
Abstract
Specific causes of mortality among various types of health care professionals (HCPs), including those characterized by age, gender, and race, have not been well described. The National Occupational Mortality Surveillance data for deaths in 26 US states in 1999, 2003–2004, and 2007–2014 were queried to address this question. Proportionate mortality ratios (PMRs) were calculated to compare specific causes of mortality among HCPs compared with those among the general population. HCPs were less likely to die from heart disease (PMR 93, 95% confidence intervals [CI] 92–94), alcoholism (PMR 62, 95% CI 57–68), drugs (PMR 80, 95% CI 70–90), and more likely to die from cerebrovascular disease (PMR 105, 95% CI 104–107) and diabetes (PMR 107, 95% CI 105–109). HCPs aged 18–64 years were more likely to die by suicide (PMR 104, 95% CI 101–107), whereas those aged 65–90 years were less likely to die by suicide (PMR 84, 95% CI 77–91), with physicians (PMR 251, 95% CI 229–275) and other HCPs having high PMR for suicide. Among all HCPs, suicide PMR was similarly increased, whereas heart disease PMRs are similarly decreased among Black compared with those among White HCPs and those among male compared with those among female HCPs. HCPs as a group and specific types of HCPs demonstrate causes of mortality that differ in important ways from the general population. Race and gender-based trends in PMRs for key causes of mortality among HCPs suggest that employment in a health care field may not alter race and gender disparities noted among the general population.
Introduction
There are over 20
In addition, although rates of specific etiologies of mortality such as suicide and deaths of despair have been investigated among various HCPs, 6,7 there are less data that compare multiple mortality causes among the broad range of HCPs. To expand on the current literature on causes of mortality in HCPs relative to the general population, the authors queried the National Occupational Mortality Surveillance (NOMS) data to report mortality causes among common types of HCPs, including causes stratified by age groups, gender, and race. An appreciation of etiologies of mortality among HCPs, as well as age, gender, and race-based differences, may have important implications for targeting resources to reduce mortality in this population.
Methods
Setting and study population
Occupation-coded US death certificate data were analyzed from the NOMS 8 data to study the mortality patterns of HCPs. The NOMS data are used to monitor changes in cause of death by usual occupation or industry over time. The NOMS data include all men and women employed in a specified occupation (work done during most of their working life), ages 18–90 years, who died at any time during the specified years of the analysis. The data set includes records for over 5.8 million deaths in 26 US states in 1999, 2003–2004, and 2007–2014.
The NOMS data were collected and pooled from 26 states cooperating with the National Institute for Occupational Safety and Health. The 26 states were Colorado, Florida, Georgia, Hawaii, Idaho, Indiana, Kansas, Kentucky, Louisiana, Michigan, North Carolina, North Dakota, Nebraska, New Hampshire, New Jersey, New Mexico, Nevada, Ohio, Rhode Island, South Carolina, Texas, Utah, Vermont, Washington, West Virginia, and Wisconsin, and were consistently represented during the study period. Information on the occupation and industry of decedents is reported on the death certificate by funeral directors, based on information provided by an informant, usually a family member. Information on the cause of death is completed by a medical certifier, who is the attending physician, medical examiner, or coroner.
Primary outcomes and analysis
This study included all decedents with the main occupation recorded as health care. Based on the way the data are presented in NOMS, HCPs were subcategorized into the following occupational categories: physicians, nurses, registered nurses, dietitians, health care support, dentists, veterinarians, optometrists, podiatrists, pharmacists, therapists, physician's assistants, dental hygienists, emergency medical technicians, physical and occupational therapists, and dental assistants.
The NOMS data can be used to conduct occupational mortality surveillance by calculating proportionate mortality ratios (PMRs) related to the specific occupation and underlying causes of death. PMRs indicate whether the proportion of deaths due to a specific cause appears to be high or low for a particular occupation, compared with all other occupations, or a particular industry compared with all other industries. This research was deemed exempt from institutional board review ethics oversight due to the public availability of deidentified data.
The PMR Query System provides age-adjusted underlying cause (and 95% confidence intervals [CIs]) of death PMRs. PMRs are calculated by comparing the proportion of deaths from a specified cause within a specified occupation or industry group with the proportion of deaths due to that cause among all decedents. PMR statistics are suppressed for occupations or industries with fewer than 5 deaths. Unemployed, students, volunteers, and those in unknown occupations or industries (<3%) were excluded from the analysis.
Analyzed PMRs (95% CI) during study periods were included for the following causes of death—infectious diseases (ICD10 coded A00–B99), malignancies (C00–C97), hematological diseases (D46, D50–D75, D89.2, I88, R72), diabetes mellitus (E10–E14), alcoholism (F10, G31.2), drug-related mortality (F11–F19), neurological diseases (G00–G99, H00–H95), hypertension (I10, I12), heart disease (I00–I52, I97.0–97.1, I97.8–97.9), cerebrovascular diseases (G45.0–45.2, G45.4–45.9, I60–I69), respiratory diseases (J00–J99), gastrointestinal diseases (K00–K93, R68.2), genitourinary diseases (N00–N99, R31), sudden death with unknown cause (R95, R96, R98), mortality due to external causes (V01–Y98), and suicide (X60–X84, Y87.0).
Results
Mortality by age groups
During the years 1999, 2003–2004, and 2007–2014 among HCP decedents aged 18–64 years, there were significantly reduced PMRs of several important causes of mortality compared with the general population, including heart diseases (PMR 87, 95% CI 86–88; P < 0.01), alcoholism, and drug-related mortality (PMR 63, 95% CI 57–69 and PMR 79, 95% CI 69–90, respectively; both P < 0.01), and external causes of death (PMR 97, 95% CI 95–98; P < 0.01). However, significant excess PMRs compared with the general population were observed among HCPs for most other causes of death, including malignancies (PMR 107, 95% CI 106–108; P < 0.01) and suicide (PMR 104, 95% CI 101–107; P < 0.01).
The highest PMRs were observed for hematological, neurological, and diabetes-related mortality (PMR 128, 95% CI 116–141; 118, 95% CI 114–122; and 112, 95% CI 108–115, respectively; all P-values <0.01) (Fig. 1A and Table 1).
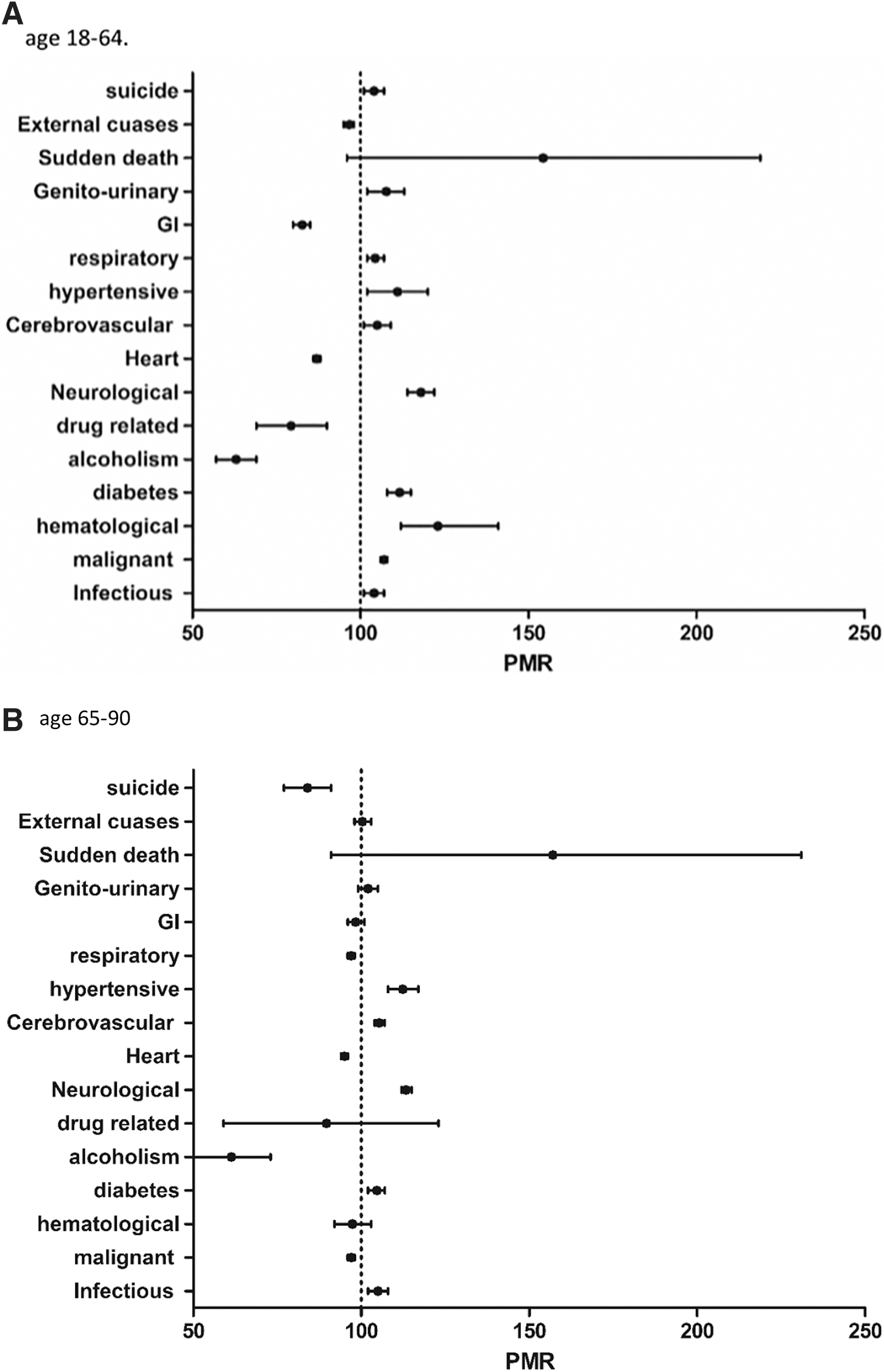
Proportionate mortality ratio—all health care professionals, by cause of death.
Proportionate Mortality Ratios: All Health Care Professionals, by Cause of Death and Age
NS, non significant.
In decedents aged 65–90 years, reduced PMR among HCPs was observed for heart (PMR 95, 95% CI 94–96; P < 0.01) and respiratory (PMR 97, 95% CI 96–98; P < 0.01) diseases, malignancies (PMR 97, 95% CI 96–98; P < 0.01), alcoholism (PMR 61, 95% CI 50–73; P < 0.01), and suicide (PMR 84, 95% CI 77–91; P < 0.01). Increased mortality rates were observed in hypertensive disease (PMR 112, 95% CI 108–117; P < 0.01), cerebrovascular disease (PMR 105, 95% CI 104–107; P < 0.01), and neurological disease (PMR 113, 95% CI 112–115; P < 0.01), infectious diseases (PMR 105, 95% CI 102–108; P < 0.01), and in diabetes (PMR 105, 95% CI 102–108; P < 0.01) compared with the general population (Fig. 1B and Table 1).
Mortality by gender/race
There was a significant differential mortality patterns among different gender and race groups (Supplementary Fig. S1). Among Black HCP women, this study found reduced mortality ratios for most cardiovascular causes, including heart (PMR 98, 95% CI 97–100; P < 0.05) and cerebrovascular (PMR 95, 95% CI 91–99; P < 0.05) diseases, compared with Black women in the general population. Hypertension (PMR 100, 95% CI 92–108; P-non significant [NS]), diabetes (PMR 103, 95% CI 99–107; P-NS), and suicide-related mortality (PMR 118, 95% CI 97–142; P-NS) PMRs did not differ in Black women HCPs compared with Black women in the general population.
Malignancy-related mortality was slightly increased in Black women HCPs (PMR 102, 95% CI 100–103; P < 0.05) as was mortality from external causes (PMR 105, 95% CI 100–109; P < 0.05).
In Black HCP men, there were increased PMRs of suicide (PMR 133, 95% CI 108–162; P < 0.05), and infectious disease (PMR 129, 95% CI 117–143; P < 0.01) compared with Black men in the general population. For most other mortality causes, including heart disease (PMR 98, 95% CI 93–102; P-NS), cerebrovascular disease (PMR 94, 95% CI 84–106; P-NS), diabetes (PMR 110, 95% CI 97–124; P-NS), and malignancies (PMR 101, 95% CI 97–106; P-NS), PMRs did not differ significantly from Black men in the general population.
White women HCPs had reduced mortality ratios for common mortality causes including heart (PMR 97, 95% CI 96–99; P < 0.05) and cerebrovascular diseases (PMR 98, 95% CI 96–100; P < 0.05), as well as malignancies (PMR 96, 95% CI 96–97; P < 0.01) compared with White women in the general population. On the contrary, compared with White women in the general population, excess mortality in White women HCPs was noted for diabetes (PMR 103, 95% CI 101–106, P < 0.05), suicide (PMR 138, 95% CI 133–142, p < 0.01, and for external causes of death (PMR 111, 95% CI 116–118, P < 0.01).
There were reduced PMRs from heart diseases (PMR 97, 95% CI 96–98; P < 0.01), alcoholism (PMR 86, 95% CI 75–99; P < 0.05), and drug-related mortality (PMR 75, 95% CI 56–98; P < 0.05) in White HCP men. Among White men, there was significant excess mortality from external causes (PMR 114, 95% CI 111–116; P < 0.01) as well as suicide (PMR 141, 95% CI 136–146, P < 0.01) compared with White men in the general population.
Differential mortality patterns by specific health care occupations
Differences in PMRs between various occupations of HCPs and the general population by specific causes of mortality are noted in Supplementary Tables S1–S15 and Figure 2A–H. For example, regarding mortality for heart disease, among all HCPs, there was reduced PMR compared with the general population (PMR 93, 95% CI 92–94; P < 0.01). This trend was also noted across most health care occupations including physicians (PMR 96, 95% CI 93–98; P < 0.01), nurses (PMR 90, 95% CI 89–91; P < 0.01), and registered nurses (PMR 89, 95% CI 88–90; P < 0.01) (Fig. 2A and Supplementary Table S1).

Main causes of death by occupation.
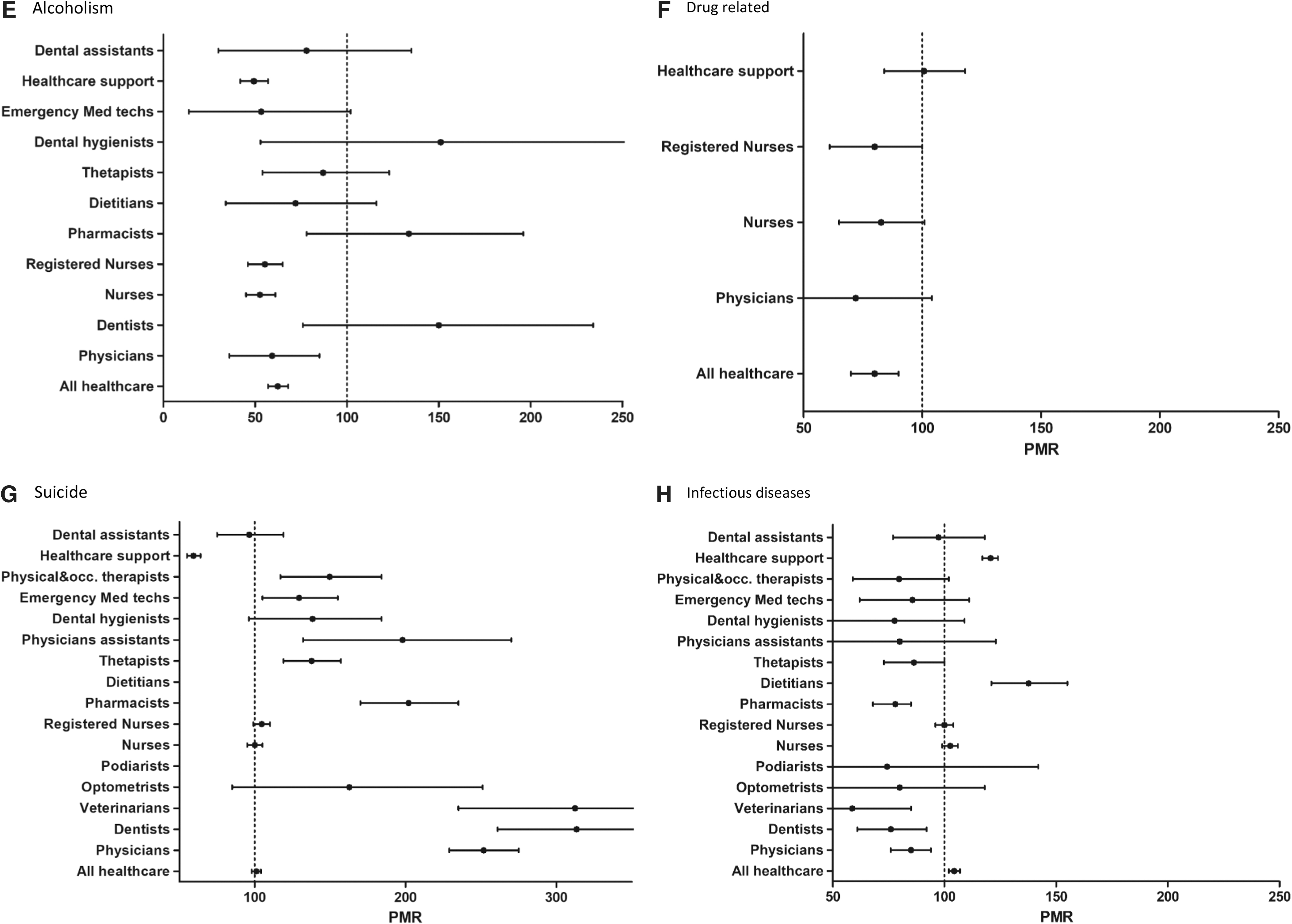
Other conditions of particular importance include mortality from alcohol, drugs, and suicide. There were decreased alcohol (PMR 62, 95% CI 57–68; P < 0.01) and drug-related (PMR 80, 95% CI 70–90; P < 0.01) mortality ratios in HCPs. Significantly reduced alcohol-related PMRs were observed among nurses (PMR 52, 95% CI 45–61; P < 0.01), registered nurses (PMR 55, 95% CI 46–65, health care support (PMR 49, 95% CI 42–57; P < 0.01), and physicians (PMR 57, 95% CI 36–85; P < 0.01).
PMR of drug-related mortality was reduced among registered nurses (PMR 79, 95% CI 61–100; P < 0.05). The drug-related PMR of physicians, nurses, and health care support did not differ from the general population (PMR [95% CI] of 76 [36–140], 82 [65–101], and 100 [84–118], respectively; all P-NS) (Fig. 2E, F, and Supplementary Tables S7 and S8).
Suicide mortality rates differed significantly between different HCP occupations. Although significantly increased suicide-related PMRs were observed among most health care occupations, physicians had among the highest rates (PMR 251, 95% CI 229–275, P < 0.01). Dietitians and health care support had significantly decreased suicide mortality rates (PMR [95% CI] of 32 [32–47] and 59 [55–65] respectively; both P < 0.01).
The suicide PMRs of nurses and registered nurses did not differ from those of the general population (PMR [95% CI] 100 [95–105] and 105 [99–110], respectively; both P-NS). The highest PMRs were observed among podiatrists, dentists, and veterinarians (PMR [95% CI] of 327 [163–585], 311 [261–368], and 307 [235–395], respectively; all P < 0.01) (Fig. 2G and Supplementary Table S9).
Discussion
This analysis from an NOMS database on the causes of mortality among HCPs compared with the general population demonstrates several important findings. HCPs are less likely to die from heart disease, alcohol, and drugs but more likely to die from cerebrovascular disease, diabetes, and infectious diseases compared with the general population. In addition, physicians and several other HCPs, including dentists, veterinarians, and optometrists, are more likely to die from malignancy and less likely to die from diabetes-related causes compared with the general population.
Compared with similarly aged individuals in the general population, HCPs aged 18–64 years are more likely to die by suicide; notably physicians had a 2.5-fold increased rate compared with the general population. Finally, among all HCPs, heart disease mortality rates are decreased to a similar extent among Black and White HCPs and among men and women HCPs compared with the general population, suggesting that working in a health care field may not alter underlying race and gender disparities seen in the general population.
Previous data that focused exclusively on causes of mortality among HCPs, particularly in the United States, have been limited. An analysis of ∼1200 physicians from 1948 to 1998, of whom >50% were smokers, identified lower all-cause mortality among male and female physicians, with lower mortality rates from heart disease and cancer, compared with the general population. 4 Prior analyses from the NOMS database from 1984 to 1995 comparing male physicians with other male professionals noted that mortality from heart disease and diabetes was similar, whereas mortality from cerebrovascular disease was greater among male physicians. 3
Findings from outside the United States noted lower mortality among physicians from diabetes and cardiovascular disease compared with the general population 9,10 Among nurses, mortality between 1984 and 1990 was lower for ischemic heart disease and similar for diabetes compared with the general population. 5 Other studies have highlighted individual causes of morality among HCPs, including from occupational exposure to infectious pathogens 11 and workplace injuries. 12
The findings of this study expand on these results with more contemporary mortality data for physicians and nurses, as well as mortality data for numerous other fields of HCPs. There may be several reasons for lower mortality trends from cardiovascular and metabolic conditions among HCPs, particularly those with advanced degrees such as physicians, dentists, optometrists, physician assistants, and nurses. Health care practitioners may have higher levels of health literacy, better health habits, better access to care, and higher socioeconomic status, all of which may correlate with a lower risk of adverse cardiovascular outcomes. 13,14
However, HCPs including physicians may seek less preventative health care, 15 experience other barriers to health access, 16 and have unique workplace stressors 17 that may blunt some of the beneficial mortality effects experienced by HCPs. Additional focus on the health habits of both doctorate level HCPs and other HCPs is needed to better explain mortality trends among the key causes of death presented in this analysis.
Another important finding from the current analysis relates to mortality rates among HCPs stratified by race and gender. In the overall US population, all-cause mortality rates are higher for Black than for White individuals, and higher for men than for women. 18 In this analysis, trends in individual components of mortality among HCPs (vs. the overall gender- and race-matched population) appear similar between men and women and between Black and White individuals. Prior data on the effects of race and gender on mortality among HCPs are limited.
Among physicians who died between 1984 and 1995, age at the time of death was higher for White than for Black physicians. 3 In US men aged 16–60 years who died between 1982 and 1992, heart disease mortality was lower among White physicians and nurses than among other occupations. 19 However, mortality among Black physicians and nurses was similar to that among Black individuals in other occupations, and overall mortality was higher than among their White counterparts. 19
In this study, similar PMRs for Black and White HCPs and male and female HCPs suggest that differences in education and socioeconomic status associated with most health care fields may not lessen baseline gender and race-based health care disparities seen in the overall US population. 20 These results are consistent with literature demonstrating the attenuated benefit of higher socioeconomic and education level on health outcomes among Black men and women compared with White men and women in the United States, 21,22 which highlights the urgent need to address ongoing race and gender-based health inequalities including among HCPs.
Another important set of findings of this study relates to mortality from substance abuse and suicide. HCPs are less likely to experience mortality from substance abuse, including drugs and alcohol, compared with the general population. Although HCPs, including physicians and nurses, have rates of drug and alcohol abuse that mirror the general population, 23,24 they experience a better prognosis for recovery from chemical dependency 25 that may explain lower mortality rates from alcohol and drug abuse. In contrast, mortality by suicide is increased for most HCPs, with significantly higher rates among physicians, dentists, veterinarians, pharmacists, and physician assistants, as well as trends for increased rates for dental hygienists, registered nurses, and optometrists.
Higher rates of suicide have been reported for physicians, 6 nurses, 26,27 dentists, 28 and pharmacists, 29 with limited data on other health care workers. 6,30 Data on trends in suicide among HCPs over time are mixed. Physician suicide rates have remained stable over time in the United States, 6 whereas rates among HCPs and heath care support workers have exhibited variable trends. 30 Suicide among physicians, nurses, and other HCPs has been attributed to occupational stresses, difficulties attaining work–life balance, burnout, personality traits attributed to work in the health care setting, and concerns about seeking mental health services. 6,31,32
Higher rates of suicide among HCPs are more prominent in those aged 18–64 years, who are most at risk for such stressors. In contrast, higher socioeconomic status or relatively fewer work stressors among older and retired HCPs may contribute to the lower risk for suicide among HCPs over age 65 years. Among all HCPs evaluated in this analysis, Black and White HCPs and male and female HCPs exhibited similar increases in mortality by suicide compared with the overall gender- and race-matched population. This finding implies that suicide prevention interventions are similarly needed across all gender and race groups, even as women and racial minorities may benefit from targeted approaches that specifically address the needs of those populations. 33,34
Several additional findings of this study deserve further evaluation. Most types of HCPs, particularly those aged 18–64 years, are more likely to die from malignancies. There are limited data to explain this finding, as cancer screening by physicians has been reported to be similar to the general population, 35,36 and occupational exposures, such as medical radiation, have not consistently been associated with elevated cancer risk. 37,38 Additional research into malignancy screening rates and risk factors among HCPs is needed to further evaluate and potentially reduce malignancy-related mortality in this population.
Other findings of interest, such as higher diabetes-related mortality among dietitians and all HCPs, lower mortality among HCPs for heart disease but higher mortality for cerebrovascular disease, and lower mortality rates among physicians, dentists, pharmacists, and some other HCPs from infectious disease also deserve further evaluation. These results of the current study are also important as they highlight morbidity and mortality among a workforce that is experiencing a current shortage of physicians and other HCPs. This may be exacerbated by staffing shortages, burnout, and COVID-19–related mortality among HCPs. 39
This study has important limitations. The data are derived from death certificates maintained by a national data set and are reliant on accurate entry of etiology of mortality and accurate classification of an individual's specific occupation. 40 Based on data availability, only 26 states are included in the data set. Mortality for this article only extends through 2014, although these data are more contemporary than many other prior descriptions of mortality among HCPs. However, the data presented here cannot be used to determine the effects of the novel coronavirus pandemic that began in 2020 on HCP mortality.
The NOMS data set does not include important patient characteristics that may confound mortality analyses, such as comorbidities, lifestyle behaviors, and socioeconomic status. Therefore, individual HCPs within a specialty may have heterogeneous risk factor profiles that contribute to mortality and cannot be well evaluated in the NOMS data set. Specific etiologies of mortality need to be interpreted in the context of competing risks. For example, if HCPs are less likely to experience heart disease-associated mortality, they may eventually live longer to die of malignancy.
Similarly, HCPs prone to social stressors or with mental health comorbidities may succumb to suicide earlier in life thus making suicide as an etiology of mortality higher than the general population among younger HCPs; consequently, those HCPs who survive to older age may have lower suicide rates than other populations.
In conclusion, this study describes disease-specific mortality rates for various fields of HCPs in the United States. The results demonstrate that HCPs are more likely to die from suicide and less likely to die from other common causes including heart disease and alcohol/drug abuse. In addition, this study shows that trends for individual causes of mortality among HCPs are similar, based on gender and race. These results expand on limited literature on etiologies of mortality among HCPs and identify disease states that warrant further evaluation to improve outcomes in the growing field of HCPs.
Data Availability
The data are publicly available.
Footnotes
Authors' Contributions
Dr. Kobo contributed to conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing. Dr. Abramov was involved in writing—original draft, writing—review and editing, and validation. Drs. Volgman, Mieres, Wijeysundera, and Van Spall carried out writing—review and editing. Dr. Mamas was in charge of conceptualization, methodology, writing—review and editing, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11
Supplementary Table S12
Supplementary Table S13
Supplementary Table S14
Supplementary Table S15
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.