other dual-eligible beneficiaries. As such, the authors' results using interrupted time series compare the trajectories of program participants before and after program initiation, which is a valid research design for measuring the effects of interventions. 23 –27 Second, the lack of random selection may induce a regression to the mean bias in the author's findings. Prior evaluations of utilization patterns among individuals with high health care use and costs document a reduction in utilization over time regardless of intervention, as persistent high utilization is uncommon. 35 However, this is less true for groups with more persistent health care utilization such as high-need dual-eligible individuals. 7,35 Third, the state of Rhode Island does not report race or ethnicity data in the APCD, and therefore the authors cannot account for potential racial and/or ethnic disparities in care management participation and outcomes. Fourth, the study focuses on a program that took place in a single state for a select group of enrollees, which may limit generalizability to other settings. Despite these limitations, the authors find significant reductions in utilization associated with the community-based care management program.
Conclusion
This study is the first to evaluate the impact of a new community-based care management program for Rhode Island's high utilizing dual-eligible beneficiaries. The authors find that participation was associated with a reduction in inpatient hospital admissions, Medicaid costs, and total costs. As state officials, clinicians, and health insurers attempt to contain growing health care costs, particularly among dual-eligible beneficiaries, these results suggest that community-based care management programs may offer a viable mechanism to provide participants with needed services while diverting inefficient and expensive health care utilization.
Footnotes
Authors' Contributions
Ms. Tucher: Conceptualization, methodology, software, validation, formal analysis, investigation, writing—original draft, writing—review and editing, visualization, and project administration; Dr. McHugh: Conceptualization, writing—review and editing, and supervision; Dr. Thomas: Conceptualization, writing—review and editing, and supervision; Dr. Wallack: Conceptualization, methodology, investigation, writing—review and editing, supervision, project administration, and funding acquisition; Mr. Meyers: Conceptualization, methodology, validation, investigation, writing—review and editing, supervision, project administration, and funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to disclose. Dr. Wallack and Dr. Meyers were under contract by Rhode Island Parent Information Network to conduct the analysis, but this research reflects the research team's analytic plan and interpretations.
Funding Information
This study was funded by the Rhode Island Parent Information Network (RIPIN) under a contract from the Rhode Island Executive Office. The funders had no role in the design, analysis, or interpretation of the results.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.