
Abstract
Individuals with prediabetes living in hard-to-reach and underserved areas experience barriers to accessing traditional in-person preventive health services. The National Diabetes Prevention Program (DPP) is a preventive health care program designed to reduce the risk of developing type 2 diabetes. Although there have been increasing numbers of remote DPPs accessible, there are little data on the clinical outcomes of digital DPPs for members living in hard-to-reach and underserved areas. This study assessed whether living in a designated Health Professional Shortage Area (HPSA) and a rural versus urban area impacted the weight loss of N = 7266 members of a fully digital program called Lark DPP. Secondary analyses included between-group comparisons of program retention and member characteristics, demographics, and socioeconomics. Percent weight loss did not differ by HPSA (P = 0.16) or rural/urban status (P = 0.15), despite greater potential barriers for members residing in HPSAs (eg, highest starting body mass index, lowest income, lowest education). Mean percent weight loss for members residing in an HPSA and rural area was mean (M) = 4.75%, standard error (SE) = 0.09; for members in a non-HPSA, rural area M = 4.96%, SE = 0.16; for members in an HPSA, urban area M = 4.55%, SE = 0.13; and for members in a non-HPSA, urban area M = 4.77%, SE = 0.13. Members of a fully digital DPP achieved weight loss that did not differ by HPSA or urban/rural designation. Fully digital programs offer a solution to reduce the risk of type 2 diabetes in areas where residents may not otherwise have access to diabetes prevention services.
Introduction
Since the inception of the National Diabetes Prevention Program (NDPP) in 2010, 1 the Centers for Disease Control and Prevention (CDC) has worked to scale this program for increased reach and accessibility to curb the epidemic of prediabetes in the United States. The NDPP has expanded its offerings, but as of 2018, only 27.9% of counties had an in-person NDPP partnership site. 2 In-person NDPP sites were more likely to be in an urban versus rural county and were starkly underrepresented in the areas of highest diabetes incidence and area deprivation. 3 Alternative modalities of delivery, such as digital programs, are critical to helping the NDPP offer accessible preventive services to all those in need, especially those in hard-to-reach and/or underserved areas. 4
Individuals living in rural areas and/or areas designated as having a shortage of health care providers experience barriers to health care access that negatively impact their health. 5,6 Basu et al 7 observed a 51.5-day increase in life expectancy and reduced mortality by 30.4 deaths per million from cardiovascular disease for every additional 10 primary care physicians per 100,000 people. However, from 2005 to 2015 the density of primary care physicians in the United States decreased from 46.6 to 41.4 per 100,000 people. This trend is expected to continue, with physician workforce shortages projected throughout the United States in 2030. 8
Digital Diabetes Prevention Programs (DPPs) have the potential to reach millions of people regardless of geographic location or proximity to preventive health services and help those with prediabetes to reduce their risk of developing type 2 diabetes. Enrollment in the NDPP is greatly needed, as there are currently 96 million individuals living with prediabetes in the United States. 9 Given the potential for increased reach, the Diabetes Prevention Recognition Program recognized online modes of delivery in 2015. 10 The NDPP recently reported enrollment statistics categorized by mode of delivery. Since the recognition of online programs, cumulative enrollment in the NDPP has increased most steeply due to online offerings. 11
The ability of online programs to reach and scale has led to more participants enrolling through online organizations compared with in-person organizations. Consistent with these findings, recent research on a fully digital DPP called Lark showed that 30.8% of its enrolled members resided in areas designated as whole-county Health Professional Shortage Areas (HPSAs) and 24.4% lived in designated rural areas. 12 Only 7.6% of enrolled members had access to an in-person DPP within their zip code. Despite the encouraging enrollment, little is known about the primary DPP outcome, weight loss, for members of digital DPPs who reside in HPSAs and/or rural areas in the United States.
The primary aims of this study were to compare weight loss in a fully digital program called Lark DPP between members living in HPSAs versus areas with sufficient care providers and members living in urban versus rural areas because although many HPSAs are in rural communities, there are also HPSAs in urban locales. In addition to the negative associations between HPSAs and health, previous research has shown that individuals living in HPSAs had a lower likelihood of successfully completing a chronic disease self-management program. 13
Based on the findings of Towne et al, 13 and the negative associations between HPSAs and health, the primary hypotheses were that members living in HPSAs would have a lower percent weight loss than those living in non-HPSAs due to assumed barriers to program engagement, and members living in rural areas would have a lower percent weight loss than those living in urban areas due to barriers to quality health care in rural areas and lower engagement in health-promoting behaviors compared with urban counterparts. 14
Methods
Description of the program
The Lark DPP has full CDC recognition (Organization No. 4358176), which involves an assessment of real-world clinical effectiveness and approval of the curriculum. The program guides members through the 26 PreventT2 curriculum lessons developed by the NDPP. 15 The digital platform is available to members 24 hours a day through Android or iOS smartphones; thus, educational lessons can be completed at a member's convenience. The program reinforces the PreventT2 educational content by encouraging healthy dietary changes, physical activity, good sleep hygiene, and stress management through personalized interactive coaching powered by artificial intelligence (AI).
The digital platform facilitates diet tracking through an intuitive meal-logging system powered by natural language processing. Physical activity may be entered manually by a member and/or tracked passively from the motion sensors in a member's phone (or third-party programs such as Apple Health Kit) and edited as necessary by the member. The conversational AI coach encourages members to engage in these self-tracking behaviors and provides synchronous feedback, tips, and encouragement on progress toward goals. A detailed supplement describing this AI-powered program is published elsewhere. 16
Per the NDPP standards, the primary goal of this AI-powered DPP is weight loss, and members are encouraged to lose 5%–7% of their starting weight. This magnitude of weight loss is clinically meaningful and associated with a 58% reduction in the risk of developing type 2 diabetes. 17 Members receive a cellular-connected digital scale that automatically uploads their weigh-ins to the digital platform and are encouraged to weigh themselves weekly to track their progress.
DPP inclusion criteria
Members enroll in the AI-powered DPP as a covered service under their health insurance plans or employer. Digital advertising (eg, Facebook) and/or outreach from the health plan, employer, or Lark helps facilitate awareness of this covered service. In addition to being a Lark DPP member, inclusion criteria for this study followed CDC requirements 18 : (1) >18 years old; (2) no previous diagnosis of type 1 or 2 diabetes; (3) initial body mass index (BMI) ≥25 kg/m2 (or ≥23 if Asian); and at least 1 of the following: (4) blood test result (within the past year) of either fasting plasma glucose between 100 and 125 mg/dL, 2-hour plasma glucose after 75-g glucose load between 140 and 199 mg/dL, or hemoglobin A1c 5.7%–6.4%; or (5) a risk score indicating high risk for type 2 diabetes as defined by CDC criteria. Most members qualify for the DPP based on criterion 5.
The Lark DPP enrollment process is as follows: Upon viewing digital marketing materials, interested individuals proceed to the CDC risk screener 19 where they respond to risk assessment questions. Individuals who receive high-risk scores for prediabetes (≥5/10) can then input their insurance information. If the Lark DPP is a covered program under their insurance plan, interested individuals can download the application. Once prospective members open the application, an onboarding and consent process occurs introducing the focus and goals of the program, providing the Lark privacy policy along with a preview of what participating members can expect, and enabling members to customize their notification and data-sharing settings. If an individual is still interested in program participation, they proceed to order the Lark cellular scale.
Completion of these steps triggers the Lark AI coach to send a message to the member that their coaching has begun. For this study, the authors excluded members from analyses who had not completed these steps and engaged in at least 1 educational lesson (indicating program initiation) and those who did not provide a starting weight measurement in the first 10 days. Per these criteria, there were 904 individuals who chose not to proceed in the program after onboarding.
From the basic eligibility demographics provided, individuals who chose not to continue were significantly younger, mean (M) = 46.0, standard error (SE) = 0.15 years, than those who continued in the program, M = 49.2, SE = 0.17 years, t(8173) = −14.1, P ≤ 0.0001. There was also a lower percentage of females (72.6%) among those who chose not to continue than those who continued in the program (76.2%), χ 2 (8170) = 13.3, P ≤ 0.001. There were no observed differences in race.
Study design
This study received exemption status from Advarra (Protocol No. Pro00047181) Institutional Review Board for retrospective analyses of previously collected and de-identified data. All members agreed to a privacy policy at registration, which included permission to use their de-identified data for research. The authors analyzed data for 7266 members who met inclusion criteria and initiated the program between January 2020 and April 2021. For the flow of members through the study (Fig. 1).
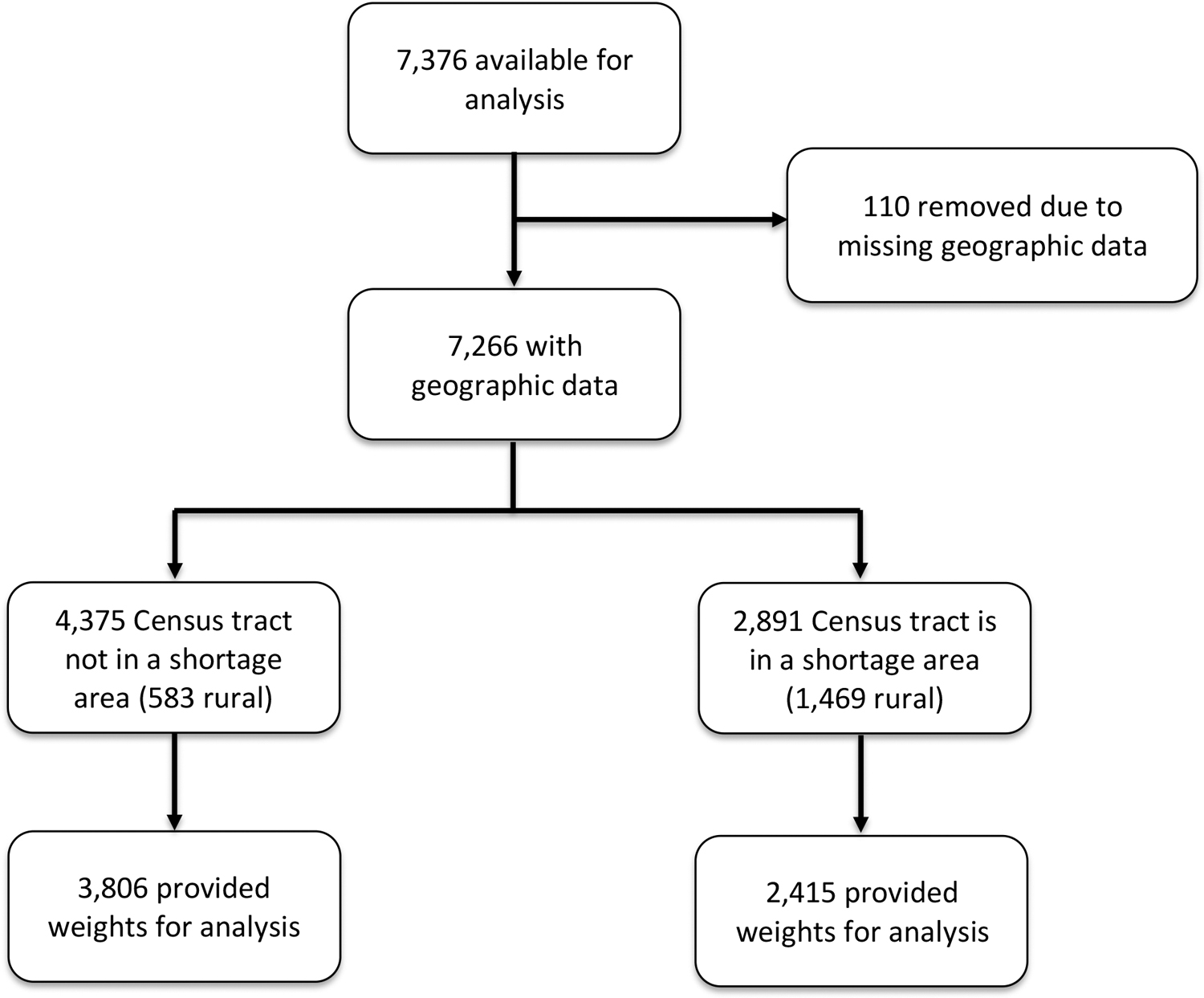
Flow of members through the study.
Comparisons of weight loss by HPSA and rurality status
Starting weight was the first valid weight provided and confirmed to be accurate by a member in the first 10 days of the program. As a quality control, outlier detection algorithms flag abnormal subsequent weigh-ins for review by identifying a weight loss rate of 3.18 kg/week and remove outlier weights unless confirmed by the member to be accurate. The primary outcome of this study was the peak percent weight loss (called weight nadir) that occurred after at least 2 months in the program. Weight nadir is a common metric used in DPP studies 17,20 and to evaluate achievement of the ≥5% goal for insurance reimbursement in the Medicare DPP. 21 Weight nadir was particularly appropriate for these analyses because the primary goal was to assess whether geography impacted a member's peak potential for achieving weight loss. Published outcomes of weight loss maintenance at 12 months for this AI-powered DPP can be viewed elsewhere. 16
The Health Resources and Services Administration (HRSA) designates HPSA areas and population groups within the United States that have a shortage of health care professionals. 22 HPSAs can be geographic areas, populations, or facilities. Geographic and Population HPSAs have a population-to-physician ratio of at least 3500 to 1 and are built from counties, county subdivisions, or census tracts. If HRSA classifies an entire county as having a shortage, the county is designated a “whole-county” shortage area. 23 If only specific subdivisions or census tracts have a shortage, then the county is a “partial-county” shortage area.
In a previous publication on the reach of the Lark DPP, the authors categorized members based on whether they lived in a county designated as a primary care whole, partial, or non-HPSA per these definitions. 12 However, for accurate weight loss comparisons, this study used the more granular census tract-level designation to better determine whether members living in partial-county HPSAs actually resided in the portion of the county designated as a shortage area.
This study also compared the weight nadir between members who lived in rural versus urban areas per HRSA's Federal Office of Rural Health Policy definitions using the list of eligible rural US zip codes from HRSA's data files. 24 In brief, the Census Bureau defines both urbanized areas and clusters and considers anything not falling into these urban designations as rural.
Secondary variables included member demographics (age, sex, race, rurality), characteristics (starting BMI, program retention), and zip code census data, 25 including median income, education, and unemployment by HPSA designation. Census data provided a proxy for these variables since this AI-powered DPP is a real-world program and does not require members to disclose these items for program participation. Finally, this study examined what percentage of members had access to an in-person DPP with preliminary or full recognition within their zip code using the current list of recognized programs from the NDPP registry. 26
Statistical analyses
The authors conducted all statistical analyses in RStudio 4.0.5. Initial descriptive analyses compared the percentages of members living in an HPSA versus non-HPSA and members living in rural versus urban areas. The authors explored how the distribution of Lark members living in HPSAs across the United States compared with the national distribution of HPSAs. For this purpose, the analysis considered the proportion of designated HPSAs in the United States for each Health and Human Services (HHS) region 1–10 (Fig. 2).
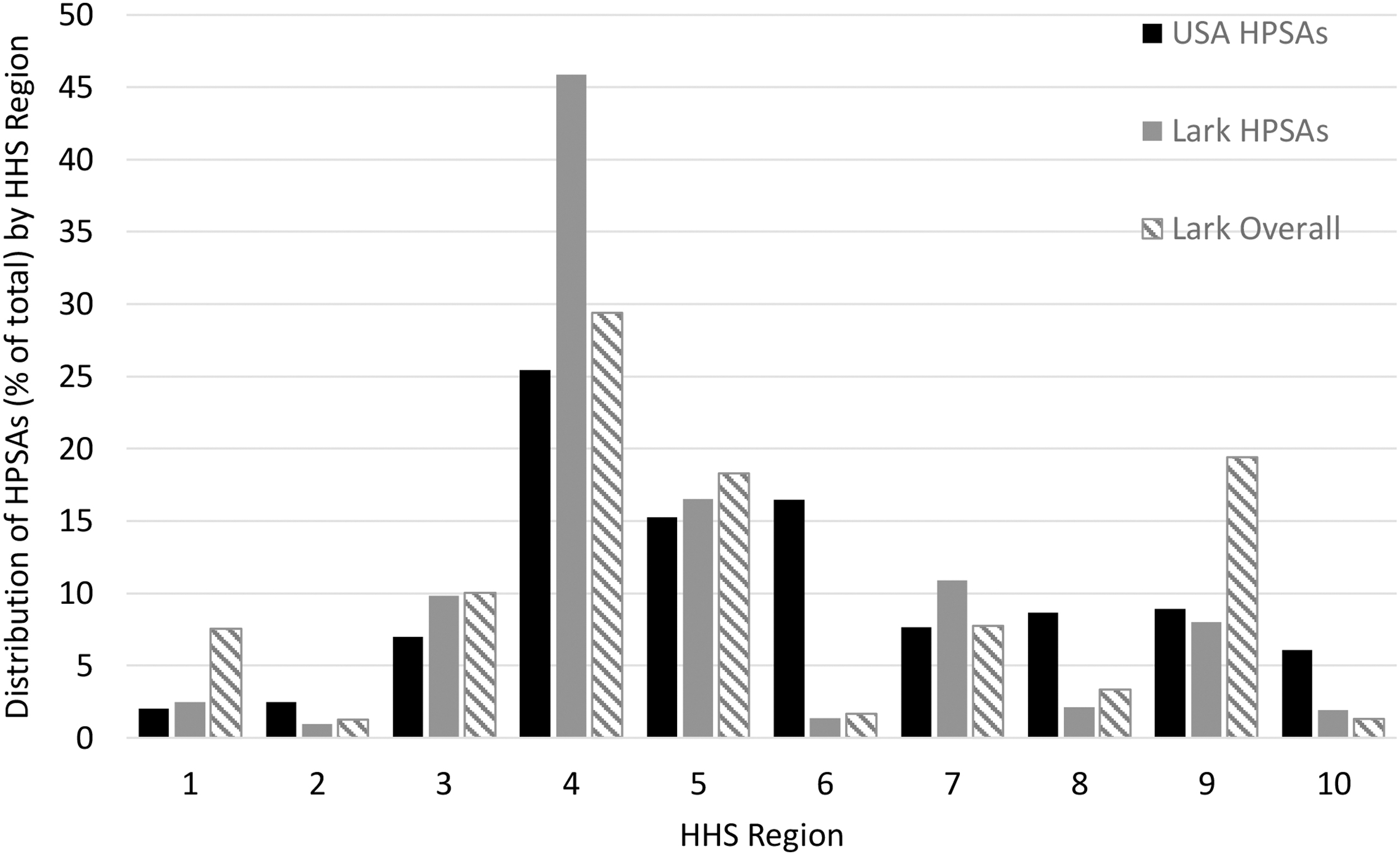
Figure demonstrating the national coverage of the Lark program in high HPSA areas. Black bars: Proportion of designated HPSAs in the United States distributed across HHS regions 1–10. Black bars sum to 100% reflecting all designated HPSAs in the United States. Solid gray bars: Proportion of Lark members living in designated HPSAs across HHS regions 1–10 out of the total Lark members living in a designated HPSA (bars sum to 100%, n = 2891). Example interpretation: The program recruited a disproportionally large percentage of members residing in an HPSA in region 4, consistent with the largest proportion of US HPSAs located in this region. Dashed gray bars: Proportion of all Lark members regardless of HPSA designation across HHS regions (n = 7266). US states in each HHS region. 1: CT, ME, MA, NH, RI, VT; 2: NJ, NY; 3: DE, DC, MD, PA, VA, WV; 4: AL, FL, GA, KY, MS, NC, SC, TN; 5: IL, IN, MI, MN, OH, WI; 6: AR, LA, NM, OK, TX; 7: IA, KS, MO, NE; 8: CO, MT, ND, SD, UT, WY; 9: AZ, CA, HI, NV; 10: AK, ID, OR, WA. HHS, Health and Human Services; HPSA, Health Professional Shortage Area.
The authors provide side-by-side comparisons for the breakdown of Lark members living in an HPSA and the breakdown of Lark members overall across these regions. The authors used unpaired t-tests (continuous variables) or chi-square tests (categorical variables) to compare all demographic and characteristic variables between HPSA designations. Finally, the authors conducted a linear regression to investigate the primary outcome of weight nadir, including HPSA status (yes/no), rural versus urban designation, age, sex, and starting BMI as independent predictors. The regression did not include race due to missing a substantial amount of data for this variable. The a priori alpha was ≤0.05.
Results
Percentage of members residing in HPSAs and rural areas
Using the more general HPSA designation of primary care whole, partial, or none of county from a previous publication, 12 there was a similar breakdown across HPSAs in this sample of members. Lark DPP members residing in an area designated as a whole-county shortage area comprised 32.7% of this sample, partial-county residents comprised 58.3%, and non-HPSA residents 9.0%. Using the more granular census tract-level designation, 39.8% (n = 2891) of the sample resided in an HPSA and 60.2% (n = 4375) did not live in an HPSA (Fig. 1).
Thus, only a small percentage of residents classified as “partial county” resided specifically in the part of the county classified as an HPSA area. Members residing in rural areas comprised 28.2% (n = 2052) of the sample and urban areas 71.8% (n = 5214). A greater proportion of members living in an HPSA also resided in a rural area (50.8%) compared with members living in a rural area not classified as an HPSA (13.3%) (Table 1). Lark members represented all 10 HHS regions, with a particularly high representation of HPSAs in regions 4, 5, and 7 (Fig. 2).
Comparisons of Sociodemographics and Characteristics for All Members Between Health Professional Shortage Area Designations
Indicates variables derived from census data. All other data collected directly from members.
BMI, body mass index; HPSA, Health Professional Shortage Area.
Comparisons of member sociodemographics and characteristics
There were observed differences in member sociodemographic variables and characteristics between HPSA designations (Table 1). Members residing in HPSAs were younger, more likely to be female and White, had a higher starting BMI, and had the lowest income and percentage college-educated compared with those living in non-HPSAs. These results did not differ when comparing the members residing in HPSAs versus non-HPSAs who provided weights for analysis of weight loss and those who did not provide weights (all P > 0.05).
Weight loss by HPSA and rural versus urban designation
There were no observed differences in weight loss by HPSA or rural/urban designation (Fig. 3). Results of the linear regression indicated that the only significant predictor of weight nadir was sex (β = 0.13, P = 0.04), with male sex predicting greater weight loss. HPSA status, rural/urban designation, age, and starting BMI were nonsignificant (Ps 0.15–0.69). There were also no observed differences in the number of members achieving ≥5% weight loss or the time in the program until the achievement of the weight nadir (Table 1). Members residing in both HPSAs and non-HPSAs achieved the weight nadir on average 6 months into the program, which is consistent with the program goals since the first 6 months of the DPP is the active weight loss phase. 18
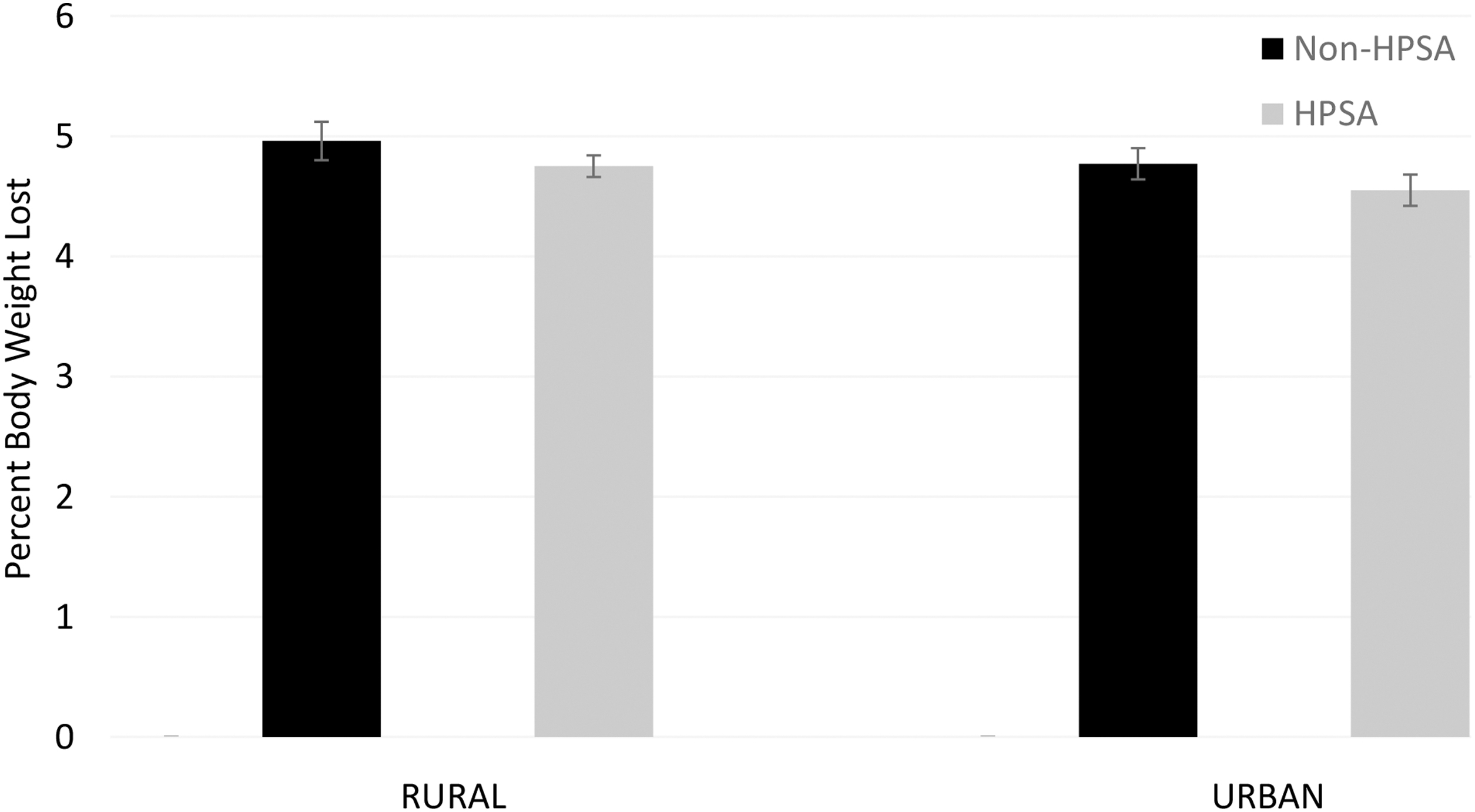
Mean (SE) percent weight loss by HPSA and rural versus urban designations. Coefficients for HPSA status and rural versus urban were not significant in the model predicting percent weight loss. SE, standard error.
Although the same relationships persisted for all variables presented in Table 1 when broken down by HPSA status for both the group of members who provided weights for analysis of weight loss and those who did not, there was a significant difference observed in the proportion of members who provided a weight based on HPSA status, χ 2 (7266) = 16.9, P ≤ 0.0001, with a smaller proportion of members residing in an HPSA providing a follow-up weight (83.5%) compared with those who did not reside in an HPSA (87.0%).
Access to an in-person DPP
Only 10.1% of Lark members had access to an in-person DPP with preliminary or full recognition from the CDC within their zip code. Of the 10.1% of members who did have access to an in-person program within their zip code, the majority resided in urban areas, with only 28.4% located in rural areas.
Discussion
This study evaluated weight loss for members of an AI-powered DPP living in HPSAs versus areas with sufficient care providers and for members living in rural versus urban areas. The primary hypothesis was a lower percent weight loss for members living in HPSAs and rural areas due to known barriers to diabetes care. 13,14 Contrary to this hypothesis, there were no observed differences in weight loss based on HPSA or rural versus urban designations.
There has been much speculation about the potential for digital technologies to reach underserved populations but little evidence of outcomes. 27 This study provides evidence that despite socioeconomic differences, individuals living in HPSAs and rural areas adhered to a fully digital DPP and achieved clinically meaningful weight loss that did not differ from that of members living in areas with more convenient access to health care and resources. The rural versus urban findings of this study are consistent with those of Mench et al, 28 who compared weight loss and engagement between adult participants of an online behavioral intervention residing in rural versus urban areas and observed no statistically significant differences based on rurality.
This study extended upon this literature by adding results pertaining to HPSA status and explored a larger geographic area than Mench et al, 28 which was limited to Vermont and Arkansas. The reach of the fully digital program investigated in this study is an important finding because only 10.1% of members had access to an in-person DPP with preliminary or full CDC recognition within their zip code. In addition, 57% of members lived in HHS regions 4–7, corresponding to areas with the highest incidence of type 2 diabetes in the United States. 9
Lacking easy access to a primary care professional is a challenge for all but can be especially harmful to those managing a chronic health condition such as prediabetes.
Living in areas with easier access to a primary care physician is associated with increased primary care visits and fewer urgent care visits, 29 fewer chronic conditions, 7 and lower rates of potentially avoidable hospitalizations. 30 If access to primary care is suboptimal, alternative services are essential. Weight loss is also a key predictor of reduced type 2 diabetes risk and an important area of primary prevention for individuals living with prediabetes. 31 Members living in an HPSA had the highest starting BMI in this study, suggesting the greatest risk of developing type 2 diabetes among the included members. 32 Despite this increased risk, there were no observed differences by HPSA status in percent weight loss, the time it took to achieve the weight nadir, or the percentage of members who achieved the NDPP goal of ≥5% weight loss.
There are other remote options to deploy the DPP, including telehealth. 33 Telehealth models provide remote access to the DPP; however, there are important differences between AI-powered programs and telehealth. Telehealth models retain the original group-based structure of the DPP, as members attend lessons along with their cohort companions, and lessons are facilitated by a human lifestyle coach. 34 Similar to in-person programs, telehealth DPPs still require costly staffing and class sizes can impose scheduling conflicts and place caps on enrollment.
Futhermore, the group-based structure of Telehealth DPP models makes offering personalized coaching to each member difficult. In contrast, an AI-powered DPP can accommodate a large capacity with minimal staffing resources since the educational content is delivered through an AI coach, which enables maximum scalability. There may be additional unique benefits associated with AI-powered DPPs such as synchronous and immediate feedback, encouragement, and personalized and data-driven recommendations provided to each member of the program.
Study strengths and limitations
A strength of this study is that it is one of the first studies to compare weight loss of an AI-powered DPP for individuals living in HPSAs and rural areas and a substantial portion of members (∼40%) resided in an HPSA. The program reached members living in HHS regions with a high density of HPSAs, 35 and 28.2% of members lived in rural areas, which is a bit higher than the overall US rural population. 24 In terms of limitations, this study was retrospective in nature; however, these data reflect the real-world implementation of a digital DPP in the target population.
This commercial program did not require members to disclose their socioeconomic data for program participation, so census data provided a reasonable proxy. The inclusion of these data provided important estimates to better understand the population represented in this study. Notably, none of the groups fell below the 2022 HHS poverty thresholds 36 ; thus, it is unlikely that this study included individuals belonging to a designated “severely disadvantaged” group. The authors plan to investigate outcomes for vulnerable groups such as the Medicare/Medicaid populations in future studies.
Although there were no observed differences in outcomes between those residing in an HPSA and those who did not, those residing in an HPSA were slightly less likely to provide follow-up weights for analysis of weight loss. This is an important discovery because early engagement in digital health programs helps to drive longer-term outcomes. 37,38 It is possible that some members residing in HPSAs require additional support or tailoring of coaching to increase their early engagement and facilitate the retention necessary to achieve beneficial long-term outcomes. 39
Future directions
In addition to future investigations of vulnerable groups, a remote AI-powered DPP can act as a tether between a member and their health plan and care provider. Health plans face challenges in reaching and serving members in a timely way. Staying in contact and up to date with members residing in HPSAs or rural areas presents a particularly difficult challenge. Having a remote preventive health care program available on a mobile phone may have benefits above and beyond providing education and facilitating the adoption of healthy lifestyle behaviors. For example, an AI-powered program may assist members in better managing all aspects of prediabetes by providing reminders to schedule and attend preventive health care visits such as blood pressure checks, eye screenings, and lipid profiles. This tether between the member and their health plan or care provider can serve as a conduit to maintain open lines of communication and promote adherence to a prescribed care management plan.
Future studies could explore the impact of this tether. In addition, an AI-powered DPP can deploy health screenings that can be conducted virtually (eg, mental health screenings such as the Patient Health Questionnaire, medication adherence questionnaires) and escalate members in need of additional counseling to their care provider. Future studies could also explore the results of these escalations.
Conclusions
Members of an AI-powered DPP achieved weight loss that did not significantly differ by HPSA or rural versus urban designations. Living in an HPSA or rural area was not an observed barrier to achieving clinical outcomes in this study, despite members living in HPSAs having the highest starting BMI and lowest household income and education. A fully digital AI-powered program facilitated reduced risk of diabetes through weight loss in areas where residents might not otherwise have been able to access diabetes prevention services.
Footnotes
Acknowledgments
We thank the team at Lark for their assistance in managing the data collection.
Authors' Contributions
Dr. Graham designed the study, performed analytics, wrote, and edited the article; Dr. Auster-Gussman, Dr. Lockwood, and Dr. Branch wrote and edited the article.
Author Disclosure Statement
Dr. Graham, Dr. Auster-Gussman, Dr. Lockwood, and Dr. Branch are employed by Lark.
Funding Information
No funding was received for this article.