
Abstract
The United States is facing a maternal health crisis with increasing rates of severe maternal morbidity and mortality. To improve maternal health and promote health equity, the authors developed a novel 2-generation model of postpartum and pediatric care. This article describes the Two-Generation Clinic (Two-Gen) and model of care. The model combines a dyadic strategy for simultaneous maternal and pediatric care with the collaborative care model in which seamless primary and behavioral health care are delivered to address the physical health, behavioral health, and social service needs of families. The transdisciplinary team includes primary care physicians, nurse practitioners, psychiatrists, obstetrician-gynecologists, social workers, care navigators, and lactation specialists. Dyad clinic visits are coscheduled (at the same time) and colocated (in the same examination room) with the same primary care provider. In the Two-Gen, the majority (89%) of the mothers self-identify as racial and ethnic minorities. More than 40% have a mental health diagnosis. Almost all mothers (97.8%) completed mental health screenings, >50.0% have received counseling from a social worker, 17.2% had a visit with a psychiatrist, and 50.0% received lactation counseling. Over 80% of the children were up to date with their well-child visits and immunizations. The Two-Gen is a promising model of care that has the potential to inform the design of postpartum care models and promote health equity in communities with the highest maternal health disparities.
Introduction
The United States is facing a maternal health crisis with rates of severe maternal morbidity (SMM) and maternal mortality (MM) continuing to increase. 1 The United States MM rate is the highest among all developed nations in the world. 2 Maternal health outcomes are particularly bleak for Black women who experience alarmingly high MM compared with White women (55.3 vs. 19.1 per 100,000 live births in 2020). 3 In Illinois, Black women also have disparate SMM rates (132.4 vs. 59.8 per 10,000 delivery hospitalizations). 4
The disparities in Illinois reflect the national maternal health landscape. Black women living in Illinois were 8 times as likely as White women to die of a pregnancy-related medical condition in 2016–2017. 4 Furthermore, COVID-19 disproportionately affected Black and Hispanic pregnant women with higher rates of severe disease. 5 –10 Nearly 70% of pregnancy-associated deaths occur postpartum. 1,4
Nationally, and in Illinois, mental health disorders, including substance use disorders, are the leading cause of pregnancy-related deaths (ie, the cause of death was related to the pregnancy), and almost all deaths are potentially preventable. 3,4,11 There is a salient difference by race and ethnicity in the contribution of mental health disorders to pregnancy-related deaths. For example, in Illinois in 2016–2017, the burden of mental health disorders was substantially greater for White (64%) and Hispanic (56%) women than for Black (13%) women. 4
Mental health disorders can surface during the perinatal period or existing conditions can be exacerbated by pregnancy. 12 Perinatal mental health and substance use disorders often are undiagnosed and untreated which can lead to a multitude of negative consequences for women including suffering, symptoms worsening, and is potentially fatal for some (ie, suicide, unintentional poisoning/overdose). 13 Maternal outcomes have substantially worsened during the COVID-19 pandemic, including poorer mental health and increased rates of substance abuse. 14 –18
Although the exact cause is unknown, evidence indicates that mental health disorders result from a dynamic mix of biological, socioenvironmental, and psychological factors across the life span. 19 Low socioeconomic status, interpersonal problems, ongoing adverse life events, chaotic social relationships, and high-stress levels represent a constellation of risk factors that result in deleterious perinatal mental health. 20,21
Reducing SMM and MM and improving maternal health require innovative health care delivery mechanisms that address both the physical and mental health needs of postpartum women. 22,23 Collaborative care is a health systems approach that integrates behavioral health care into primary care. 24 Collaborative care improves both health and behavioral health outcomes, enhances access to care, is more convenient for patients, improves quality and coordination of care, and lowers health care costs. 25 –27 Although not well studied, collaborative care is a highly promising model to address the behavioral health needs of postpartum women. 28
Receiving regular health care during the fourth trimester (ie, the postpartum period) is essential for maintaining health and promptly identifying and addressing emerging or exacerbated medical and mental health concerns. 23 The fourth trimester is a critical period for women as they adapt to physical, psychological, and social changes. To reduce SMM and MM, the American College of Obstetricians and Gynecologists recommends postpartum care be offered as an ongoing process, rather than a single visit, and that all women have contact with their provider within the first 3 weeks after birth. 23
Timely care is particularly important for women with chronic medical and/or mental health conditions. However, many women do not receive postpartum care as recommended. 29 In fact, among some low-income populations, fewer than 60% of women receive a single postpartum visit. 30
Many postpartum women prioritize their infant's health care over their own. 31 More than 85% of infants receive the recommended well-child visits in the first 6 months, and these pediatric visits represent the most regular contact postpartum women have with the health care system. 32 The American Academy of Pediatrics periodicity schedule recommendations for preventive infant health care are 3–5 days post hospital discharge and 1, 2, 4, 6, 9, and 12 months of age. 33 The periodicity schedule coincides with postpartum care recommendations, which presents an ideal opportunity for integration of postpartum and infant care.
Despite the growing evidence about feasibility and maternal acceptability of linking postpartum and pediatric care, this practice has not been widely implemented and few studies have explored a 2-generation approach to increase postpartum care utilization and improve maternal health. 34,35 The goal of this article is to describe an approach to building an innovative postpartum model of care called the Two-Generation Clinic (Two-Gen) in which postpartum mothers and their children simultaneously receive comprehensive collaborative care.
Methods
Clinic aim and setting
Two-Gen was designed to address unmet health and behavioral health needs among postpartum mothers, especially those at risk for adverse outcomes during the postpartum period. The aim of Two-Gen is to deliver integrated, comprehensive postpartum care to mothers and their children. The clinics are located within a combined Internal Medicine and Pediatrics Clinic Settings University of Illinois Hospital and Health Sciences System (UI Health) in Chicago, Illinois. The Primary Service Area comprises 53 of the 77 community areas in the city of Chicago and covers approximately 2 million individuals, including some of the poorest, lowest-resourced communities with high rates of racial residential segregation and violent crime. 36
Two-Gen has locations on the West Side (opened 2020) and South Side (opened 2021) of Chicago where Black women bear a disproportionate burden of death and disease, and experience alarmingly high levels of SMM and MM. 4,36 Two-Gen was designed to systemically address inequities by offering a model of population health that provides comprehensive screening and services to address the health, behavioral health, and social service needs of postpartum mothers and children.
Clinic patients
The model of care was designed to provide care to a woman and child as a dyad. However, to fully meet the needs and preferences of each family, the clinic is available to postpartum mothers, newborns, other children, and fathers. Families can join at any time, and the clinic does not restrict the number of days or months postpartum or age of the child. In addition, families can continue to receive care indefinitely. Potential patients are identified by medical center clinicians or staff and a referral is sent through the electronic health record. Two-Gen also has a website description of care and patients may call to directly schedule an appointment.
One social worker is responsible for all incoming referrals and contacts potential patients within 24 hours to confirm interest and schedule an appointment. To ensure coordination and seamless care delivery, the social worker assigns each patient/family to 1 social worker or care navigator who serves as the primary point of contact. Patients with identified mental health needs are automatically assigned to a social worker. UI Health accepts all Illinois insurance carriers, including Medicaid.
Model of care
The Two-Gen transdisciplinary team delivers comprehensive services that promote continuity of care with a shared goal of high-quality care over time (Fig. 1).
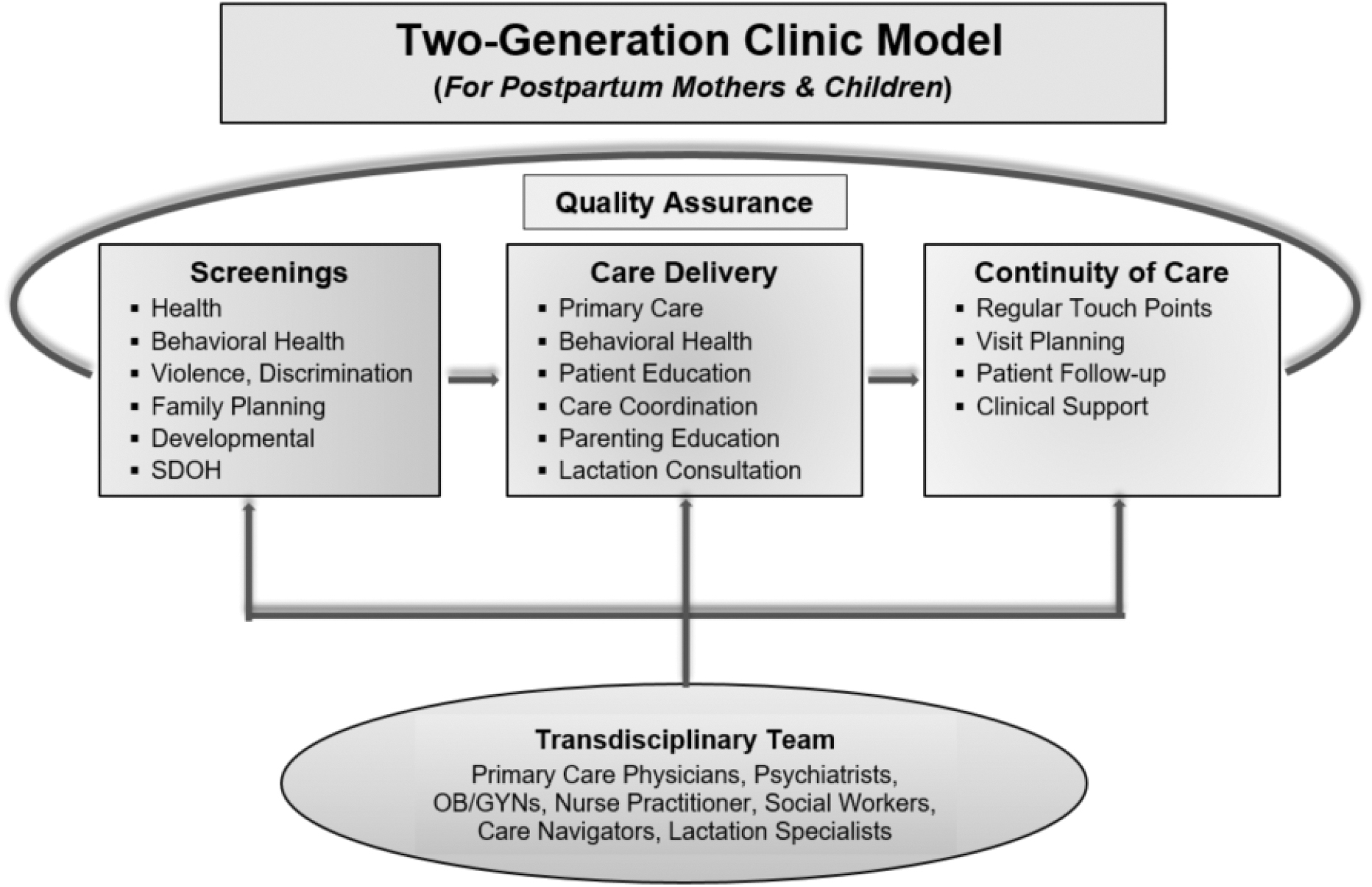
The Two-Generation Clinic model of care delivery for postpartum mothers and their children. OB/GYNs, obstetrician/gynecologists; SDOH, social determinants of health.
Transdisciplinary team
The Two-Gen transdisciplinary team specializes in maternal and child health. The team includes primary care physicians, nurse practitioners, psychiatrists, obstetrician-gynecologists, social workers, care navigators, and lactation specialists. Dyad clinic visits are coscheduled (at the same time) and colocated (in the same examination room) with the same primary care provider. All care and services provided to mothers and children are tailored to meet their individual health, developmental/behavioral health, and social service needs.
Screenings
Social workers and care navigators conduct an initial comprehensive screening to identify health, behavioral health, and social service needs. All mothers receive comprehensive screenings including mental health history, depression, post-traumatic stress disorder, substance use, interpersonal violence, discrimination, neighborhood safety, family planning, and social determinants of health (SDOH). Children receive routine comprehensive developmental screenings at scheduled intervals using standardized screening tools.
When possible, the screenings are administered by phone prior to the initial appointment. Once needs have been identified, social workers and care navigators work with the transdisciplinary team and family to collaboratively develop individualized care plans.
Care delivery
Primary care
All Two-Gen primary care providers are board certified in internal medicine and pediatrics. The physicians provide comprehensive care and primary care services to mothers, children, and family members.
Behavioral health
Comprehensive behavioral health services include psychiatry, counseling, support, and psychoeducation toward the prevention, diagnosis, and treatment of patients' mental health issues. Behavioral health is offered to mothers, children, and fathers. Two-Gen psychiatrists provide real-time psychiatric evaluation, services, and medication management to patients and consultation to other Two-Gen providers.
Licensed clinical social workers provide evidence-based psychotherapy, support, care management, and psychoeducation to patients experiencing mental health symptoms, such as depression or anxiety, trauma, stress, relationship issues, and assistance with managing mental health disorders. Providers also focus on promotion and prevention of mental health and substance use problems in mothers and social–emotional competency in children.
Patient and parent education
All mothers receive health and mental health education, including a handout about urgent postpartum warning signs and instructions about seeking immediate health care. Other individualized education includes topics such as family planning and contraception, choosing childcare, postpartum depression, nutrition, application to government assistance programs, and self-care. Parent education is provided about child development, soothing fussy babies, safety (eg, safe sleep, car seats, medication safety, child proofing), learning age-appropriate child development skills and milestones, promoting positive play and interaction between parents and children, and locating and accessing community services and supports such as home visiting programs.
Care coordination and SDOH
All patients receive care coordination. An essential cornerstone to coordination is facilitation of bidirectional communication between the patient and care team. The care navigator is the point of contact for families, and the team ensures exchange of information between all. During the intake process and ongoing, care navigators collect information about family's needs and goals, and then develop a care plan to address the needs. Special attention is focused on assessing needs and providing resources to address SDOH including benefit eligibility, housing, food security, transportation, utilities, childcare, finances, legal assistance, and access to menstrual supplies, formula, and diapers.
The care navigators and social workers provide warm handoffs, referrals, and link families to community resources. After connections to resources are provided, the team follows up to ensure that resources were obtained by families. Care navigators and social workers also schedule appointments, facilitate referrals, and ensure seamless care between settings, including inpatient to outpatient, primary and specialty care, and between Two-Gen providers (eg, social worker, physician, lactation specialist). Care navigators and social workers schedule appointments, provide appointment reminders, and monitor and follow-up care recommendations.
Lactation support
Lactation specialists provide breastfeeding education, support, and encouragement to mothers who choose to breastfeed their children. Specialists also help manage challenges (eg, pain, low milk supply, latching techniques) to support initiation and continuation of breastfeeding. Specialists provide feeding information for mothers who choose not to breastfeed, are supplementing with formula, or weaning. Lactation specialists provide in-clinic appointments, telehealth, and phone consultations.
Patient flow
Services delivered by the social worker, care navigator, psychiatrist, and/or lactation specialist are provided before or after clinical visits, based on the family needs and overall clinic schedule. Families with more urgent support needs may meet with the social worker or care navigator before the clinical visit if the physician is with another patient. The goal is to maximize services provided during a single visit while not limiting patient throughput in the clinic.
Continuity of care
Visit planning
All members of the transdisciplinary team meet weekly to collaboratively develop a coordinated plan to address the health, behavioral health, and social care needs for those patients with a scheduled appointment. Then the team reviews, discusses, and develops a detailed, coordinated plan for each patient on the schedule for the upcoming week.
Patient follow-up
During the weekly visit planning meeting, the transdisciplinary team provides updates about patients seen the previous week and to discuss follow-up and care needs. In addition, a list of high- and moderate-risk patients is maintained and reviewed weekly. The high-risk patients have significant medical, mental health, developmental, and/or SDOH needs that affect their ability to receive care. Examples include uncontrolled diabetes or hypertension, infant failure to thrive or gain weight, severe clinical depression, and child developmental delays requiring early intervention. The moderate-risk patients have needs that have been addressed, but require close monitoring. Examples include monitoring after starting a new medication, receiving mental health counseling, and multiple SDOH resource referrals.
Clinical support
Providing clinical support, training, and ongoing supervision improves the process and effectiveness of care delivery as well as support to providers. 37 The wrap-around team that includes social workers, lactation specialists, and care navigators receive extensive training and clinical support. Each team member received foundational education and training relative to his or her position (ie, social work, lactation, care navigation). In addition, team members received additional training in maternal and child health and mental health, including trauma-informed care, motivational interviewing, and implicit bias.
Many of the Two-Gen families have complex social and behavioral health needs that require a variety of therapeutic techniques and strategies. To address the complexity of needs, all team members receive individual and group supervision, and all providers have access to consultation to support their delivery of effective, high-quality patient care.
Data
Data were abstracted from the electronic health record to describe the demographic and health characteristics and service utilization of the Two-Gen mothers and children enrolled during October 2020 to January 2023. A mother or child is considered enrolled when the mother verbally agrees to join Two-Gen and has at least 1 primary care visit. Age was calculated upon enrollment in Two-Gen. Race and ethnicity were categorized as non-Hispanic Black, Hispanic, or non-Hispanic White/other. Education was dichotomized as high school degree/General Educational Diploma/or less or some college or more.
Marital status was dichotomized as married or unmarried. Employment status was dichotomized as employed (full time or part time) or unemployed. Number of children was categorized as 1, 2, or 3 or more. Hypertension, diabetes, and presence of any mental health diagnosis were each dichotomized as yes or no. These categories were not mutually exclusive, some mothers had >1 condition.
The measure of care utilization included screenings upon enrollment and at least 1 counseling session with a social worker, psychiatrist visit, or lactation counseling. Linkage to SDOH resources was measured yes or no for each family. Ever breastfed was measured yes or no. Pediatric visits and immunizations were considered up to date if the child received the American Academy of Pediatrics periodicity recommendations for care. The University of Illinois at Chicago Institutional Review Board approved this study (Protocol No.: 2022-0195).
Results
Between October 2020 and January 2023, Two-Gen enrolled 203 patients (92 mothers and 111 children). Table 1 describes the demographics, health characteristics, and service utilization of Two-Gen mothers and children. Of the Two-Gen patients, 89.1% were dyads. The age range for the mothers was 15–43 years with an average age of 27 years. The majority of the mothers self-identified as racial and ethnic minorities (56.0% non-Hispanic Black, 33.0% Hispanic, and 11.0% non-Hispanic White or other).
Demographics, Health Characteristics, and Service Utilization of Two-Generation Clinic Mothers and Children Between October 2020 and January 2023: Chicago, IL
GED, General Educational Diploma.
More than half of the mothers had at least some college (60.2%) and about half (55.3%) were unemployed. The majority of mothers were unmarried (81.4%). The majority of mothers had 1 child (58.8%). The mothers had the following conditions: 17.4% hypertension, 5.4% diabetes, and 41.3% mental health diagnosis.
Almost all mothers (97.8%) completed screenings upon enrollment. The mothers utilized the following services: 50.0% received counseling from a social worker, 17.2% had a visit with a psychiatrist, 50.0% received lactation counseling, and 26.9% were linked to SDOH resources. About 44% of children were enrolled in Two-Gen during the first month of life.
The majority of the children were non-Hispanic Black (57.3%), followed by Hispanic (33.6%), and non-Hispanic White or other (9.1%). Over 80% of the children were up to date with their well-child visits and immunizations.
Discussion
The Two-Gen model merged a dyadic strategy for simultaneous maternal and pediatric care with the collaborative care model in which seamless primary and behavioral health care are delivered to families. The Two-Gen model of integrated postpartum and pediatric care is a novel approach to improve outcomes and promote equity by comprehensively addressing the physical health, behavioral health, and social service needs of families. Postpartum mothers and children receive colocated, coscheduled care, a family-centered approach designed for convenience and to reduce care access barriers. The Two-Gen model is a multilevel approach to address the multifarious factors that can potentially lead to adverse maternal health outcomes such as chronic medical conditions, mental illness, and SDOH.
Undoubtedly, reducing maternal morbidity and MM requires addressing behavioral health needs during the perinatal period. Historically marginalized populations (eg, Black, socioeconomically disadvantaged) have a high burden of behavioral health conditions, which has been exacerbated by the COVID-19 pandemic. Collaborative care is a novel postpartum care strategy, and the few studies that have examined it focused solely on screening and treatment of depression. Indeed, integrated care is an equity strategy that increases access to comprehensive care that is otherwise difficult to access, particularly in low-resource areas where maternal health disparities are widespread.
Almost all of the Two-Gen mothers were screened to identify mental health needs, and all mothers with needs were offered services with a social worker and/or psychiatrist. Half of the Two-Gen mothers received at least 1 counseling session with a social worker. About 17% of mothers had a visit with a psychiatrist, and many more mothers are taking psychotropic medications prescribed by their primary care physician. The considerable number of mothers seeking mental health services substantiates the need for access to behavioral health care among the postpartum population.
Although further investigation is necessary, the clinical team has found that the collaborative care model described has increased access to behavioral health care for postpartum mothers that otherwise would not have access to or seek out services.
Mistrust in the health care system and providers is a deterrent to health care utilization, 38,39 and is a barrier for women from marginalized communities in seeking postpartum care, thus further increasing their risk for maternal morbidity and MM. 40 To address this mistrust, the Two-Gen team intentionally uses a relationship-based strategy by assigning 1 team member, either a care navigator or social worker, as the primary contact for the family. The team member uses a high-touch approach through regular contact with the family to establish rapport and eventually build trust.
Team members also are responsive to mothers who contact them with questions or need assistance, and reply to mothers the same day. A component of this strategy, in conjunction with the acknowledgment that trauma (eg, childhood maltreatment, community and intimate partner violence, exposure to toxic stress, racial bias) is extremely prevalent among the Two-Gen families, is practicing trauma-informed care to create an environment of emotional safety and empower families to be active partners who have choice and control in their care. 40 –42
A promising strategy to reduce health inequities is to standardize practices across populations and make the changes at the institutional level so as not to rely on individual judgment that can be biased. Thus, the authors use standardized questions and validated screening tools to systematically identify potential patient needs that require further investigation or lead to identification of needed resources. The authors speculate that mothers may fear disclosing sensitive information, especially those with a history of trauma. One successful strategy is for care navigators and social workers to follow-up with mothers after the initial visit and ask open-ended questions. The team continues to evaluate the best process for gathering sensitive information from families to identify and address their needs.
The Two-Gen providers focus on the modifiable underlying social, economic, and structural mechanisms that drive poor health and act as barriers to wellness. 22 Foremost, all families are screened during the enrollment process and ongoing for SDOH needs. Those with identified needs are immediately connected with resources. The majority of the UI Health patients are racial and ethnic minorities with public insurance, and when designing Two-Gen the team anticipated that most families would have multiple SDOH needs.
However, only about a quarter of the families reported having needs that required connections to community resources. The families have needs, but many report that they are effective at securing needed community resources. When families report a need, it is often urgent and requires immediate assistance.
Conclusions
The Two-Gen model of care is a novel model for postpartum care. Factors that are unique and important in the Two-Gen model are providing care simultaneously to mothers and their children, integration of real-time behavioral health and primary care, and providing navigation to coordinate care and address SDOH. This model of care is aimed to reduce maternal morbidity and promote maternal health. The authors continue to collect data to determine which components of the model are impactful and improve maternal health outcomes. Future outcomes from the clinic have the potential to inform the design of postpartum care models and promote health equity in communities with the highest maternal health disparities.
Footnotes
Acknowledgments
We thank the UI Health Two-Generation Clinic families. We also thank the I PROMOTE-IL team for their support of this project. We thank Lawrie Zhang for her assistance with editing.
Authors' Contributions
A.E.G. contributed to conceptualization, methodology, writing—original draft, project administration, and supervision. M.W.-S., M.A., B.H., E.H., Y.M., A.M., A.R., J.S., S.S., and S.W. were involved in project administration and writing—review and editing. A.K. carried out conceptualization and writing—review and editing. A.H. took charge of formal analysis, writing, reviewing, and editing. A.H. was in charge of writing—review and editing. R.C. was in charge of conceptualization, methodology, supervision, and funding acquisition.
Author Disclosure Statement
The authors declare that there is no conflict of interest. The authors have no potential conflicts of interest to disclose. The authors have no financial relationships relevant to this article to disclose.
Funding Information
This project was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of a financial assistance award totaling $9.5 million with 100 percent funded by HRSA/HHS (U7AMC33720). The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA/HHS, or the US Government.