
Abstract
Community-based organizations (CBOs) are on the frontlines offering resources and support to residents during times of distress. Through a community-academic partnership, an interdisciplinary team developed, collected, and analyzed 91 surveys from social services providers across New York City assessing the impact of the COVID-19 pandemic on their organizations' operations. The majority (93%) of these organizations stayed open during the pandemic but had to shift the services they offered to meet new needs. Although most (89%) shared they were not offering on-site testing for COVID-19, 53% expressed interest in becoming a test site, citing needs such as funding, test kits, and skills-building for staff. More than half of the respondents were eager to get involved in public health efforts in other ways, such as joining local research advisory boards. Despite increasing the services they provided, CBOs saw decreases in staffing and volunteers. Furthermore, although nearly half (48%) received governmental aid, many faced financial pressures and several had to close offices during the pandemic. As trusted resources, CBOs can help meet public health needs if provided with proper support and resources. It is critical that those working in prevention and relief are considerate about how and when they leverage effective partnerships between public health organizations and CBOs, offering organizations the resources they need to be effective in this charge, given the role they can have in promoting health equity.
Introduction
Across the country, community-based organizations (CBOs) in local neighborhoods respond to community members' needs and concerns, connecting them with the tools, services, and information they need in hopes of improving their quality of life. 1,2 Individually, CBOs have sustained trust-informed relationships with their local communities. 2,3 In addition, local government and health care organizations often partner with CBOs to better reach and engage community members. 4 Such partnerships can provide more resources to community members while cultivating trust between these health care organizations and CBOs. 3,4
Throughout history, epidemics, natural disasters, and other crises have called forth CBOs and volunteers to help. During World War II, citizens volunteered as emergency response personnel due to a shortage of professionals. 5 The AIDS epidemic in the 1980s pushed forward the importance of volunteer efforts in the gay community as homophobia stigmatized members of the community, making them distrustful of governmental intrusions. 6 Today, organizations such as the Red Cross and FEMA offer many necessities for community members during natural disasters. 7,8 COVID-19 presented another moment for CBOs to help.
In spring of 2020, New York City (NYC) was publicly deemed the United States' first epicenter of the pandemic. 9 Just 3 weeks into March, the state's Governor closed businesses deemed nonessential. 10 People were confined to their homes, 11 and a barrage of unemployment claims commenced with >1.6 million New Yorkers filing for unemployment from March through mid-August of 2020. 12 The virus, meanwhile, continued to spread; in the first 3 months, NYC saw >200,000 cases of COVID-19. 11
CBOs who participated in the current study's NYC-based Research-to-Action Network 13 remained hard at work meeting their communities' needs, but these partners were quick to note both the growing needs of their communities and the many operational shifts they had to make that required them to be more nimble than ever. Members wondered how the local organizations helping NYC's community members were managing and how they would continue to fare as the pandemic decimated New York.
Although The Independent Sector produced one of the first and only studies, to the research team's knowledge, to provide some insight into the tremendous financial burden of the pandemic on mid-sized and larger-sized organizations nationally, 14 information about how local CBO operations were being affected, financially or otherwise, remains difficult to find. Aside from individual reports from organizations such as the New York Community Trust that detail how organizations across the city used the $110 million they were gifted in 2020, 15 there remains minimal literature exploring CBOs' contributions and stressors during the pandemic. There is also a limited understanding of how or if the impact of CBOs could have been better maximized during the pandemic.
The research presented in this article was born out of a larger community-based participatory research project that engaged community partners in the creation and implementation of locally relevant COVID-19 research. 14 States such as Minnesota 16 and cities such as San Diego 17 were surveying organizations in their communities to understand the ongoing impacts of COVID-19 on their operations, but this project's partners noticed the lack of such data in NYC. The Minnesota Council for Non-Profits, in documenting their own findings across time, articulated the need for organizations and key stakeholders to have such data to (1) look at individual organizations within a larger but still local context and (2) determine next steps for supporting organizations in meeting growing demands.
This article presents a descriptive landscape analysis of what local community organizations in NYC were doing in the early stages of the pandemic to adapt while continuing to meet their constituents' needs, some of the fears they held about the future, and what all of this meant not only for their communities, but for their staff. It also highlights, in retrospect, missed opportunities for engaging partners in some direct efforts to slow the spread of COVID-19 while also identifying a clear need to better understand why some organizations might be hesitant to engage in certain efforts.
Methods
In March of 2020, a Research-to-Action Network of >100 community and academic partners in NYC came together to understand how the pandemic was impacting New Yorkers. 14 As part of this work, the research team collaboratively developed a survey of local CBOs to understand how they were faring in the face of the pandemic amidst the strain that COVID-19 was putting on their constituents. First, key community and academic investigators identified domains for the survey, including organizational information, and current and anticipated future effects of COVID-19 on operations, workforce, demand, safety, and finances.
The researchers then sent an open invitation to all Research-to-Action Network participants asking them to join a workgroup focused on survey development, recruitment, and analysis. Twelve partners joined the effort. At the first workgroup meeting, partners reviewed the survey's goals, discussed a sampling strategy and survey timeline, and suggested edits and additional items to consider in the survey, including questions about any new opportunities or partnerships that may have emerged. The final version of the survey assessed populations served, operations during COVID-19, and workforce considerations, including morale, service demand, future outlooks, and financial concerns. After piloting, the workgroup programmed the survey into REDCap, a web-based program for secure surveying (Supplementary Data). 18
In early July 2020, the research team shared the survey with members of the Research-to-Action Network through e-mail and provided language they could use when disseminating the survey to other community or social service organizations. Eligibility criteria were expansive, liberally defining CBOs to include any organization in NYC providing social services to local communities. An analysis subgroup generated descriptive statistics to summarize the characteristics of the participating CBOs and the broad range of impacts COVID-19 had on them.
Results
Overview of participants
During July 2020–April 2021, the Research-to-Action Network reached out to 100 organizations and received 91 survey responses from 88 unique organizations. For 4 organizations, >1 representative completed the survey, reflecting different employees' perspectives. The majority of responses came from individuals in leadership, including executive leaders (54%) and managers (29%). Most were medium or large in size (ie, 31% reported an annual revenue between 1 and 5 million dollars, and 25% reported an annual revenue between 10 and 50 million dollars). CBOs served populations in all 5 boroughs of NYC: 43% served residents of the Bronx, 36% Manhattan, 36% Queens, 36% Brooklyn, and 24% Staten Island.
Before the pandemic, organizations primarily served children/youth (70%), families (68%), racial, ethnic, and/or religious minorities (66%), seniors (57%), and immigrants and refugees (54%), as shown in Figure 1. Their services included human (55%), health (53%), community support and development (48%), mental health (43%), and education and child development (39%). Most (69%) reported being essential service providers, meaning that they were exempt from the NYS On Pause Executive Order, 11,12 and could stay open to serve their clients.

Populations served by participating CBOs before COVID-19. CBOs, community-based organizations.
General service provision during COVID-19
Most (65%) noted that they were extremely concerned about the long-term effects of COVID-19 on their CBO's clients (morbidity, mortality, financial difficulties, and access to health care). Services their clients had difficulty accessing in the early phases of the pandemic included health (reported by 43% of respondents), mental health (45%), education and child development (40%), housing support (39%), and emergency food (35%).
The majority (93%) remained open for new clients during the pandemic. Some (33%) limited the numbers of new clients, 39% maintained their client base, and 21% increased their client base.
In response to the increased need, 55% offered additional or new services with food provision (52%) and financial assistance (26%) most cited. Figure 2 demonstrates the growth in the top needed services provided. Some (30%) had to reduce programs or services because of financial pressures during the pandemic. Less than half (42%) were moderately ready to return to full operations considering state and federal reopening guidance.
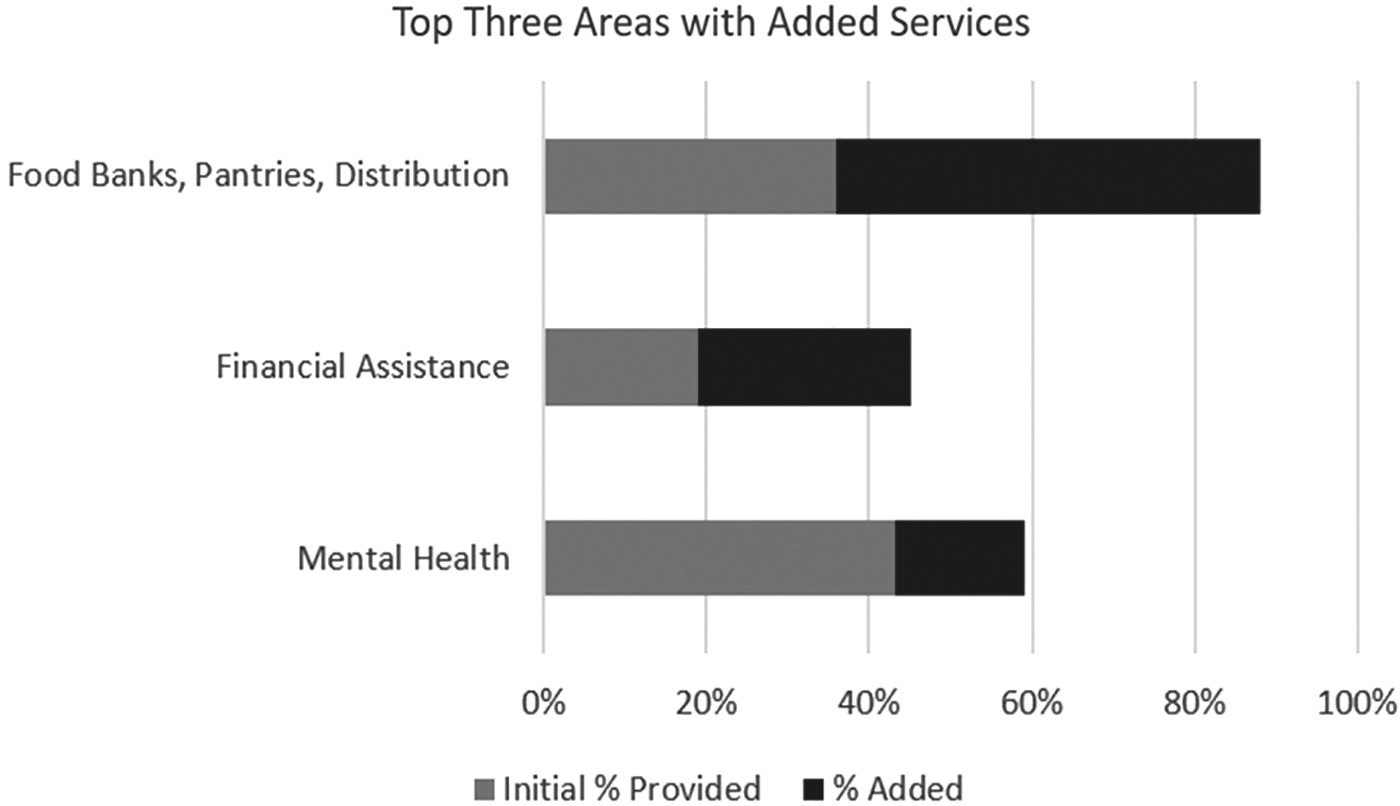
Growth in the 3 services most commonly added by community-based organizations during the COVID-19 pandemic.
More than half (54%) had difficulty acquiring personal protective equipment, and 27% needed thermometers, 32% needed cleaning/disinfection products, and 27% needed hand sanitizer.
COVID-19-specific service provision
Participants noted barriers community members faced related to COVID-19 testing, including not having enough information about testing (54%), limited access to tests (49%), and fear (46%). Although most respondents (89%) stated that their CBO was not offering on-site testing, 53% were somewhat or very interested in becoming test sites. Seventy-six percent were already promoting COVID-19 testing and/or referring their clients elsewhere for testing. To support testing and related promotional initiatives, CBOs reported they would need funding (76%), COVID-19 testing kits (67%), skills-building and COVID-19 training opportunities for staff/volunteers (67%), information about local test sites (68%), and tailored promotional materials for clients (74%) (Fig. 3).
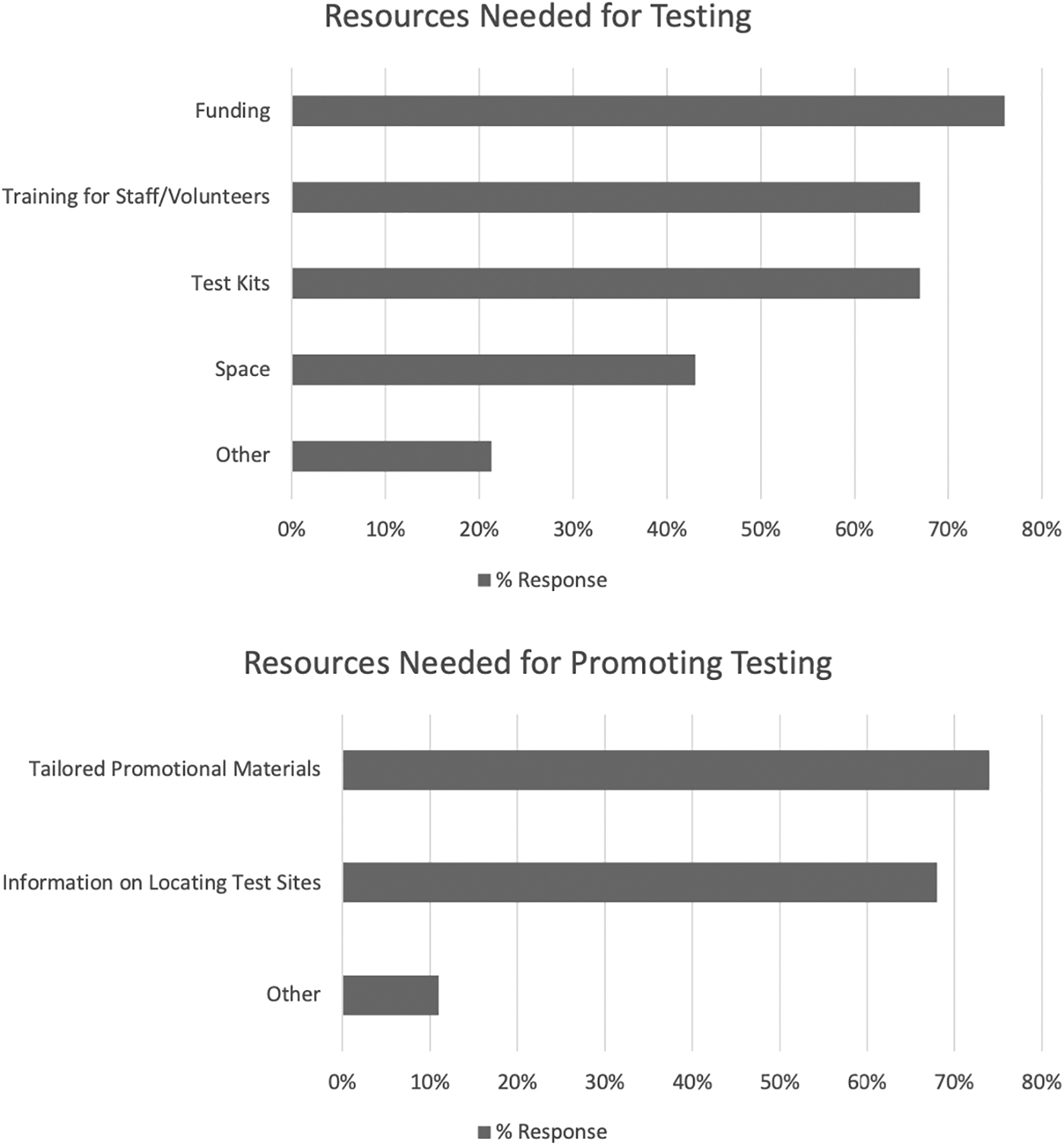
Needs that organizations documented for becoming testing sites or promoting testing resources.
Among those few who selected “other” when asked about on-site testing resources, open-ended responses included the need for personal protective equipment or explanations that they did not think their space was suitable for testing and/or that they were embedded within a larger hospital system that offered testing. The most common additional need participants identified when considering promotion of testing services was availability of materials in clients' languages.
Forty-seven percent of participants indicated they were not at all interested in becoming test sites, and 24% of organizations were not referring their constituents to other test sites. In addition, of the organizations that were not referring to testing, there was mixed interest in offering these referrals with many respondents (45%) being only somewhat interested in this.
Beyond direct COVID-19 prevention work, many participants were interested in supporting public health in other ways. When asked if they were interested in getting involved in COVID-19 and non-COVID-19-related research, 84% expressed at least some interest with 24% being extremely interested. Figure 4 shows participant preferences for participation in the research process. Although joining research advisory boards (57%) and disseminating research findings to help their communities (47%) were the most common responses, there was interest in getting involved with research in other ways. Related, when participants were asked about capacity-building opportunities that would be helpful for them, in addition to a strong interest in adapting programs/services for delivery (74%), 47% of participants wanted support in developing needs assessments, 40% identified program evaluation needs, and 33% were interested in building survey development skills.
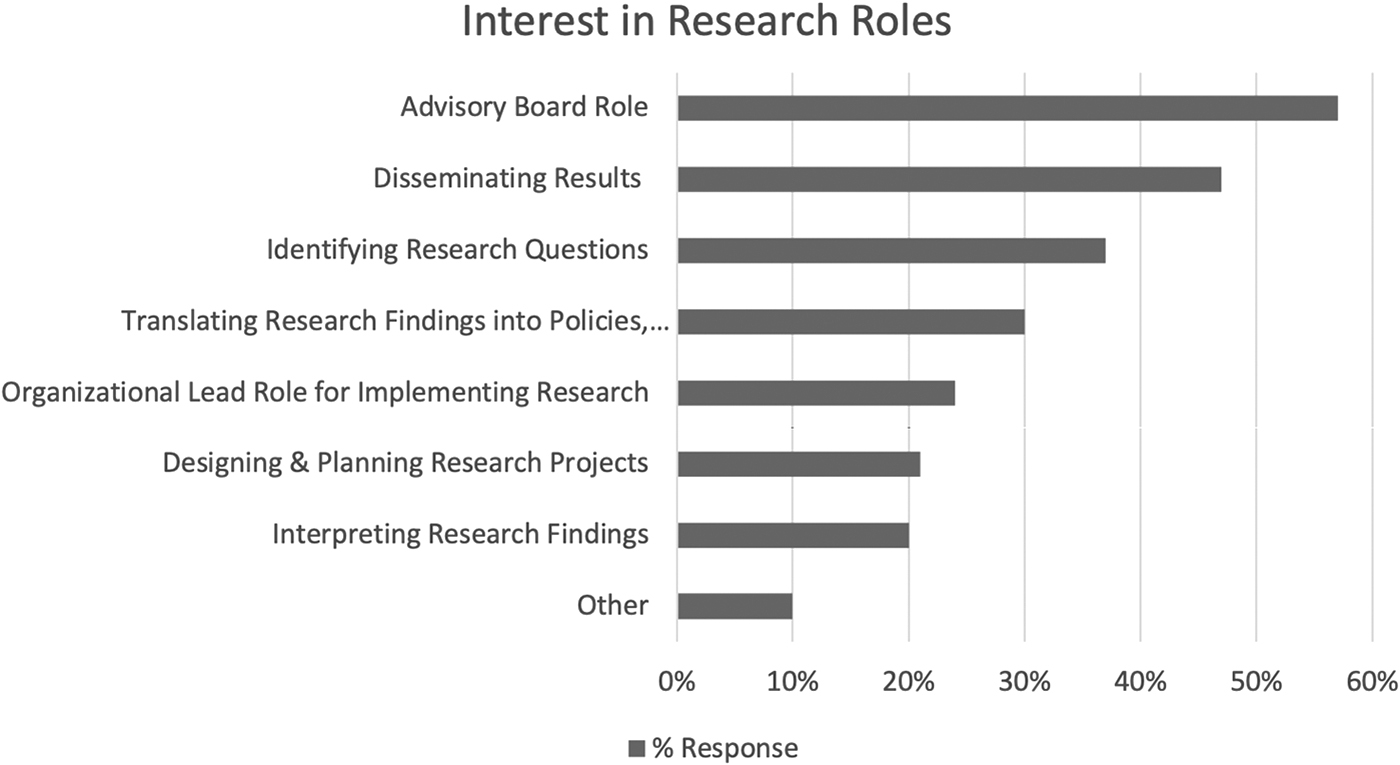
Participating CBOs' interest in research roles. CBOs, community-based organizations.
Personnel
Despite increases in services provided, CBO staff began working remotely, 69% at least part of the time and 56% completely. Many staff members (56%) switched to televisits with clients for health services, case management, and other services. Staggered staff schedules (47%) and reduced hours for staff (36%) were also common. At the worst of the pandemic, only 9% of the CBOs reported experiencing workforce disruptions or reductions directly due to COVID-19 illness. There were also some changes to their volunteer bases with 39% reporting decreases in volunteers.
During the pandemic, CBOs also provided additional services to their staff: 52% expanded sick leave, 42% provided or increased staff mental health services, and 42% offered additional training related to COVID-19. Still, 37% of the respondents indicated that the morale of their staff declined during the pandemic.
Funding
Since the start of the pandemic, almost half of the respondents (48%) received increased aid through Congress' approved Paycheck Protection Plan, 41% received an increase in philanthropic donations, 21% reported an increase in loans, and 40% did not use any loans to fund their expenses. However, due to financial pressures, 38% had to close offices or program sites, 31% furloughed employees, and 30% reduced their hours of operation. Despite increasing services and the significant financial challenges, 50% did not have fees for their self-paying clients and 28% decreased their fees. Furthermore, most (76%) were concerned that their CBO may not be able to continue to operate (57% slightly and 19% extremely concerned).
Discussion
A community-academic partnership designed, implemented, and analyzed a survey of nearly 100 CBOs across the 5 NYC boroughs, representing some of the hardest hit populations, to determine how the early days and months of the COVID-19 pandemic impacted their organizations, and what their response has been. Perhaps unsurprisingly, given the established dedication CBOs have shown to their communities during distressing times, 5 –9 this study found that CBOs continued to offer, and even to expand, their services despite the dire consequences of COVID-19 on both their finances and personnel, NYC communities faced a myriad of challenges in the early phases of the pandemic.
For example, Black and Latine New York youth experienced barriers to accessing mental health services, including inadequate health insurance, language barriers, and stigma and biases toward people of color. 19 The burden of food insecurity grew 36%, with 1 in 4 children facing food insecurity, 20 and 11% of adults in the greater NYC area reporting not having enough to eat. 21 In addition, 34% of residents in the greater NYC metropolitan area reported that they missed their mortgage or rent payment in the last month and/or lacked confidence that they would be able to pay on time in the coming month. 22 CBOs, as shown in this survey, stepped forward to respond to these challenges by increasing mental health, food services, and financial support for housing regardless of the stress it put on their operations.
CBOs and the response to COVID-19-related health concerns
This survey also asked CBOs about their role in addressing COVID-19 prevention needs more specifically. Given their status as trusted entities working on the ground to meet constituent needs, the research team wanted to assess their interest and capacity for supporting testing and research efforts. The findings provide opportunity for reflection on how CBOs should be leveraged during major health crises such as COVID-19. However, when examined within the larger context of everything CBOs were already doing during a time of financial pressure and morale tensions, considerations over such questions become potentially nuanced.
Centuries of systemic inequities have meant that racial minorities experience higher rates of chronic medical conditions, 23 disproportionately work in higher-risk environments, and live in crowded urban neighborhoods, 24,25 all risk factors that contributed to the disproportionate COVID-19 rates documented among such communities. 23 As many of the CBO sites engaged in this project were working additional hours, located in neighborhoods where case rates were soaring, and interacting more with clients than usual, they would have been well positioned to offer testing services to communities most at risk and with least access to testing during a time when this was the main defense mechanism in the fight against COVID-19. Given that finding a testing site in NYC was confusing and overwhelming at the start of the pandemic, with long wait times and few appointments, particularly in Black and Latine neighborhoods, 26 CBO support in linking people to test resources could have gone a long way.
Their survey responses indicate that the majority of the CBOs did see testing linkages as a part of their responsibility but often had inadequate resources needed to support these efforts. Many CBOs wanted to play an even larger role in pandemic prevention efforts through education and testing, but nearly 70% of the CBO leaders surveyed said they would require additional resources, particularly funding, to support such efforts. Despite expressing interest in becoming test sites, they also noted other significant barriers likely to limit their contributions, including not having enough information about testing, limited access to tests, and fear.
The NIH and others prioritized community-academic partnerships for test and trace efforts early on 27 and are currently supporting robust community-centered initiatives on vaccine equity, such as the Community Engagement Alliance Against COVID-19 Disparities. 28 However, responses from community partners suggest they were not being leveraged to support direct testing efforts and/or given the appropriate materials to support linkages to tests. It would have been reasonable to turn to local social service organizations to test, particularly given the confusion of the testing landscape early in the pandemic. 27 Perhaps there should be exploration into what building capacity for similar services might look like in advance of similar health crises in the future.
It is also important to note that although CBOs are rooted in their communities and offer opportunities for improved health outcomes at a greater scale, some CBO leaders indicated that they did not want to actively engage in direct COVID-19 testing work. Although this survey did not ask partners to elaborate on why they were hesitant about becoming testing sites, other responses about their capacity might provide hints about their reluctance.
For example, participants cited struggles with staff morale, changes in operations, and financial disruptions that suggest CBOs needed more support to actualize even their primary social service goals. Positive morale is often an indicator for success in achieving organizational goals. 29 Although CBOs tried to provide more resources to their teams by expanding sick leave and providing additional mental health support, they saw a decline in morale. As mental health outcomes worsened across the city, 30 it cannot be expected that those on the frontlines serving their local communities would be exempt from feeling such burdens, which may contribute to morale decreases.
As morale worsened and responsibility increased, CBOs also lost many of their staff and volunteers. Although the drastic reduction in the number of volunteers could have been due to safety concerns, other cutbacks (eg, furloughs and firing) were largely the result of a dramatically altered financial landscape documented in the results. Although some received aid that may have allowed operations to continue, small or mid-sized organizations, in particular, struggled to provide the same quality of services to more clients with fewer funds.
On a national scale, many programs were developed to help alleviate the major financial strain that CBOs were experiencing. Several loan and emergency grant programs were developed, including Congress' Coronavirus Aid, Relief, and Economic Security Act (CARES). 31 Philanthropy was also at a high; the Center for Disaster Philanthropy (CDP) found that in the early half of 2020, philanthropic organizations across the world gave nearly 12 billion dollars in funding to COVID-19 relief efforts, with nearly 8 billion dollars going to the United States. 32
Although the CDP notes that this was exponentially more than has been given during any other recent disaster, they also expressed concern about how the funding was, or was not, designated, observing that despite an increased focus on health disparities exacerbated by the pandemic, many of the funds lacked guidelines around supporting the most vulnerable communities. 32 Although some funders developed COVID-19 response funds that CBOs could leverage to provide relief for their struggling communities, 33 the CDP's report shows that most of the funds were not allocated to local small organizations providing their constituents with resources to support everyday and emerging needs. 32
Given the multitude of stressors facing community partners, it may be unrealistic to expect that all, or even the majority, should or can pivot to supporting direct care or response efforts. However, understanding partners' perspectives about getting involved in such ways (or not) should be further explored.
Conclusion
A poll conducted during the pandemic found that trust in traditional public health institutions is lacking, with just more than half of the respondents reporting that they have “quite a lot of trust” in the Centers for Disease Control and Prevention and only a third feeling similarly about the U.S. Department of Health and Human Services. 34 In contrast, the commitment that CBOs have to their communities make them trusted spaces for community members, further supporting the argument that high-investment authentic partnerships between CBOs and public health professionals have tremendous potential to impact health outcomes and disparities. For decades, researchers, funders, and others with concerns about health equity have been urging such partnerships, citing the importance of trust at the local level. 35
It is evident that public health crises, such as the one brought forth by COVID-19, necessitate proper funding and support for community organizations from larger health and government organizations. The results from this study suggest that local organizations were working hard to meet growing demands, and that their work, even if not directly geared toward stopping the spread, was important. Given that CBOs are well positioned to support the communities they serve, there is also opportunity to equip CBOs with what they need to help handle future public health crises more rapidly provided that they have the interest and capacity to help with direct prevention work.
Building a public health system with community members and CBOs at its core has always had the potential for vastly improving the overall health of communities; it is thus critical that public health researchers and governmental entities continue to share resources and build partnerships while anticipating CBOs' funding and other needs so that they can collaboratively and proactively address emergent community challenges. It is further critical, however, that public health practitioners have honest conversations with their CBO partners about what they envision their role in future health crises may be and that those working to improve community health are increasingly mindful of the many demands these organizations are balancing to serve their communities.
Authors' Contributions
Madden, Robinson, Leto, Cortez-Weir, Mohamed, Privett, Horowitz, and Vangeepuram contributed to the conceptualization and design of this study, with Privett as the Principal Investigator. All authors reviewed the results, contributed to the manuscript, and reviewed the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This was an internally supported project, funded by the Icahn School of Medicine at Mount Sinai.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.