
Abstract
Accountable care organizations (ACOs) are often tasked with helping providers to deliver care efficiently and with higher quality outcomes. For an ACO to succeed in delivering efficient care, it is important to direct resources toward patients who exhibit the greatest levels of opportunity while focusing attention toward mitigating their needs. Home-based palliative care (HBPC) services are known to address patient needs for those with serious illness while decreasing the total cost of care (TCC). In this retrospective review, ACO researchers reviewed cost, quality, and utilization patterns for 3418 beneficiaries within a Medicare Shared Saving Program approaching the end of life comparing decedents who received HBPC versus those who did not receive the service. Those individuals who received HBPC services were significantly less likely to be hospitalized (51% reduction in the HBPC group), more likely to use hospice (70% vs. 43%; P = 0.001), and their TCC was less than that of those who did not receive the service ($27,203 vs. $36,089: P = 0.0163). Although more research needs to be done to understand the specific components of care delivery that are helpful in decreasing unnecessary utilization, in this retrospective review in an accountable care population, HBPC is associated with a significant decrease in cost and utilization in a population approaching end of life.
Introduction
Accountable Care Organizations (ACOs) participating in the Medicare Shared Savings Program (MSSP) are rewarded by providing high-quality care with a focus on quality performance and appropriate resource utilization, resulting in decrease in the total cost of care (TCC) per beneficiary. 1 The Center for Medicare and Medicaid Services (CMS) provides ACOs with beneficiary-level claims data that can be analyzed to identify populations wherein there is opportunity to improve value.
Given that Medicare costs for the last year of life can be as high as 25% of their lifetime expenditures, 2 individuals with serious illness represent a key segment of the population wherein an ACO can impact outcomes and the patient experience of care. Patients with serious illness often experience frequent admissions to acute care facilities, higher readmissions, and high TCC. 3
Palliative care services for patients with serious illness have been demonstrated to improve outcomes and reduce cost. 4 Many hospitals and health systems across the United States now provide inpatient palliative care services for patients receiving acute care. 5 These acute care palliative services are adept at managing pain and other symptoms, goals of care, and focusing on quality of life. 6 Unfortunately, upon discharge, the ongoing need for home-based palliative care (HBPC) far outstrips the availability of resources in the community. 7
Home health care organizations, hospices, and other groups have sought to close the gap in access to community-based palliative care and provide palliative care services to patients residing within the community. 8 In addition to superior symptom management, it has been found that patients utilizing HPBC services are more likely to experience higher quality outcomes including fewer hospitalizations as well as skilled nursing facility stays. 9 It has also been discovered that strategies and partnerships geared toward increasing utilization of HBPC services for those patients and families dealing with serious illness or nearing the end of life and avoiding more costly acute care utilization can be an effective strategy to decrease TCC. 4
Furthermore, in an accountable care setting, it has been demonstrated that HBPC services improve quality outcomes for individuals through a decrease in cost and number of hospitalizations and an increase in hospice length of stay, thereby improving the value of care for ACO beneficiaries. 10
ACOs are formed by a group of coordinated health care providers and often have formal relationships with post-acute care providers including home health and hospice organizations. 11 The comprehensive service profile and 24-7 access to care often provided by home health and hospice organizations can provide the structure for many of the components necessary to build HBPC services and build a collaborative program to meet the needs of the community. 12 The claims data and provider relationships that an ACO maintains can provide the additional components imperative to assess the performance of a comprehensive HBPC program.
In this study, ACO researchers explore cost and quality outcomes resulting when a large ACO in the greater Philadelphia, Pennsylvania, area partnered with an ACO provider group and a preferred home health and hospice organization to create a nascent HBPC program to serve the needs of the community and the ACO beneficiaries. In this setting, researchers explore whether the HBPC strategy decreased the TCC for decedents who received HBPC services before death compared with those who did not.
Methodology
This retrospective review aims to examine the cost savings per CMS category associated with the utilization of a singular nascent HBPC program for patients in accountable care setting. In this study, researchers from a large Medicare ACO partnered with an existing home health organization to provide HPBC services serving overlapping communities. The intent of the analysis is to determine whether the delivery of HBPC services to an MSSP population provided superior quality and cost outcomes for enrollees. This analysis was completed using data collected from 1 MSSP and 1 HBPC provider.
Typical interventions delivered from the HBPC provider are shown in Figure 1. HBPC referrals were initiated by the patient's primary care physician, inpatient or outpatient specialists, or other clinicians involved in the patient's care, including home health nurses and care coordinators.
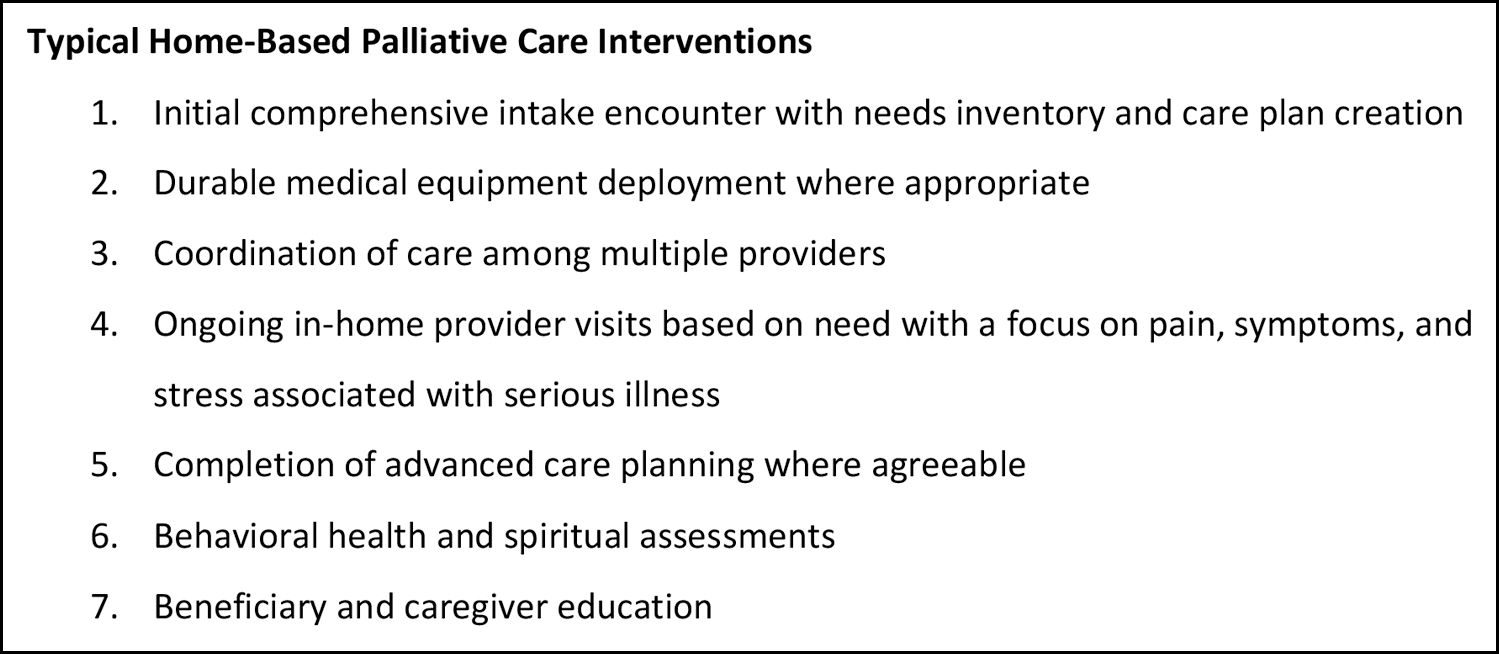
Typical home-based palliative care interventions.
Population Selection Criteria
Included in the study were 3418 ACO patients. The patients were attributed to the MSSP, deceased between May 1, 2021 and April 30, 2022, had continuous enrollment in Medicare Part A and Part B for 12 months before their death, and resided in 1 of the 5 main counties served by the MSSP. Location of care delivery was limited to home or assisted living/personal care facilities. Patients with hospice stays exceeding 180 days were excluded from the analysis. To ensure the mean age of the 2 populations (HBPC and non-HBPC) was similar, patients with ages >2 standard deviations from the mean were removed from the analysis.
Patients receiving HBPC were identified using patient lists from the service provider (n = 140). The remaining patients who met the criteria outlined above, but were not receiving HBPC from the service provider, were identified using claims and categorized into the non-HBPC group (n = 3278).
To further evaluate differences in the populations, a Charlson Comorbidity Index (CCI) was measured. The CCI is used to assess the burden of comorbidities on patient outcomes in this setting. 13 The CCI contains 17 comorbid conditions, including myocardial infarction, congestive heart failure, diabetes, liver disease, and cancer. 13 In accordance with standardized scoring for the CCI, each condition is weighted and summed to provide a cumulative index score for each patient.
Population characteristics are listed in Table 1.
Population Characteristics
Statistical significance threshold is a P-value <0.05.
CCI, Charlson Comorbidity Index; HBPC, home-based palliative care.
Data Collection and Analysis
Data for the study metrics were obtained from CMS Medicare claims and associated patient electronic medical records. Comparative analysis was performed between the HBPC group and the non-HBPC group. Statistical significance was determined using Welch's t-test, z-test, or Mann–Whitney test as given in Table 1. The primary outcome measure was the difference in total health care costs between the HBPC and non-HBPC groups, with a focus on the last 90 days of life.
Utilization metrics such as hospital admissions, length of stay, readmissions, emergency department (ED) visits, hospice use, and corresponding cost categories were used to evaluate the impact of HBPC. Cost categorization was grouped based on MSSP quarterly reporting categories and reported as such. Although most cost categories are self explanatory, it is worth mentioning that the outpatient cost category consists of outpatient facility costs including, but not limited to, hospital outpatient departments, outpatient dialysis facilities, Federally Qualified Health Centers, rural health clinic, outpatient rehabilitation facilities, and community mental health centers.
Demographic metrics (age and gender) and cancer incidence were used to identify differences between the test and control groups. Patients with ages >2 standard deviations from the mean age were removed to ensure similarity in the mean age between the 2 groups. A CCI score was reported for each patient.
The Welch's t-test with square root (sqrt) transformation was used to compare means. The method was selected to account for unequal variances between groups and prevent the data distribution from positive skew. The addition of the sqrt calculation to the data values can reduce the impact of outliers and make the data distribution closer to normal when comparing means.
This review was done in retrospect as a process improvement project in the ordinary course of data analysis within the ACO. This analysis uses aggregate Medicare reporting data as part of the typical course of ACO activities. No protected health information is included. This analysis is considered exempt from institutional review board review.
Results
This study examined quality and TCC differences between the HBPC and non-HBPC groups during their last 90 days of life. Before comparison of control and test groups, an examination of population characteristics and the use of the CCI found that the HBPC and non-HBPC populations have a similar make up based on demographic and clinical risk factors. Age was determined to be statistically higher (+2.32 years) in the HBPC population.
The TCC in the last 90 days of life per enrollee was $27,203 for the HBPC population and $36,089 for the non-HBPC population. The HBPC population demonstrated significantly lower costs by $8,886 that was found to be significantly different among the groups (P = 0.01631, Welch's t-test with sqrt transformation). Further differences in cost and utilization by category were found between the HBPC and non-HBPC populations as given in Table 2.
Cost and Utilization Comparison Results
Statistical significance threshold is a P-value <0.05.
DME, durable medical equipment; ED, emergency department; HBPC, home-based palliative care; HHA, home health agency; LOS, length of stay; N/A, not applicable; sqrt, square root; SNF, skilled nursing facility.
The results of this study demonstrate that utilization of a HBPC program is associated with statistically significant savings in the TCC per enrollee with cost differentials in each of the specified categories. Enrollees also experienced fewer admissions, greater hospice utilization, and higher hospice length of stay. The study supports the potential benefits of HBPC on utilization and cost in end-of-life care in an accountable care setting.
Discussion
In a Medicare fee-for-service population that died during the timeframe of this study period, it was determined that those who received HBPC services were more likely to have lower TCC than those who did not receive the services. Medicare beneficiaries in this review were noted to have statistically significant findings across multiple domains including the following: outpatient cost, inpatient hospitalization cost, durable medical equipment costs, and Medicare Part B drug cost. There was an increase in the utilization and cost associated with hospice, durable medical equipment, and home care.
Data analysis from this study demonstrates that the use of costly acute care is supplanted by the less costly service of homecare and hospice. Patients also were able to benefit from higher quality outcomes such as fewer acute care utilization episodes in the last weeks of life, allowing them to retain control of their care in the home. This important quality-of-life outcome is pertinent for enrollees and consistent with research exploring patient wishes for end-of-life care. 14
Although the literature shows that individuals with life-limiting illness discharged from the acute care setting may experience a worsening of symptoms at home, the use of HBPC services is an important part of care and has been shown to be beneficial in managing the physical and psychological symptoms this population experiences. 6
In addition to demonstrating superior symptom control, HBPC services have also shown a direct correlation with the reduction of TCC. 15 When compared with usual care, HBPC has shown a statistically significant decrease in health care expenses within multiple comparison groups including age, gender, insurance product, diagnosis, and ethnicity. 15 HBPC results in fewer ED visits, intensive care unit admissions, and shorter hospital lengths of stay that drive financial savings while also improving patient quality of life. 6
HBPC services have demonstrated cost benefits to patients in an accountable care setting in previous studies. In the landmark study of HBPC in an accountable care population, Lustbader and team demonstrated approximately $12,000 reductions in TCC and hospitalizations as well as increased hospice utilization in the months before death (2017). Lustbader's research is supported by the findings in this study. Although this study did not uncover that degree of difference, the current researchers did determine statistical variance and proved it over a number of CMS cost categories.
This study expands the work of Lustbader by illustrating how the unique attributes of an MSSP ACO can be leveraged to support the creation of a comprehensive HBPC program. Combining CMS claims data with the imperative for higher quality and cost stewardship from an ACO, researchers for this group were able to achieve significant results for improving outcomes for Medicare beneficiaries. This study also illustrates how synergistic existing resources in a home care and hospice organization can be leveraged to support the creation of a new HBPC program to meet the needs of an accountable care population.
This study has some limitations. The population included in this analysis is specific to the region of the ACO and associated health systems. There may be occult biases in utilization patterns or access that are not transferrable to a larger population. Similarly, this population includes a small sample size and only considers the Medicare fee-for-service population. It is unclear whether this effect would be experienced or enhanced in a population covered by a Medicaid or managed insurance product. Given the sample size, small fluctuations in TCC or quality may result in an under-representation or exaggeration of the response.
Patient referrals to the HBPC program were initiated by the patient's primary care physician, inpatient or outpatient specialists, or other clinicians involved in the patient's care including home health nurses and care coordinators. It is thus possible that there was a referral bias inherent to the study population. For example, it is possible that the care team members referred a population with a higher illness burden into the program while not referring a population that was healthier.
Age-based analysis showed that there was a difference in the age between the HBPC and non-HBPC groups. The difference may lead to speculation about increased likelihood for referral for an older population regardless of illness burden. The use of the CCI did not reflect differences in the level of morbidity or survival predictability between the groups.
Given the limitations of race, ethnicity, and primary language data reporting in CMS claims, researchers in this study were unable to analyze health equity, quality, or cost for under-represented populations.
And finally, this study is done as a data review in retrospect. There is no prospective analysis nor randomization or age-matched control group. Although the analysis does not show differences in gender, CCI, or the diagnosis of cancer, other differences in the population may emerge when comparing populations in a prospective analysis. Prospective study design and statistical analysis would bring further credibility toward the hypothesis that HBPC decreases cost and utilization.
In conclusion, the use of HBPC services is shown to be associated with a decrease in acute care utilization and thereby TCC through earlier hospice referral. In the current setting of strained Medicare financial resources, ACOs must continue to demonstrate cost avoidance through such programs that drive utilization consistent with patient goals and avoid the use of costly hospitalizations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.