
Abstract

With the continued upward trend in the prevalence of diabetes and hypertension, chronic kidney disease (CKD) has become an increasingly serious population health issue that affects 37 million Americans. 1 By 2030, an estimated 1 in every 6 adults age 30 and over will have CKD, with greater prevalence among persons who identify as Black or Hispanic. 1 Medicare spends $124 billion per year on CKD and end-stage kidney disease (ESKD), 1 and $90,000 per patient/per year for those on hemodialysis. 2
In addition to potentially widening pre-existing health disparities, the pandemic has had a measurable impact on CKD. Coronavirus disease 2019 (COVID-19) is directly associated with acute kidney injury in hospitalized patients, and the question of long-term effects has yet to be resolved. Indirect effects of COVID-19 include delays in care for related chronic diseases (diabetes and hypertension), food insecurity, and potential widening of the existing digital divide 3 due to a shift toward telemedicine. 4
From a population perspective, there are two main challenges to providing care for CKD: Identifying those at risk for disease progression that will require dialysis or transplant. The current prediction tools to identify high-risk patients have not been widely adopted in routine clinical practice. We need a real-time CKD risk predictor that is integrated into the electronic health record (EHR) and facilitates easy identification of high-risk patients. Closing gaps in CKD care. Today there are >3000 patients with CKD for every nephrologist. Primary care physicians (PCPs) provide most of the care. We need more efficient systems-based resources for PCPs to manage these complex patients.
The patient-level challenges are substantial: 90% of those with CKD are unaware and, most often, awareness comes only when the disease is advanced (ie, causing symptoms) and dialysis is required in an unplanned way. 1 Studies consistently show the value of early identification, management and patient education for slowing disease progression, and preventing CKD-related complications. 5
Under Medicare's current fee-for-service model for kidney disease, the main clinician focus has been on ESKD, and there has been limited emphasis on optimizing CKD care to prevent progression to ESKD. 6 To limit costs and improve quality of care, the Centers for Medicare and Medicaid Services has launched new Kidney Care Choices 7 models with emphasis on shifting to value-based care, focusing upstream and intervening earlier in the trajectory of the disease. A number of value-based companies have developed programs for providers and patients to help improve kidney health 8 and address health equity.
By supporting providers in implementing the latest evidence-based guidelines these programs can help close the implementation gap for research to be fully translated into practice—a transition that usually takes 17 years. 9 Such programs can also help close gaps in health equity and access to specialized care, and can help shift the focus of ESKD care from hospital to home by preparing patients better for kidney transplant, in-home dialysis, or medical management without dialysis.
Researchers at the University of Pittsburgh are evaluating a model for value-based CKD care using a population health management (PHM) approach in the ongoing National Institutes of Health-funded randomized controlled trial (2018–2023)
Implementation of such clinical programs requires strong commitment from health system leadership and the willingness to make necessary investments of time and resources to build a robust EHR and clinical and data analytics infrastructure (Fig. 1).
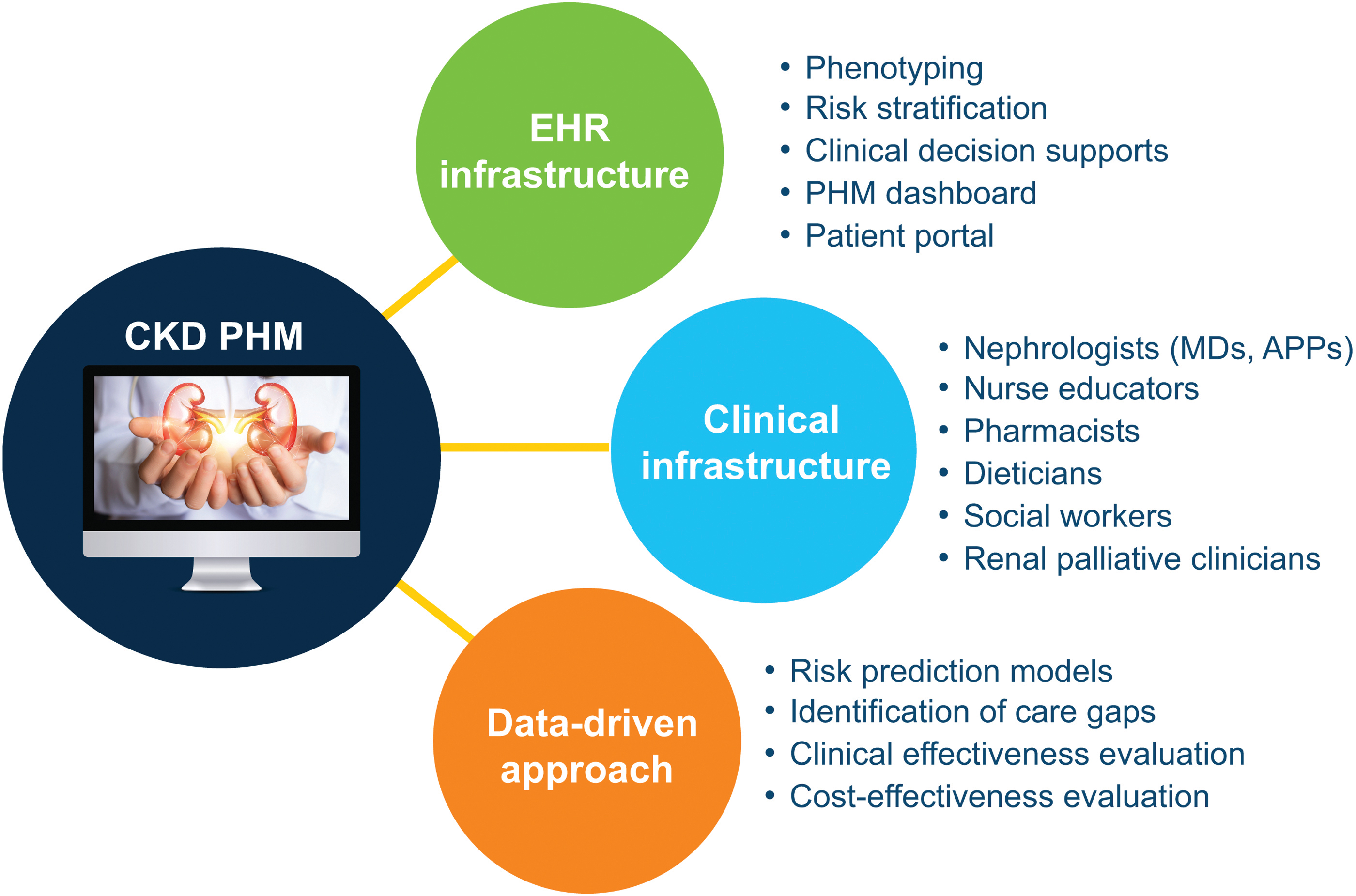
Health informatics, clinical and data analytic infrastructure.
This model is by no means a panacea. Gaps in care remain and solutions will require time, resources, and laser-like focus on improvement efforts. For example:
To facilitate comprehensive CKD care management, health systems must commit to investment in informatics and clinical infrastructure.
Resources are needed to identify and address social determinants of health to ensure equitable access to high-quality care.
Dissemination of standardized CKD care management guidelines are needed across all providers.
Traditional means for providing education to clinicians and patients are no longer effective. The digital age requires different approaches to patient and clinician education.
Footnotes
Author Disclosure Statement
Dr. Jhamb received no compensation for her contribution to this supplement. Her other potential conflicts of interest include grant support from Bayer, LLC and Pfizer; and advisory board participation with Boehringer Ingelheim, LLC.
Funding Information
Department of Medicine, University of Pittsburgh received funding to support Dr. Jhamb's NIH trial R01 DK116957.