
Abstract
This study aimed at examining the effect of continued use of home health care resources on end-of-life care at home in older patients with cancer. This retrospective cohort study was conducted using medical and long-term care claims data of 6435 older patients with cancer who died between April 2016 and March 2019 in Fukuoka Prefecture. The main explanatory variables were enhanced home care support clinics and hospitals (HCSCs), enhanced HCSCs with beds, conventional HCSCs, other HCSCs, and home visit nursing care. The covariates were sex, age, required level of care, and the Charlson Comorbidity Index. A logistic regression model was used. The results of the multilevel logistic regression analysis showed that the following were significantly associated with end-of-life care at home: use of enhanced HCSCs with beds (odds ratio, OR: 8.66; 95% confidence interval, CI: [4.31–17.40]), conventional HCSCs (OR: 5.78; 95% CI: [1.86–17.94]), enhanced HCSCs (OR: 4.44; 95% CI: [1.47–13.42]), home-visit nursing care (OR: 1.86; 95% CI: [1.42–2.44]), and a severe need for care (OR: 3.89; 95% CI: [2.92–5.18]). The results suggest that the continued use of home health care resources in older patients with cancer who require out-of-hospital care may lead to increased end-of-life care at home. Particularly, use of enhanced HCSCs with beds is most strongly associated with end-of-life care at home.
Introduction
With the aging population, the demand for improving the quality of end-of-life care is expanding. In particular, there is significant focus on the desired place of death of patients with diseases without a prospect of recovery, such as terminal cancer. 1 –3 Over the past few decades, hospitals have been the most common place of death, instead of home, in developed countries, including Japan, 2,4 while many patients with cancer wish to die at home. 3,5 –8
Home-based palliative care is expected to improve quality of life (QOL) and reduce the physical and emotional burden on patients. 7 –9 In addition, it has been highlighted that the use of home care by patients who wish to die at home can lead to shorter hospital stays, prevent readmission, and improve the quality of palliative care 10,11 by optimizing the allocation of medical resources and financial burden.
A main barrier to death at home is the lack of palliative care services due to inadequate development of home health care delivery system. 3,12,13 For example, Wye et al suggested that specialized 24-hour integrated palliative care services increase family carer satisfaction and more deaths in the community. 14
Therefore, to improve the quality of end-of-life care, Japan is promoting the development of a system for the provision of home health care by enhancing reimbursement for institutions such as home care, 24-hour home care support clinics and hospitals (HCSCs), and home-visit nursing care services. 15 –17 One such application is home health care services that is covered by Japan's Universal Health Insurance system.
As of 2023, the home health care services, which are mainly used by patients who are terminally ill such as those with cancer, are divided into 4 types depending on the medical institution providing service to them: enhanced HCSCs with or without bed, conventional HCSCs, and other HCSCs. 18 Patients can freely choose from these services according to their preferences.
In particular, conventional HCSCs play a central role in home health care by attending to emergency house calls and providing 24-hour home-visit nursing care and end-of-life care at home. In 2012, the enhanced HCSC category was introduced to the existing HCSC requirements, adding 3 or more full-time doctors and ensuring a certain level of experience in attending to emergency house calls and providing end-of-life care, to provide a wider range of services. 17,18 The current reimbursement system provides the greatest incentive for home health services to enhanced HCSCs by which they have beds or not. 17,18
Another health care service that complements home health care services is home-visit nursing care, which is covered by both medical and long-term care (LTC) insurance. 19 Some home-visit nursing care under the HCSC is provided on a 24-hour basis, whereas others are implemented flexibly according to the instructions of the family doctor and the form of the visiting nursing agency.
However, a few empirical studies have examined how the home health care provision system that has been promoted in Japan since 2013 and includes home-visit nursing care affects the end-of-life care at home in patients with cancer. Recent studies have shown that the use of enhanced HCSCs (with or without beds) and conventional HCSCs increases the rate of death at home 20,21 ; however, they do not focus on home-visit nursing care services separately from home health care services. Moreover, the effects of continuing services have not been measured.
Therefore, this study aimed at assessing the impact on end-of-life care at home of older patients with cancer in Japan, with a focus on the continued use of home health care services and home-visit nursing care.
Methods
Database
The medical and LTC insurance databases from April 1, 2016 to March 31, 2019, were obtained from the Fukuoka Prefecture Association of Latter-Stage Elderly Healthcare, Japan's public insurance system for individuals aged 75 years and older and those aged 65–74 with specified illnesses. Medical claims information includes patient characteristics such as age, sex, admission and discharge status, disease diagnosis, medical treatment practices, and drug prescriptions for those who have received insurance treatment.
LTC is the public insurance for older people aged 65 years and older and adults aged 40 years and older with specified illnesses. This care fee claim contains monthly information on age, sex, required level of care, and service use for all people certified to use care insurance. 22 LTC insurance classifies the required level of care into 7 levels. The 2 lowest levels are classified as “support required” (levels 1 and 2), for users who often live independently and require little or no care services.
The other 5 levels are classified as “care required” (levels 1, 2, 3, 4, and 5), with higher levels indicating greater care dependency. 22 Administrative claims data were integrated by reconstructing the database to ensure that individuals were not identified using workstations that were not connected to the network.
Study design
This study had a retrospective cohort design. It analyzed the data for patients with cancer who died between April 1, 2016 and March 31, 2019. Cancer diagnosis was classified according to the International Classification of Diseases, tenth revision (ICD-10) codes (C00-C96). Apart from the diagnosis, patients with cancer were categorized using the medical practices.
Surgical treatments were categorized using surgical codes, chemotherapy and radiotherapy using drug codes, and place of death as home death and other deaths based on billing code records of end-of-life care in medical and LTC claims. The term “home” in this study referred to a home for older adults from the perspective of living a convalescent life in a familiar environment with a consideration for QOL, even if medical needs were high, and included serviced housing for older adults, small-scale multifunctional nursing homes, fee-paying nursing homes, and group homes for older individuals with dementia.
Figure 1 shows the participant selection process flow diagram. Supplementary Appendix S1 shows the codes used to identify medical treatments and end-of-life care.
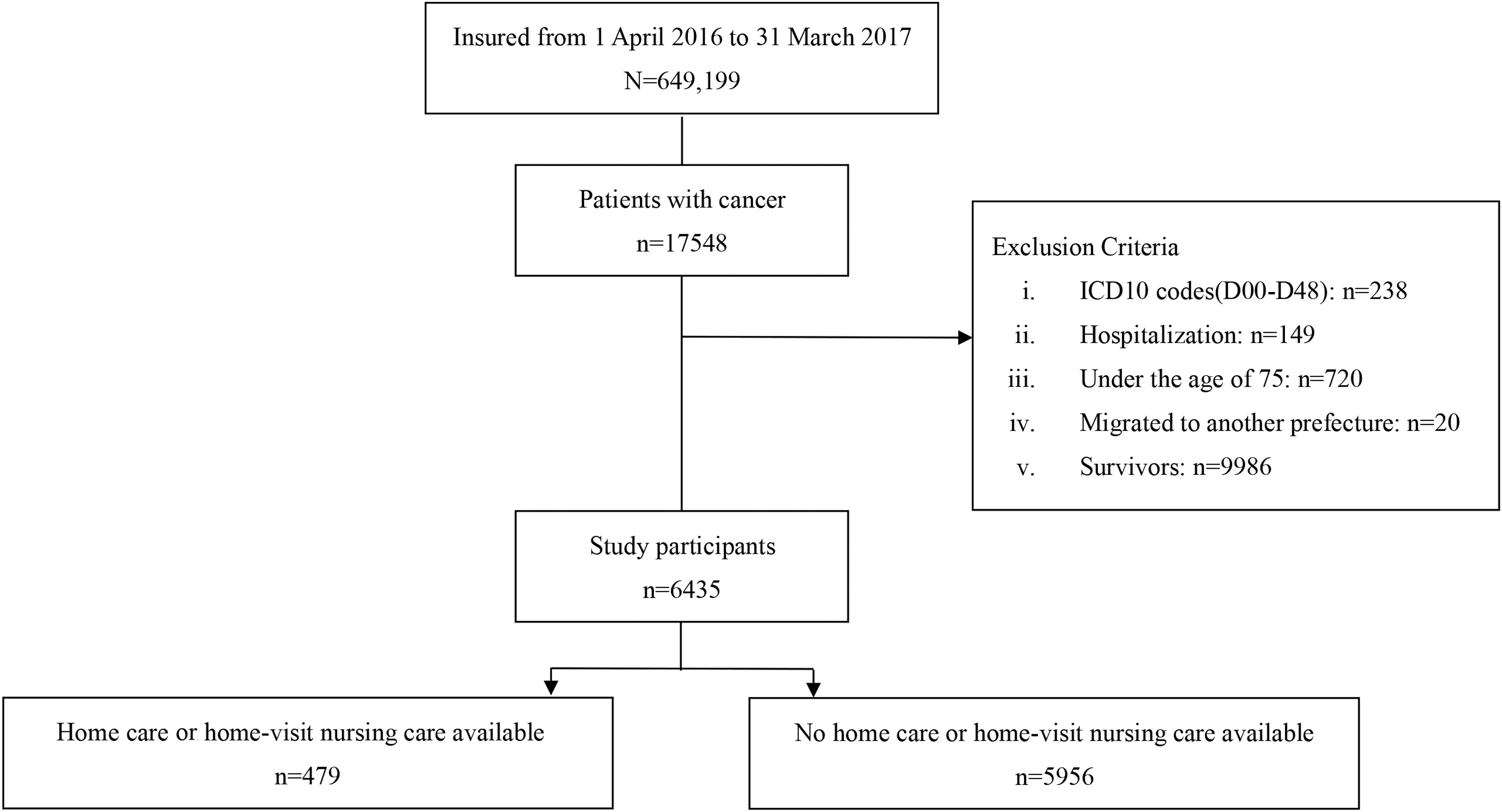
Flowchart of study participant selection.
To evaluate the outcomes of end-of-life care at home, the main explanatory variables were the use or non-use of home health care services and home-visit nursing care. Types of home health care services by medical claims were enhanced HCSCs without beds, enhanced HCSCs with beds, conventional HCSCs mixed with beds and without beds, and other HCSCs such as general clinics.
Therefore, there were 4 main explanatory variables: enhanced HCSCs, enhanced HCSCs with beds, conventional HCSCs, and other HCSCs. Details regarding the definitions for the HCSC explanatory variables are described in Figure 2. Enhanced HCSCs, enhanced HCSCs with beds, conventional HCSCs, and other HCSCs were considered if a patient was diagnosed with cancer between April 1, 2016 and March 31, 2017, used the service at least once a month, and received treatment for at least 3 months.

Definitions of home care support clinics and hospitals explanatory variables. A refers to the availability of beds in the facility, B refers to the number of full-time physicians and the operating condition, C refers to the home health care system, D refers to functions of cooperation, and E refers to the level of the facility's needs. *To promote the home health care service system. The arrow indicates the direction of time flow. HCSCs, home care support clinics/hospitals. Note: Quoted and altered from Presentation Materials of Overview of the Revision of Medical Fees Home (Home health care, home nursing) (in Japanese) 2022. Japanese Ministry of Health, Labour and Welfare (online). Available at
The reason for this definition was to exclude those who only used the service immediately before death, as patients with cancer require extensive care and treatment from ∼1 month before death. 23 The definition of home-visit nursing care was identified from the visit nursing instructions of the medical claims and home care nursing service codes of the LTC claims.
Note that home nursing covered by health insurance is usually ordered once a month by the primary care physician but is valid for up to 6 months. It is, therefore, possible that some patients may not be billed every month depending on the doctor's decision. To ensure continuity, home nursing for medical insurance includes patients who have had a home nursing order for at least 2 months.
Residents who migrated to other prefectures were excluded from the tracking period. Supplementary Appendix S2 contains the codes used to identify exposure. Supplementary Appendix S3 shows the details of the types of home health care facilities.
Sex, age, care, and Charlson comorbidity index (CCI) scores were used as covariates. Age was divided into 4 categories: 75–79, 80–84, 85–89, and ≥90 years. CCI scores showing the weighted number of individuals with co-existing disorders were calculated and divided into 3 categories: 0–3, 4–5, and ≥6. 24
Statistical analysis
Patients who used enhanced HCSC, enhanced HCSC with beds, conventional HCSC, other HCSC, or home nursing were defined as the home-care group and others as the non-home care group; the data for these 2 groups were compared. The authors conducted chi-squared tests for sex, age, care, CCI, residential area, and the presence or absence of symptoms at home. Three logistic regression models were adopted to investigate the effects of home health care services and home-visit nursing care on deaths at home.
Model 1 was a single-variate regression model and Model 2 was a multivariate regression model adjusted for the covariates. Based on the possibility of providing home health care and home-visit nursing care at home, 25 the authors constructed Model 3 for the 13 areas in Fukuoka Prefecture as multilevel. 26 In this case, the primary level was the patient and the secondary level was the secondary medical area. The model was evaluated using Akaike's information criterion (AIC).
Statistical significance was set at P < 0.05. Data were extracted using the SQL Server 2014, and all analyses were performed using Stata ver.14.2 (Stata Corp, TX, USA).
Ethical considerations
The data used in this study were anonymized. This study was approved by the Ethics Committee of Kyushu University.
Result
Table 1 shows the characteristics of the participants (n = 6435; 61.7% men). Average age was 81.9 years (standard deviation [SD] ±4.9), and the median CCI score was 6. Among the 13 secondary medical areas, Kitakyushu had the largest proportion of patients (26.3%).
Participants' Characteristics at Baseline
P-value <0.001 across spending trajectories, Chi-square test to compare proportions.
CCI, Charlson Comorbidity Index; IQR, interquartile range; SD, standard deviation.
Table 2 shows the details of the home medical resource use. The number of patients who used home health care services was 75 (1.2%), and enhanced HCSCs with beds was 41 (0.6%). There were 453 (7.0%) home-visit nursing care users.
Details of Home Health Care Resource Users
HCSCs, home care support clinics/hospitals.
Table 3 shows the results of the 3 models used to estimate the relationship between the use of home health care services and home-visit nursing care and death at home. In all models, enhanced HCSCs, enhanced HCSCs with beds, conventional HCSCs, home-visit nursing care, and severe nursing care were significantly associated with death at home.
Association Between the Utilization of Home Care Resources and Death at Home
Multivariate logistic regression models adjusted for sex, age, care-need level, and CCI as covariates.
The explanatory variables were divided into 2 levels. The primary level was individual patients, and the secondary level was the secondary health care area. In addition, multilevel logistic regression models adjusted for sex, age, care-need level, and CCI as covariates.
AIC, Akaike information criterion; BIC, Bayesian information criterion.
Model 3 showed that those who used enhanced HCSCs were 4.44 times more likely to die at home (odds ratio, OR: 4.44; 95% confidence interval, CI: [1.47–13.42]); those who used enhanced HCSCs with beds were 8.66 times more likely to die at home (OR: 8.66; 95% CI: [4.31–17.40]); those who used conventional HCSCs were 5.78 times more likely to die at home (OR: 5.78; 95% CI: [1.86–17.94]); and those who used home-visit nursing care were 1.86 times more likely to die at home (OR: 1.86; 95% CI: [1.42–2.44]).
Compared with patients with no care needs, those with the most advanced level of care needs were 3.89 times more likely to die at home (OR: 3.89; 95% CI: [2.92–5.18]). Sex, age, CCI score, and secondary medical care areas were not significantly associated with death at home. In Model 3, the variance of random effects was not significant, but the improvement in the model was due to the improvement in Log-likelihoods, AIC, and Bayesian information criterion (BIC).
Discussion
This retrospective study found that the continued use of home health care services and home-visit nursing care was associated with improved end-of-life care at home in older patients with cancer. The continued use of both home health care services and home-visit nursing care was positively associated with death at home, with the highest effect of use of enhanced HCSCs with beds equipped with 24-hour, 365-day physician visits and home nursing.
Recently, several Japanese researchers have reported that areas with abundant home health care resources had significantly more death at home. 25,27,28 In other words, to improve the quality of end-of-life care by increasing the proportion of deaths at home, desired by many patients who are terminally ill, the priority of health policy should be to establish a system for the provision of home health care services and home-visit nursing care.
In this study, the probability of death at home was not significant for any region, as represented by the 13 secondary medical districts in Fukuoka Prefecture (Table 3, Model 3 results). However, the multilevel logistic regression model adjusted for region as a random effect proved that the continuous availability of home health care services and home-visit nursing care was more likely to be associated with death at home. Therefore, the findings are consistent with that of previous literature.
Compared with users of other HCSCs, those who used enhanced HCSCs (with or without beds) and conventional HCSCs were significantly more likely to die at home for the following reasons. The first is the home care system of the facility. Previous studies have reported that the use of enhanced HCSCs (with or without beds) and conventional HCSCs is effective in reducing readmissions, with more deaths occurring at home, and timely management of emergency house calls when patient conditions deteriorate. 20,21
Enhanced HCSCs (with or without beds) and conventional HCSCs provide home health care services during the day and night, whereas other HCSCs attend to home calls and visit homes as an adjunct to their practice. This means that enhanced HCSCs (with or without beds) and conventional HCSCs have the following facility criteria: (1) contact doctors and nurses 24 hours and 365 days; (2) provide home visits and home nursing care 24 hours and 365 days; (3) accept patients for admission or arrange admission to a linked medical institution in an emergency; and (4) cooperate with local medical institutions and welfare services. 18
Further, most conventional HCSCs and other HCSCs have 1 full-time doctor, whereas enhanced HCSCs (with or without beds) have 3 or more full-time doctors compared with HCSCs. Therefore, they are likely to be more flexible in dealing with sudden changes in the condition of older patients with cancer and complex medical procedures such as palliative care.
In 2022, HCSC facility standards needed to consider quality of death and QOL, as requirements such as creating guidelines on appropriate decision-making support were added to the HCSC facility standards. 17,29 The current study results showed a strong association between death at home and severity of care. People with cancer near their end of life as their level of care progresses 23 and they are less willing to use active medical intervention. 11,14 People who use care resources die more at home, 1,30 confirming a scenario similar to that reported in previous studies.
As older patients with cancer have multifaceted health care needs, it is essential to have a home health care provision system in the community as the core of care, capable of attending to emergencies and providing urgent hospital admissions, equipped with general medicine and palliative care departments, and capable of working closely with patients' home. 31
Most previous studies have suggested that early intervention in palliative care and the involvement of a home palliative care team improve the possibility of death at home 32 and that the provision of multidisciplinary professional health and care services increases deaths at home. 1,30
A previous report showed that enhanced HCSCs with beds were particularly effective in reducing the length of hospital stay. 20 In this study, older patients with cancer who used the enhanced HCSC beds were seamlessly transferred to hospital admission when their condition deteriorated and to home care after recovery. The necessary medical and nursing services were provided in an integrated and continuous manner until end-of-life care, which may have contributed to high-quality, comprehensive home care through multidisciplinary cooperation.
Another point to note is the inpatient functions provided by home health care services. In all analytical models in this study, the use of enhanced HCSCs without beds had a lower OR for death at home than conventional HCSCs, which consisted of a mix of beds and without beds. This may be due to the fact that when enhanced HCSCs had no beds, patients had to be admitted to hospitals in case of an acute deterioration, which weakened the relationship between the patient and their family doctor and did not reflect the patient's wishes.
The use of home-visit nursing care is another point to be noted. A high proportion of the home care group used home-visit nursing care (>90%). This revealed that older people with cancer spent their lives with the support of home-visit nursing care, which helps them stay in their familiar home environment. It can also be inferred that nurses and home nursing stations within hospitals and clinics worked together with primary physicians and supported the patients in their recuperation and end-of-life care at home through an effective interaction process.
Prior studies have reported that the use of home-visit nursing care contributes to a reduction in death at home and hospital admissions. 14 This study suggests that home-visit nursing care is a strong backup and important for primary care physicians.
The Ministry of Health, Labour and Welfare (MHLW) has reported changes in the place of deaths in Japan after 2020 due to the impact of the COVID-19 pandemic. Deaths at home increased to 17.2% in 2021, whereas hospital deaths decreased to 65.9%. 4
This is due to a number of factors, including an increase in the number of patients and their families willing to receive home care or spend the last days of their lives at home, as hospitals restricted visits due to the pandemic. 33 During the pandemic, health care was under pressure and people could not be hospitalized as hospital beds were reserved for patients with COVID-19 infection. 34 The Government of Japan has highlighted the need to establish a system to ensure the stable and continuous provision of medical and nursing services at home in the event of a similar crises such as the COVID-19 pandemic and natural disasters. 35
In this study, a small proportion of older patients with cancer were in the home care continuation group (7.4%). However, the results showed a significant difference in the proportion of deaths at home in the continuing home care group (25.7%), which was ∼3.3 times higher than that in the non-continuing group. This suggests that the utilization of home health care resources is likely to be effective for those who wish to receive end-of-life care at home.
With the aging population, cancer has been the leading cause of death among Japanese people since 1981. Cancer survival rates are increasing for many organ sites, 36 and the demand for home care for patients with cancer is expected to increase in the future. In this study, enhanced HCSCs with beds and home-visit nursing care facilities were the most effective home health care resources for providing end-of-life care to older patients with cancer.
The study findings are crucial in assessing how limited resources can be effectively used for end-of-life home care for older patients with cancer. The study covered all 75-year-old and older residents living in Fukuoka Prefecture, which has high per capita medical costs and an abundance of hospital beds. 37 Presently, enhanced without beds get higher reimbursement than conventional HCSCs under the reimbursement system.
However, end-of-life care for older patients with cancer at home was primarily facilitated by enhanced HCSCs with beds, followed by conventional HCSCs. To expand the role of enhanced HCSCs in end-of-life care for older patients with cancer at home, it is necessary to evaluate bed availability, physician coverage, and collaboration with other clinics. Conducting an objective evaluation of these factors would aid in the development of improved home health care services.
It is essential to maintain objectivity when evaluating these factors to ensure that home health care services are effective and meet the needs of patients. While regional variations exist in both resources and circumstances, implementing a reimbursement system that supports functional differentiation and coordination within the home health care delivery system would enhance resources and promote the aging in place of older patients with cancer. This would also lead to an improvement in the quality of end-of-life care.
According to the MHLW, in 2021, enhanced HCSCs (with or without beds) in Japan accounted for 25.9% of all HCSCs. 38 If the number of nurses engaged in home-visit nursing care is to be increased to ∼30% of the proportion of deaths at home in the Netherlands, France, and other countries, ∼150,000 nurses will be needed. 39,40 Home health care in Japan is insufficient in terms of both quality and quantity. 35 It is necessary to create a home health care provision system in each region that includes not only doctors, but also visiting nurses and caregivers, to provide care to people who wish to receive end-of-life care at home.
This study had several limitations. First, it was conducted using data only from residents of Fukuoka Prefecture, Japan, limiting its generalizability. 37 Second, patients who received home nursing care provided by nurses from hospitals and clinics were excluded, as no home nursing instructions were issued.
Third, although end-of-life care at home is influenced by patients' wishes, living conditions reflecting family structure, characteristics, and socioeconomic factors were not identified in this study. Fourth, because the study focused on the use of home care and nursing, it did not include clinical data of individual patients (eg, disease progression or test results). Hence, the data might have been influenced by residual confounding factors. Finally, the possibility of some patients moving from home to a nursing home during the follow-up period was not addressed.
In conclusion, this retrospective study found that the continued use of home health care resources by older patients with cancer improves the end-of-life care at home. In particular, the current study findings suggest that promotion of agencies with enhanced HCSC, beds, and home-visit nursing care functions is advantageous when providing home health care services to patients with cancer. The current study provides useful information to consider home health care for patients with cancer as part of a community-based integrated care system.
Footnotes
Acknowledgments
The authors thank the Fukuoka Prefecture Association of Latter-Stage Elderly Healthcare for providing health care claims database. The authors also thank Miwa Shiratani, Home Hospice Shizuku Representative; Yoriko Hirano, Home-Visit Nursing Station Hana General Manager; and Manami Miyagawa, Home-Visiting Nurse, for their cooperation in providing information regarding home care support initiatives.
Authors' Contributions
Ms Yamao designed the study, collected and analyzed the data, and wrote the manuscript. Dr. Babazono contributed to the study design, data interpretation, and contributed extensively to the preparation of the manuscript. Ms Liu contributed to study design, data collection and interpretation, critical review, and manuscript revision. Mr Li, Ms Ishihara, Dr. Yoshida, Ms Kim, and Mr Jamal contributed to data collection, interpretation, and manuscript revision. All authors approved the final version and are responsible for submitting the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
Supplementary Appendix S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.