
Abstract
The impacts of homelessness on health and health care access are detrimental. Intervention and efforts to improve outcomes and increase availability of affordable housing have mainly originated from the public health sector and government. The role that large community-based health systems may play has yet to be established. This study characterizes patients self-identified as homeless in acute care facilities in a large integrated health care system in Northern California to inform the development of collaborative interventions addressing unmet needs of this vulnerable population. The authors compared sociodemographic characteristics, clinical conditions, and health care utilization of individuals who did and did not self-identify as homeless and characterized their geographical distribution in relation to Sutter hospitals and homeless resources. Between July 1, 2019 and June 30, 2020, 5% (N = 20,259) of the acute care settings patients had evidence of homelessness, among which 51.1% age <45 years, 66.4% males, and 24% non-Hispanic Black. Patients experiencing homelessness had higher emergency department utilization and lower utilization of outpatient and urgent care services. Mental health conditions were more common among patients experiencing homelessness. More than half of the hospitals had >5% of patients who identified as homeless. Some hospitals with higher proportions of patients experiencing homelessness are not located near many shelter resources. By understanding patients who self-identify as homeless, it is possible to assess the role of the health system in addressing their unmet needs. Accurate identification is the first step for the health systems to develop and deliver better solutions through collaborations with nonprofit organizations, community partners, and government agencies.
Introduction
The number of people experiencing homelessness in the United States increased by 3% between 2019 and 2021. 1 The U.S. Department of Housing and Urban Development defines a person who is homeless as one who lacks a fixed, regular, and adequate nighttime residence. Approximately one third of individuals experiencing homelessness and 52% of people experiencing unsheltered homelessness in the United States live in the state of California. 1,2
Chronic housing shortages and decreased housing affordability (ie, increased housing costs for rent and property prices) are crucial factors contributing to the increases in homelessness. 3,4 Studies have shown that compared with people living in temporary housing arrangements, people experiencing unsheltered homelessness are more likely to remain homeless for longer periods, 2 and may be at higher risk of having significant physical, mental, and behavioral health challenges. 5
There is a plethora of literature and evidence demonstrating the detrimental impacts of homelessness on health 6 and health care access. 7,8 It is also well established that physical, mental, and behavioral health are directly impacted by homelessness through lack of sleep, excessive exposure to cold or heat, physical and sexual violence, social isolation, and difficulties accessing health care services. 6,9 People experiencing homelessness have increased health risks, 7,8 greater usage of emergency department (ED) and acute hospital services, 10 and premature death. 11
In addition, people experiencing homelessness are less likely to access primary and preventive care, which increase their risk for later-stage diagnosis and control of diseases such as diabetes and hypertension. 12,13 According to 2 studies by Montgomery et al and Rountree et al, women experiencing unsheltered homelessness are considered a particularly vulnerable population with increased risk of experiencing violent attacks. 14,15
Intervention and efforts to improve these outcomes and increase availability of affordable housing have mainly originated from the public health sector and government, and the optimal role that large community-based health systems may play has yet to be established.
California Senate Bill (SB) 1152 “Hospital patient discharge process: homeless patients” is a state-mandated local program that required, as of January 1, 2019, acute care hospitals and acute psychiatric hospitals to “establish a written process to make sure adequate post-hospital care arrangements are made for homeless patients; report patient housing and discharge information to the Office of Statewide Health Planning and Development; coordinate services and referrals with behavioral health, medical care, and social services agencies for homeless patients; and maintain an accurate list of local homeless shelters, including their operation hours and admission procedures.” 16
Given this mandate, health systems in California are now compelled to collect comprehensive data regarding housing status through electronic health records (EHRs) for all acute care hospital patients and facilities. This legislation presents a unique opportunity not only for health systems to better identify the unmet needs of this population, but also to illuminate innovative solutions within which health systems may play a central role.
The purpose of this study is to characterize patients who self-identified as homeless among acute care patients in a large integrated health care system in Northern California. This group of patients was compared with those who did not identify as homeless with respect to sociodemographic characteristics, clinical conditions, and health care utilization. Finally, the team characterized the geographical distribution of patients experiencing homelessness in relation to Sutter hospitals and homeless resources.
Methods
Study setting and data source
This study was conducted at Sutter Health, a large not-for-profit integrated health system in northern California. Sutter delivers comprehensive medical services in >100 ambulatory clinics and 24 acute care hospitals, caring for ∼3.5 million people each year across 22 counties in California, in both urban and rural settings. Ten of those counties are in the San Francisco Bay Area, a highly populated and racially diverse region. Sutter's EHR (Epic Systems Corporation) is fully integrated across all hospital and ambulatory sites. This study was approved by Sutter's Institutional Review Board and was conducted according to Health Insurance Portability and Accountability Act standards.
Cohort identification and variable definitions
Data for this study were extracted from the Sutter EHR for the period July 1, 2019–June 30, 2020. Adult patients (18+) were identified based on first evidence of homelessness (index date) (group 1); comparators were selected based on first hospital or ED encounter (index date) within the study period (group 2).
Self-identified homelessness status was determined by the presence of any of the following criteria (Appendix Table A1): (1) patients' address is documented as “homeless,” (2) zip code indicates homelessness, (3) patient encounter has a check box indicating if homeless, (4) evidence of a Homeless Discharge Flowsheet (ie, written plan for homeless patient mandated by SB 1152), (5) discharge diagnosis documented as “Problems related to housing and economic circumstances” (ie, International Classification of Diseases-10 Z59*), or (6) patient housing status in patient demographic table.
Demographic and clinical characteristics were extracted from the EHR for all patients included in the study, including date of birth, sex, self-reported race/ethnicity, payer at index date, and frequent ED utilizer status (≥4 visits in 12 months). Health care utilization and clinical characteristics were calculated for the 12 months before index date (Tables 1 –5). Age was calculated as of the index date and classified as 18–29, 30–44, 45–64, 65–79, and 80 years and over.
Patient Demographic Characteristics
NHA, non-Hispanic Asian; NHB, non-Hispanic Black; NHO, non-Hispanic other; NHW, non-Hispanic White.
Patients Health Care Utilization and Clinical Characteristics
Includes data from Sutter hospitals and Care Everywhere.
Includes data from only Sutter hospitals.
ADHD, Attention-deficit/hyperactivity disorder; CHF, congestive heart failure; Dx, diagnosis; ED, emergency department; HIV = human immunodeficiency virus; IP, inpatient; OP, outpatient; SMI, serious mental illness.
Clinical Covariate Definitions
Dx, diagnosis; HIV, human immunodeficiency virus; ICD, International Classification of Diseases.
Serious Mental Illness Diagnoses
ICD, International Classification of Diseases.
Other Variable Electronic Health Records Definitions
Includes data from Sutter hospitals and Care Everywhere.
Includes data from only Sutter hospitals.
AA, African American; ED, emergency department; ICD, International Classification of Diseases; IP, inpatient; NHA, non-Hispanic Asian; NHB, non-Hispanic Black; NHO, non-Hispanic other; NHW, non-Hispanic White; Ob/gyn, obstetrician-gynecologist; OP, outpatient; SMI, serious mental illness.
Smoking status was classified as of most recent self-reported information available during 12 months before the index date (current, former, never, or unknown). Race/ethnicity was defined first by ethnic origin, followed by racial identity. Patients who self-identified as Hispanic were classified as such regardless of race. Patients who self-identified as non-Hispanic or whose ethnic origin was unknown, were classified by race (ie, non-Hispanic White [NHW], non-Hispanic Black [NHB], non-Hispanic Asian [NHA], non-Hispanic other [NHO]).
Geospatial analysis
Addresses of all Sutter hospitals and homeless shelters
17
in Northern California were obtained and R Statistical Software version 4.1.2 (R Core Team [2018]
Statistical analysis
Sociodemographic and clinical characteristics of patients in groups 1 and 2 were summarized using descriptive statistics. Standard univariate tests (eg, chi-square tests) were used for comparing the groups homeless, and not homeless (comparison group). Data extraction and statistical analyses were performed in SQL server management studio 18.7.1, and SAS Enterprise Guide 7.1 (Cary, NC). As the study was descriptive in nature, and all available data were included, no sample size calculations were conducted, and no hypotheses were tested.
Results
Demographics
The team identified 20,259 patients who had evidence of homelessness between July 1, 2019 and June 30, 2020, representing ∼5% of the total patients (N = 433,212) seen across acute care settings during that period. More than half (51.1%, N = 10,367) of patients experiencing homelessness were aged <45 years compared with 46.5% (N = 191,932) of patients without homelessness (P < 0.001). Males accounted for 66.4% (N = 13,448) of patients with homelessness compared with 41.8% (N = 172,732) of patients without homelessness (P < 0.001; Table 1). The 2 groups of patients differed by race/ethnicity.
A larger percentage of patients experiencing homelessness were NHB (24% [N = 4940] vs. 11.3% [N = 46,827]), and a smaller percentage of patient experiencing homelessness were Hispanic (15.8% [N = 3204] vs. 23.1% [N = 95,471]), or NHA (2.2% [N = 449] vs. 9.6% [N = 39,782]; P < 0.00001 for all). In terms of payer coverage, 60.7% (N = 12,295) of patients experiencing homelessness and 29.1% (N = 120,011) of patients not experiencing homelessness were insured by Medicaid, and 28.5% (N = 117,781) of patients not experiencing homelessness and 16.2% (N = 3281) of patients experiencing homelessness were insured by Medicare (P < 0.0001).
Clinical characteristics
Compared with patients not experiencing homelessness, human immunodeficiency virus (1.9% [N = 392] vs. 0.5% [N = 2044]), and mild liver disease (6.6% [N = 1343] vs. 4.1% [N = 17,105]) were more common among patients experiencing homelessness (Table 2). In contrast, hypertension (17.6% [N = 3557] vs. 26.8% [N = 110,647]), chronic pulmonary disease (12.8% [N = 2600] vs. 14.0% [57,657]), and type 2 diabetes (8.1% [N = 1633] vs. 12.1% [N = 49,889]) were less commonly occurring conditions among patients experiencing homelessness as compared with patients not experiencing homelessness.
Mental health
All mental health conditions were more common among patients experiencing homelessness: the largest discrepancies were for alcohol use disorder (11.1% [N = 2253] vs. 2.5% [10,332]); schizophrenia (8.3% [N = 1690] vs. 0.7% [N = 2923]); and suicide-related behavior (7.9% [N = 1604] vs. 0.9% [N = 3729]) (Table 2). More than one third (34.2% [N = 6934] of patients experiencing homelessness had at least 1 serious mental illness (SMI) (Tables 2 and 5) compared with one fifth (19.9% [N = 82,163]) of patients not experiencing homelessness.
Utilization
Approximately 1 quarter (24.4%, N = 4951) of patients experiencing homelessness were classified as frequent ED utilizers compared with 4.2% (N = 17,296) of patients not experiencing homelessness. One tenth (10.0% (N = 2025)) of patients experiencing homelessness had at least 1 hospital outpatient (OP), urgent care, or office visit encounter compared with 41.5% (N = 171,533) of patients not experiencing homelessness. In contrast, 11.7% (N = 2369) of patients experiencing homelessness had at least 1 inpatient (IP) hospitalization during 12 months before index date compared with 6.5% (N = 26,972) of patients not experiencing homelessness.
Geospatial analysis
Geospatial analysis revealed the areas with high density of homeless shelters (ie, within 3 km of a Sutter hospital; Figure 1A) and proportion of patients experiencing homelessness (Figure 1B) for a given hospital by hospital size (ie, number of patients served at a given hospital) (Table 6). Although there is a high density of resources in the San Francisco area, some hospitals within the system with higher proportions of patients experiencing homelessness are in geographies with very few shelter resources (eg, in Antioch and Tracy) (Table 6). In addition, more than half of the hospitals in the health systems had >5% of patients who have identified as homeless.
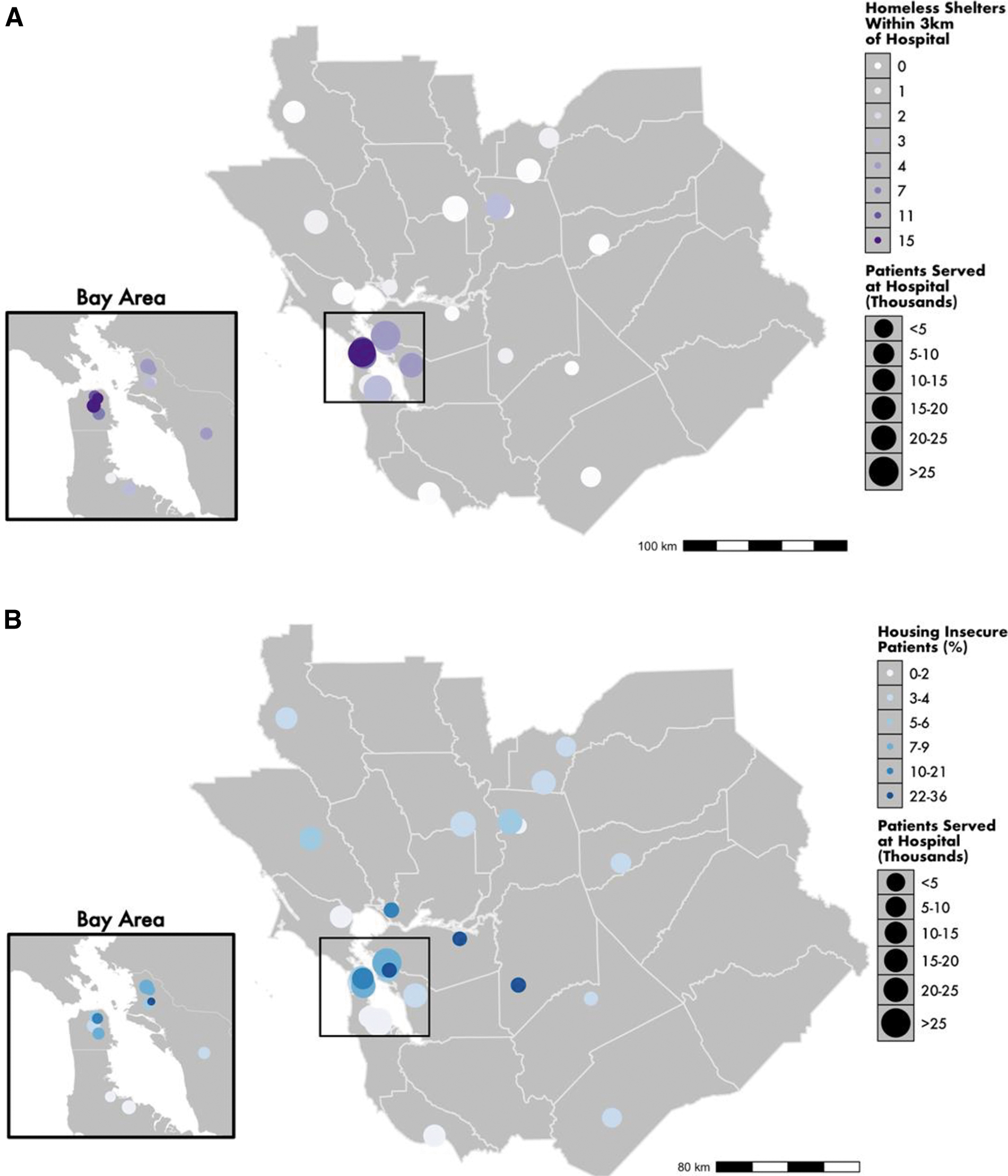
Geographic distribution of patient self-identifying as homeless.
Number of Homeless Shelters and Patients Seen in Each City
Discussion
The team sought to compare differences in sociodemographic characteristics, clinical conditions, and health care utilization among patients who self-identified as homeless compared with those who did not report homelessness, within a large integrated health care system in northern California. Leveraging recent statewide legislation, they aim to identify the unmet needs of this population and identify available existing resources to inform innovative solutions within which health systems may play a central role.
Accurately and consistently identifying individuals experiencing homelessness is the first step for health systems to develop and deliver innovative and effective solutions, through collaborative partnerships with nonprofit organizations and community partners, government, and Federally Qualified Health Centers (FQHCs). Although SB 115216 represents a step forward, there continues to be a lack of statewide or national standards for documenting homeless status within EHR, hindering population health and public health strategies to improve outcomes for this vulnerable population.
The cohort of individuals with homelessness who utilized Sutter hospitals tended to be younger, although nearly half were aged >45 years. This group also had a higher proportion of males and individuals self-identifying as NHB, compared with those with housing. Individuals with homelessness experienced a higher prevalence of substance use, including drugs and alcohol, and SMI, as has been identified in other studies. 18,19 In terms of utilization of health care services, those who reported being homeless had more frequent ED utilization and less utilization of OP and urgent care services.
These findings are consistent with national reports, where the majority of people experiencing homelessness were adults, majority male (61%), and approximately half were NHW (48%). 1 As these and other researchers have found, homelessness disproportionately affects individuals who self-identify as Black race/ethnicity, where 24% of those in this study with homelessness were NHB compared with 6% of the total patient population.
The U.S. Department of Housing and Urban Development noted in its 2019 annual report that in the 50 most populous cities in the United States, Black individuals make up the majority of the homeless population, 20 and accounted for 40% of all people experiencing homelessness in 2019. 20 Decades of discrimination and systemic racism, including Jim Crow segregation laws, 21 redlining, 22 and historical unequal access to lending, 23 have contributed to the crisis resulting in disproportionately lower home ownership for Black Americans compared with White Americans (46.4% vs. 75.8%, respectively). 23,24 All of these are significant contributing factors to the racial wealth gap. 23
As these efforts continue, it is crucial to understand that different subpopulations of individuals with homelessness may require different interventions, and this could begin at the point of care. More precisely targeted pathways can help to allocate scarce resources to those groups at highest risk or in most need. Individuals who are older will likely also have more complex health needs that require care coordination and case management. A study conducted by Lewer et al (2019) showed that people experiencing homelessness are 3 times more likely to have chronic diseases such as heart problems with asthma, chronic obstructive pulmonary disease, and epilepsy, as compared with their not homeless counterparts. 25
The team found that those with homelessness tended to have lower utilization of OP services—less diagnostic and preventative screening access/utilization, which likely contribute to the challenge of chronic disease management. This is also likely the reason this study showed lower prevalence of hypertension, pulmonary disease, and diabetes—all disorders typically diagnosed in primary care settings. Moreover, people experiencing homelessness have a higher prevalence of a range of infectious diseases in part related to lack of hygiene, access to sanitary products, 26 and substance use disorders. 6
In addition, persistent homelessness has been associated with twice the odds of violent victimization among older adults with homelessness, 27 necessitating a proactive approach to ensuring mental health and counseling resources for patients in these circumstances. Aligned with this study's findings, reviews of risk factors for homelessness have shown that mental illness and substance use disorders are strongly associated with homelessness. 18,19 Significant mental health disorders are present in 30%–50% of people experiencing homelessness, including functional psychoses, acute distress, and personality dysfunction. 28
Comorbidity of mental illness and substance misuse occurs in 20% of people experiencing homelessness, 28 and the prevalence of alcohol and drug dependence, including heroin and other opioids, is high in the homeless population. 29,30 Moreover, drug overdose was proven to be the leading cause of death among people experiencing homelessness, with other causes of death related to substance use. 31,32 These findings are not new, highlighting the persistent inadequacy of mental health and substance misuse treatment access, especially for those with the highest need.
The US Interagency Council on Homelessness reports that >150,000 individuals in California were homeless on any given day in 2019. 1 Many of them had at least 1 encounter with Sutter Health. In this study, ∼25% of patients with homelessness were identified as frequent ED utilizers, indicating that they had multiple touchpoints with the ED.
Although health care systems cannot solve homelessness in isolation, they can serve as a point of entry to housing-first initiatives and other public health resources for homelessness remediation and action. Although “Housing First” 33 has been the preferred intervention to address the complex psychosocial and medical needs associated with homelessness, critical shortages of affordable housing in urban and suburban areas necessitates innovative solutions to bridge people from more immediate to long-term interventions.
Even in the absence of significant changes to the system, there remain many opportunities for innovative and more effective care models within acute care settings. Social emergency medicine is an innovative and increasingly popular approach, focusing on the interplay between medical issues and social drivers of health, and how they manifest in emergency care settings, 34 necessitating the integration of social and chronic disease management services within ED settings. Multidisciplinary ED-based social medicine teams can support ED clinicians and patients by helping to meet the complex medical, behavioral, and social needs of patients with homelessness. 35
The team typically includes a patient navigator, hospital-based social workers, care coordination nurses, a pharmacist, physician consultants, and specialists in transitional care, substance use, and quality improvement. 35 In addition, the model depends on strong partnerships with ambulatory health care clinicians and community-based organizations essential to the safe discharge and successful care of ED patients with complex social needs when they return to the community. 35
Federal programs aimed at improving primary care access and that are reimbursable by the Center for Medicaid and Medicare (CMS), such as the Emergency Triage, Treat, and Transport program, 36 have great potential to expand access to ambulatory health care services among medically underserved by partnering with regional FQHCs to establish or reestablish the medical home, allowing beneficiaries to access the most appropriate emergency services at the right time and place.
The program was developed to triage persons who are high utilizers of nonurgent care in area EDs and IP settings to ensure that they do not have urgent health care needs, transport them to an appropriate health center location, and treat them in a place where they can establish routine health care.
In addition to actions taken within care settings, health systems can and must partner with public health agencies and community-based groups to design and implement targeted innovative interventions to address structural causes of homelessness. The underlying causes of homelessness are a complex interaction between individual and structural factors. 6 Individual factors, which include poverty, adverse childhood experiences, mental health and substance misuse problems among others, 37 –39 are compounded by a lack of affordable housing, employment opportunities for low-skilled workers, and income support. 6
Integration of the acute care safety net with local, regional, and state-funded social services to facilitate real-time referral and access to wrap around services, including OP mental health treatment and treatment for substance use disorders, is crucial. Examples include state-funded efforts such as Whole Person Care (WPC) 40 —with patients flowing from the hospital, to respite and finally, into WPC to receive long-term case management services and permanent housing. The WPC program supports individuals with the highest service needs through coordinated delivery of physical health, behavioral health, housing support, food stability, and other critical services.
In addition, the Department of Health Care Services (DHCS) and Medi-Cal system's new California Advancing and Innovating Medi-Cal program aims to offer Medi-Cal enrollees coordinated and equitable access to services that address their physical, behavioral, developmental, dental, and long-term care needs, throughout their lives. 41 All too often these promising services are unavailable or difficult to access.
To facilitate such integration would require a reimagining of access, where once identified in the acute care setting, patients could be actively connected to appropriate social services 24/7 without delay, or at least during evening shifts in contrast to traditional business hours (ie, 9 am–5 pm). In this way, health care systems and care teams can serve as important links to ensure navigation support for external resources that otherwise would be inaccessible to individuals with the highest need.
Limitations and strengths
This study has several limitations. First, it is based on a single health care system; however, the system does serve a large diverse region and is representative of many aspects of the US population. Second, the severity of comorbid conditions was not considered for identifying clinical characteristics and relied exclusively on diagnosis codes. In this manner, patients with severe and mild disease were classified together.
The authors recognize that the state of being “homeless” is fluid and not static, where individuals may at different timepoints be housed or unhoused, given the episodic nature of the EHR identification method, their analysis does not account for changes in homelessness status, and is limited to assessment and identification of individuals who identify as homeless at 1 timepoint. In addition, although the SB 1152 requires that individuals who are experiencing homelessness are identified and documented, there is still no standard for identification and assessment method and no requirement for using a standardized validated questionnaire.
This will likely result in an underestimation of individuals experiencing homelessness. Finally, because Sutter Health is an open system in which patients can receive care from other providers outside the system, some information may be missing. To ameliorate this problem, the team supplemented their Sutter EHR data with data from Care Everywhere, which allows them to access information from other EPIC systems to identify diagnosis information.
Strengths of this study include Sutter's integrated system-wide EHR that allowed the team to analyze data across their network of clinics and hospitals, and the accessible patient population that is representative of the state of California according to underlying racial/ethnic distributions. In addition, the program to collect race and ethnicity data has been in place for more than a decade, and it provides a near-complete source of self-reported information.
Conclusion
Health care systems have an opportunity and an obligation to leverage numerous touchpoints with patients experiencing homelessness to intervene at the point of care and play a more active role in addressing the complex unmet psychosocial and medical needs of those experiencing homelessness. Improvements and real-time integration of the acute care safety net health care services with local, regional, and state-funded social services would ensure that the intention of SB-1152 is not only met but also goes further to catalyze systems change.
As patient subgroup becomes better understood, health care providers can move toward fulfilling the greater goal of identifying the role of the health system in addressing the unmet medical and social care needs of these patients.
Footnotes
Acknowledgment
The authors thank Ivelina Popova for her assistance with the submission of this article and for her overall support.
Authors' Contributions
The authors would also like to thank Dr. Margot Kushel for providing guidance and reviewing the manuscript. Methodology (lead) and writing, reviewing/editing (equal) by S.M. Reviewing/editing (equal) by C.N. and S.B. Methodology and reviewing/editing (equal) by A.P. Conceptualization and reviewing/editing (equal) by A.K., J.C.L., and J.P. Conceptualization, methodology, writing (lead), and reviewing/editing (equal) by K.M.J.A.
Author Disclosure Statement
S.M. and K.M.J.A. report that the study was funded by Janssen Scientific Affairs, LLC. J.C.L. and J.P. are employees of Jansen and J&J stockholders. No other competing, personal financial, funding, employment, or other interests are reported by the authors.
Funding Information
The study was funded by Janssen Scientific Affairs, LLC.
Appendix
Criteria to Identify Homelessness Status
| Patient address | Encounter check | Discharge flowsheet | Z59.x discharge diagnosis | Patient type homeless | Patients |
|---|---|---|---|---|---|
| X | X | X | X | 5882 (29.0%) | |
| X | 3093 (15.3%) | ||||
| X | 2770 (13.7%) | ||||
| X | 1859 (9.2%) | ||||
| X | X | 1703 (8.4%) | |||
| X | X | X | 1116 (5.5%) | ||
| X | X | X | 1088 (5.4%) | ||
| X | X | X | 665 (3.3%) | ||
| X | X | 581 (2.9%) | |||
| X | X | 484 (2.4%) | |||
| X | 382 (1.9%) | ||||
| X | 244 (1.2%) | ||||
| X | X | 160 (0.8%) | |||
| X | X | 114 (0.6%) | |||
| X | X | X | 70 (0.3%) | ||
| X | X | 48 (0.2%) |