
Abstract

Approximately 8.75
Individuals identifying as AI or AN have a life expectancy that is 5.5 years less than the general US population. 2 The chronic disease disparities behind this statistic are rooted in complex, intergenerational factors that range from historical trauma (eg, genocide, abuse, neglect associated with forced boarding school experiences) to traumatic childhood experiences (eg, abuse, witnessing violence in the home, food insecurity) and adult stressors (eg, alcoholism, poverty, racism). The pandemic magnified pre-existing inequities and disparities, thereby increasing the incidence and acuity of diseases. Overall, AI/AN populations experienced a 6.5% drop in life expectancy in just two years (2019–2021). 2
Chronic conditions pose a massive challenge for the AI/AN populations. Presence of heart disease is 30% more likely than in the non-AI/AN population and smoking rates are higher. Of particular concern, 40%–50% of children in AI/AN communities are reported as overweight or obese, 3 and 30% will have diabetes in their lifetimes. 4 With an incidence almost 3 times greater than the general population, population-based diabetes prevention and management is a primary goal for the tribes.
Native Americans use 1 of 3 models of health care delivery in agreements with the Indian Health Service. (1) The IHS may provide direct care to the tribe. (2) The tribe may enter into a Title I contract to administer its own health program in close consultation with IHS. (3) The tribe may opt for full self-governance by entering into a Title V Nation-to-Nation compact that allows for flexibility and self-governance to design and administer the tribe's health programs. Today, more than 60% of IHS appropriations are administered through these Title V compacts, and the MPTN health program operates under 1 of them.
The tribe supplements insufficient federal funding with its own resources to provide a self-funded, self-insured benefit for its community (tribal community, its employees, and their dependents). Funding is population based, and it is assumed that programs will be tailored to the user population.
MPTN's health program is a complete system, with a health care advisory board that affords its members a voice in governance. As a self-funded, self-insured payer, it receives and adjudicates its own medical and pharmacy claims through its own third-party administration service. The tribe manages the full spectrum of pharmacy services (in-house, online, specialty, and pharmacy benefit management). This allows the program to control, study, evaluate, and make appropriate adjustments based on needs and outcomes. Recent statistics show that, collectively, the health care expenditures for the tribes amount to less than $5,000 per person per year. This is significantly less than the $10,000 per person per year spent for the general population. 5
The highest hurdle for any health plan is member engagement and activation, and the MPTN health program uses human-centered design to promote buy-in from its member population. MPTN's Model of Health Sovereignty builds trust among the population through localized health care services, local control, and local knowledge that reflects community values (eg, honoring the natural world). Outreach and education materials are built around the tribe's own language and culture. Team-based, on-premises services include diabetes management programs; agriculture programs through which food from tribal farms is equitably distributed on a weekly or bi-weekly basis; and cultural channels that attune their narratives to the tribal level, thus increasing their relevance and helping to reduce health risks.
In response to the diabetes epidemic among AI/AN people, congress established the Special Diabetes Program for Indians in 1997. IHS and the Tribal Nations have shown improvement in diabetes care and outcomes. A comprehensive bundle of customized solutions focused on a patient-centric approach, integration of mental health, and on-site weight management have resulted in improved diabetes prevention rates, decreased incidence of diabetes, and—importantly—a decrease in diabetes-associated kidney failure (Fig. 1).
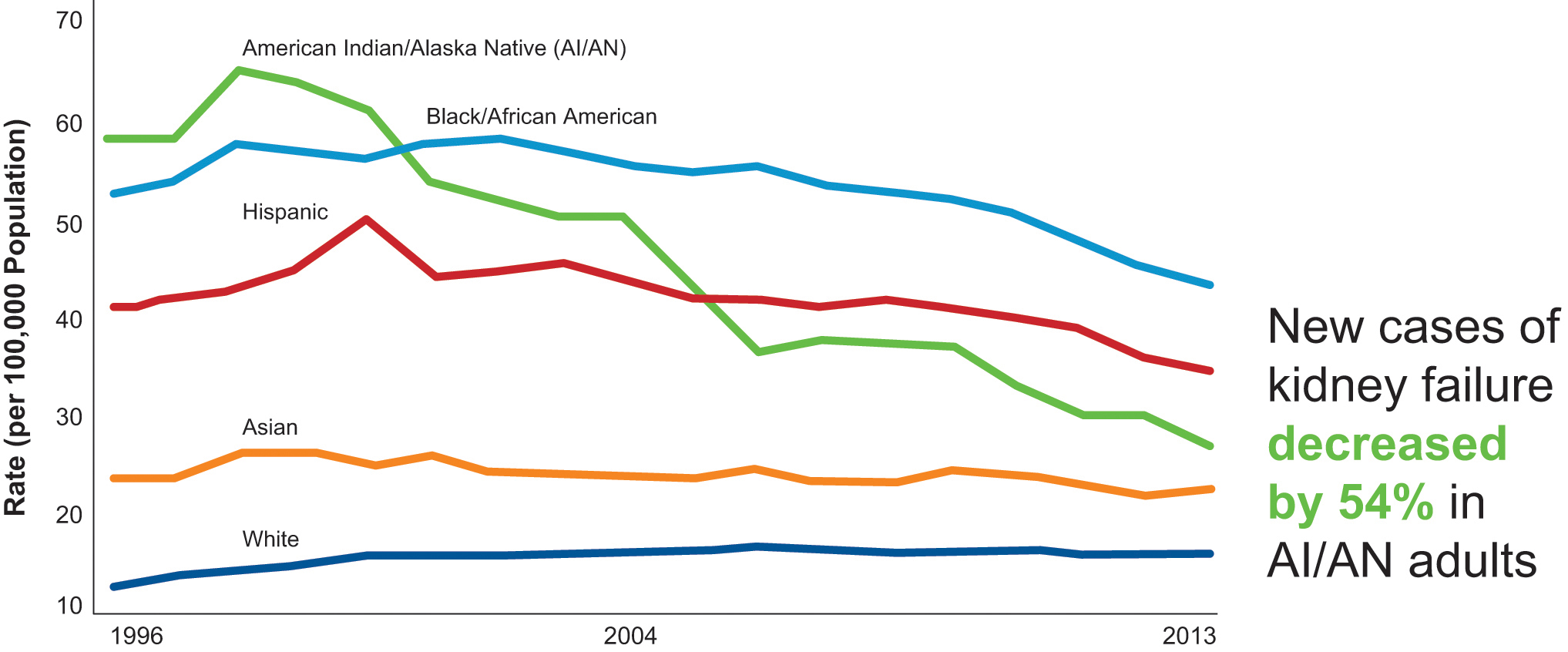
Decrease in diabetes-associated kidney failure. Source: Adapted from MMWR Morbid Mortal Wkly Rep. 2017;66:26–32. AI, American Indian; AN, Alaskan Native.
MPTN health utilizes digital health services in creative ways to assist people in its population living with type 2 diabetes.
Risk stratification/population health model: The Pequot Kidney Check app enables patients to do urinalysis testing on their phones. Even for patients who are not already engaged, this at-home test has been a plus. Of those screened to date, 40% had a positive result.
A free, in-house teleophthalmology solution that reduces barriers to appointments has helped improve retinal screening rates.
The Digital Virtual Metabolic Clinic provides metabolic disease management and health coaching services. Substantially improved health outcomes are shown in Figure 2. In terms of program expense, the pharmaceutical cost savings cover all program costs.
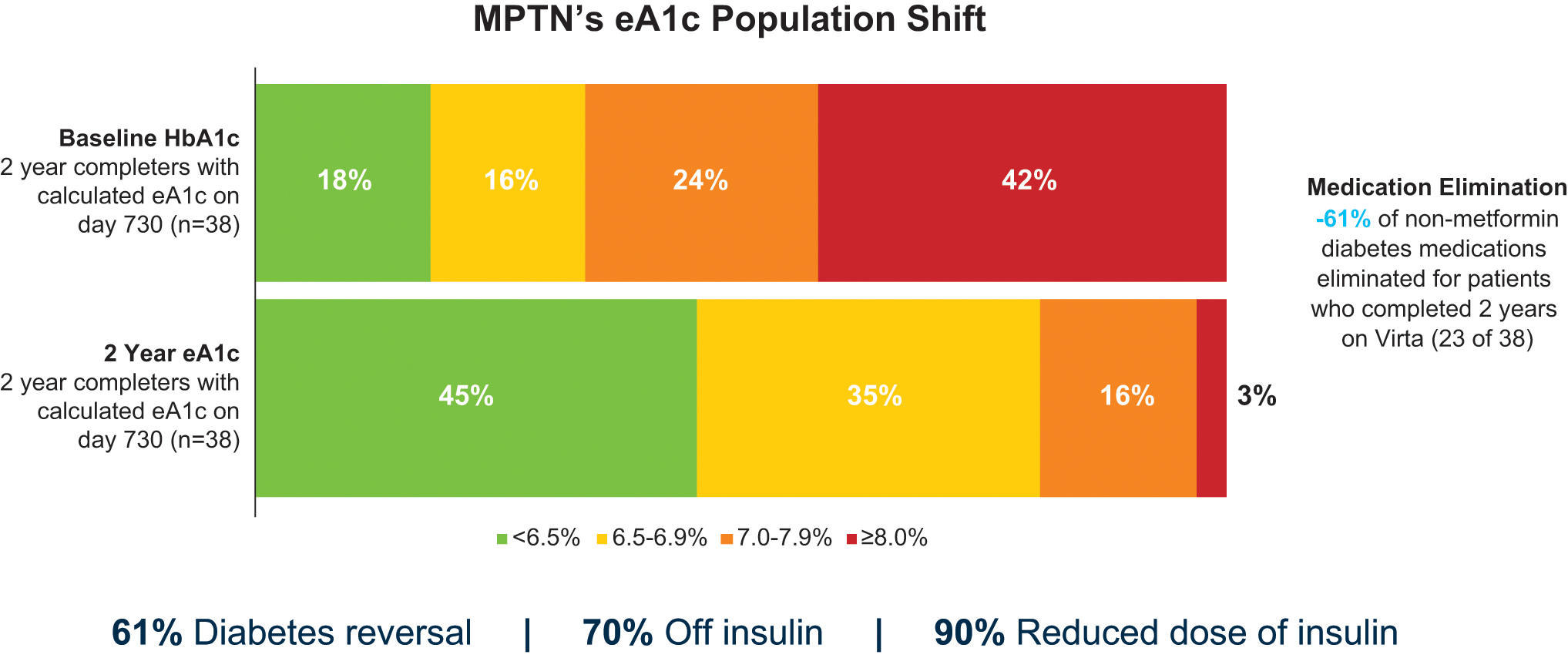
MPTN solution: digital virtual metabolic clinic. eA1c, estimated A1c; HbA1c, hemoglobin A1c; MPTN, Mashantucket Pequot Tribal Nation.
The Path Forward Postpandemic
Tribal elders were disproportionately affected by COVID-19 and efforts to minimize its impact on this population must continue as new variants arise. Although on-site COVID-19 tests were accessed by the already engaged population, testing may still be burdensome for some patients and providers. Tribes should consider onsite testing and multiplex PCR platforms to improve access and time-to-treatment and make that testing free for the members.
The pandemic has highlighted the need to build trust as a vital determinant of health. Social capital is built on trust with any organization, but more so with communities that have suffered. Trust does not come automatically—it must be earned and maintained over time. When the goal is to “manage” a patient's condition, it is helpful to have a “learner/listener” mindset. Communities are best served with an inclusive participatory model.
Footnotes
Author Disclosure Statement
Dr. Vora received no compensation for his contribution to this supplement and declared no other potential conflicts of interest.
Funding Information
No funding was received for this article.