
Abstract
In response to the opioid epidemic, the Centers for Disease Control and Prevention released best practice recommendations for prescribing, yet adoption of these guidelines has been fragmented and frequently met with uncertainty by both patients and providers. This study aims to describe the development and implementation of a comprehensive approach to improving opioid stewardship in a large network of primary care providers. The authors developed a 3-tier approach to opioid management: (1) establishment and implementation of best practices for prescribing opioids, (2) development of a weaning process to decrease opioid doses when the risk outweighs benefits, and (3) support for patients when opioid use disorders were identified. Across 44 primary care practices caring for >223,000 patients, the total number of patients prescribed a chronic opioid decreased from 4848 patients in 2018 to 3106 patients in 2021, a decrease of 36% (P < 0.001). The percent of patients with a controlled substance agreement increased from 13% to 83% (P < 0.001) and the percent of patients completing an annual urine drug screen increased from 17% to 53% (P < 0.001). The number of patients coprescribed benzodiazepines decreased from 1261 patients at baseline to 834 at completion. A total of 6.5% of patients were referred for additional support from a certified alcohol and substance abuse counselor embedded within the program. Overall, the comprehensive opioid management program provided the necessary structure to support opioid prescribing and resulted in improved adherence to best practices, facilitated weaning of opioids when medically appropriate, and enhanced support for patients with opioid use disorders.
Introduction
The opioid epidemic has influenced the core practice of medicine and touched countless lives. Chronic pain is a major contributor to morbidity in the United States, with an estimated 50 million US adults living with chronic pain. 1 Although prescription opioids offer a powerful method for treating pain, they confer an increasingly recognized risk. Approximately 12%–29% of patients prescribed an opioid for chronic pain will misuse the prescription. 2 –4 Even short courses of opioids are not without risk. Patients prescribed a 7-day course of opioids were found to have a 15% risk of addiction or dependency, with the risk increasing to 35% after a 1-month course. 5
In 2016, the Centers for Disease Control and Prevention (CDC) published best practice recommendations to guide chronic opioid prescribing in primary care. 6,7 These guidelines were widely accepted as best practice, and many states implemented stated recommendations as prescribing regulations. 8 –11 In the years following, 39 states implemented regulations that placed additional limitations on opioid prescribing. 9,11 Although there has been considerable variation between states laws, the common theme has been the intent to support safer opioid prescribing. 9,11
Despite the widespread acceptance of the need to improve safe opioid prescribing, the practical implementation of these standards has been challenging. 12,13 This study describes the development of a multifaceted team-based approach to support clinicians in implementing a comprehensive approach to opioid stewardship.
Methods
The authors developed and implemented a comprehensive opioid stewardship program across a large primary care network in Upstate New York between 2018 and 2021. The primary care network included 44 primary care practices caring for >223,000 adult patients by the end of 2021. The quality initiative was structured around 3 tiers: (1) implementing best practices around opioid prescribing consistent with the CDC recommendations, (2) developing opioid weaning protocols for patients, when medically appropriate, and (3) supporting patients when opioid use disorders were identified.
Patient participants
Patients 18 years and older prescribed at least a 90-day supply of an opioid in the prior 6 months were defined as receiving “chronic therapy” and enrolled in the intervention. Patients receiving opioids for pain related to malignancies, substance use disorder, or whose opioid regimen was not prescribed by a primary care provider were excluded from the intervention.
Formation of best practices and tool kit
Before the intervention began, a quality committee including physicians, registered nurses, practice managers, and a clinical pharmacist developed a best practice toolkit for opioid prescribing.
The best practice recommendations, along with resources available to support the program, were presented at a 2-hour educational session attended by 224 physicians and advance practice providers (APPs) employed by the primary care network. This presentation introduced the alignment of network expectations with national guidelines along with the resources available to support providers. 6,7,14,15 Central to the toolkit were recommendations for monitoring of urine drug screens and functional status, managing patient expectations, and improving provider–patient communication. The toolkit also included best practices for tapering opioids, materials to support difficult conversations, scripts for staff, and patient mailings created by the quality committee.
Three tier intervention
The intervention was structured around 3 tiers: (1) implementing best practices for safe opioid prescribing, (2) developing opioid weaning protocols when medically appropriate, and (3) supporting patients when opioid use disorders were identified (Fig. 1).

Three-tier approach to comprehensive opioid management.
Tier 1
The first tier focused on the implementation of best practices for safe opioid prescribing. Consistent with the CDC guidelines, these best practices established expectations for controlled substance agreements, annual urine drug toxicology screens, naloxone reversal kits, and ongoing assessments to ensure the benefits of therapy continued to outweigh the risks. Monitoring parameters included percent of patients prescribed chronic opioids who had (1) a controlled substance agreement in place, (2) a toxicology screen within the past year, (3) a naloxone prescription, and (4) a concurrent prescription of a benzodiazepine.
These data were readily accessible to clinicians to identify gaps in recommended care. Data were presented to clinicians through reports in an opioid dashboard and in quarterly reports delivered through email. Benchmarked reports were also shared with practices and clinicians in February 2021, which was the midpoint of the intervention. Providers performing significantly above the network mean received an accompanying letter recognizing their success.
Providers performing below the network mean received an accompanying letter reiterating the importance of safe opioid prescribing and offering resources to address barriers to practice change. Throughout the intervention, a program manager served as a resource for identifying and sharing “best practices” across practices and assisting with implementation of new workflows.
Tier 2
The second tier focused on weaning opioids when medically appropriate. As recommended by the CDC, the best practice guideline advised carefully assessing the risk and benefits of regimens including ≥50 morphine milligram equivalents (MMEs) per day and avoiding prescribing or carefully justifying the use of regimens including ≥90 MMEs per day. 6,7 Consistent with the CDC's 2022 update, weaning of opioids to safer levels was encouraged, but the decision to wean was left to the prescribing clinician in partnership with the patient. 16 An experienced clinical pharmacist and 3 registered nurse care managers were available to support patients and clinicians throughout the weaning process.
At the provider's request, the clinical pharmacist would develop weaning protocols for patients prescribed opioid regimens in whom the benefits no longer outweighed the risks of therapy. Taper plans were also provided for patients on concurrent opioids and benzodiazepines. The clinical pharmacist followed patients longitudinally, adapted the weaning protocol as needed, and provided additional recommendations for alternative pharmacotherapies to support the success of the opioid taper.
Weaning protocols were also supported by a team of experienced registered nurses (RNs) who served as opioid care managers. These experienced RN opioid care managers assisted in screening patients for pain, discussing functional goals, identifying barriers to a successful wean, and providing patient education, care coordination, emotional support, and advocacy. Pain intensity and interference were assessed using the pain, enjoyment of life and general activity scale. 17 These scores were used to help guide decisions around weaning.
The opioid care managers received behavioral health training and were able to provide brief interventions to patients who screened positive for low-grade anxiety and depression throughout the weaning process. Opioid care managers also received training in identifying symptoms of withdrawal and had direct support from a credentialed alcoholism and substance abuse counselor (CASAC).
Tier 3
To support patients when opioid use disorders were identified, they were provided direct access to a CASAC, and medication-assisted treatment (MAT). The CASAC was an experienced counselor available to address emerging substance abuse and/or mental health concerns. The CASAC served as both a centralized and as a “mobile” resource who traveled among the 44 practices to support clinicians and meet with patients.
MAT was a key component to supporting patients in whom opioid use disorders were identified. MAT was provided by their primary care physician or through referral to addiction psychiatry. In addition to counseling and MAT, the team established links with community partners to provide a community of peer support. Developing this collaborative team-based approach provided the structure and support for primary care providers to access addiction psychiatry guidance.
Electronic record tools
Tools were developed within the electronic health record to track implementation of best practices. Clinicians and practices had the ability to generate opioid reports to assess patients on chronic opioids without recent follow-up, status of a controlled substance agreement, concurrent prescriptions for benzodiazepines, history of naloxone access, and last urine drug screen (Fig. 2). In addition, point-of-prescribing alerts were built to notify the prescriber if the patient had an active naloxone order, a urine drug screen within the past 12 months, a controlled substance agreement on file, and an appointment with the past 6 months when refills were requested (Fig. 3).
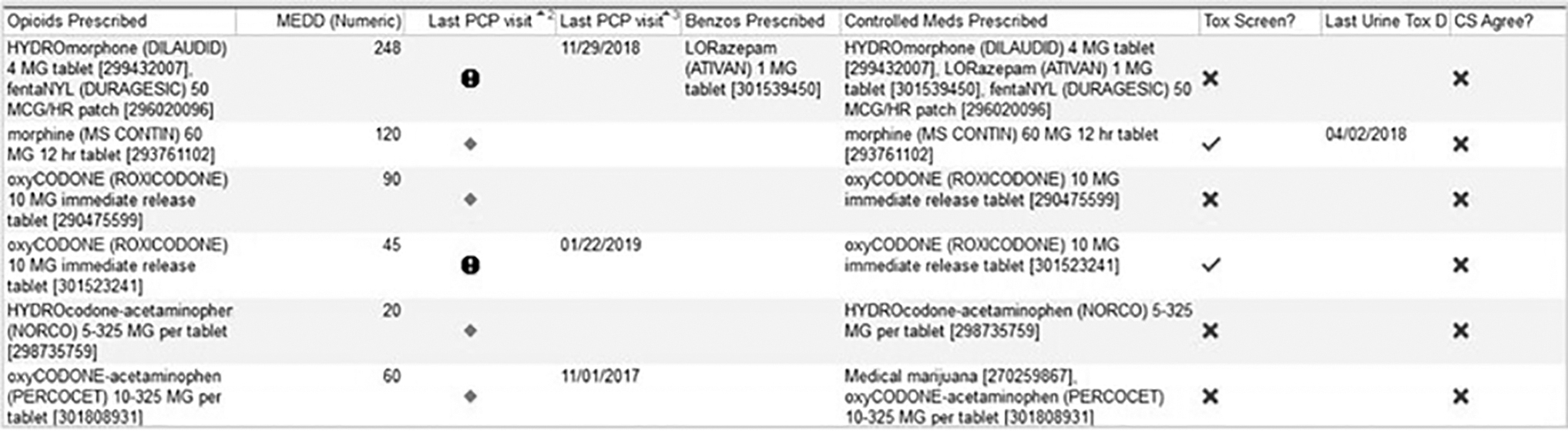
Practice-level report.
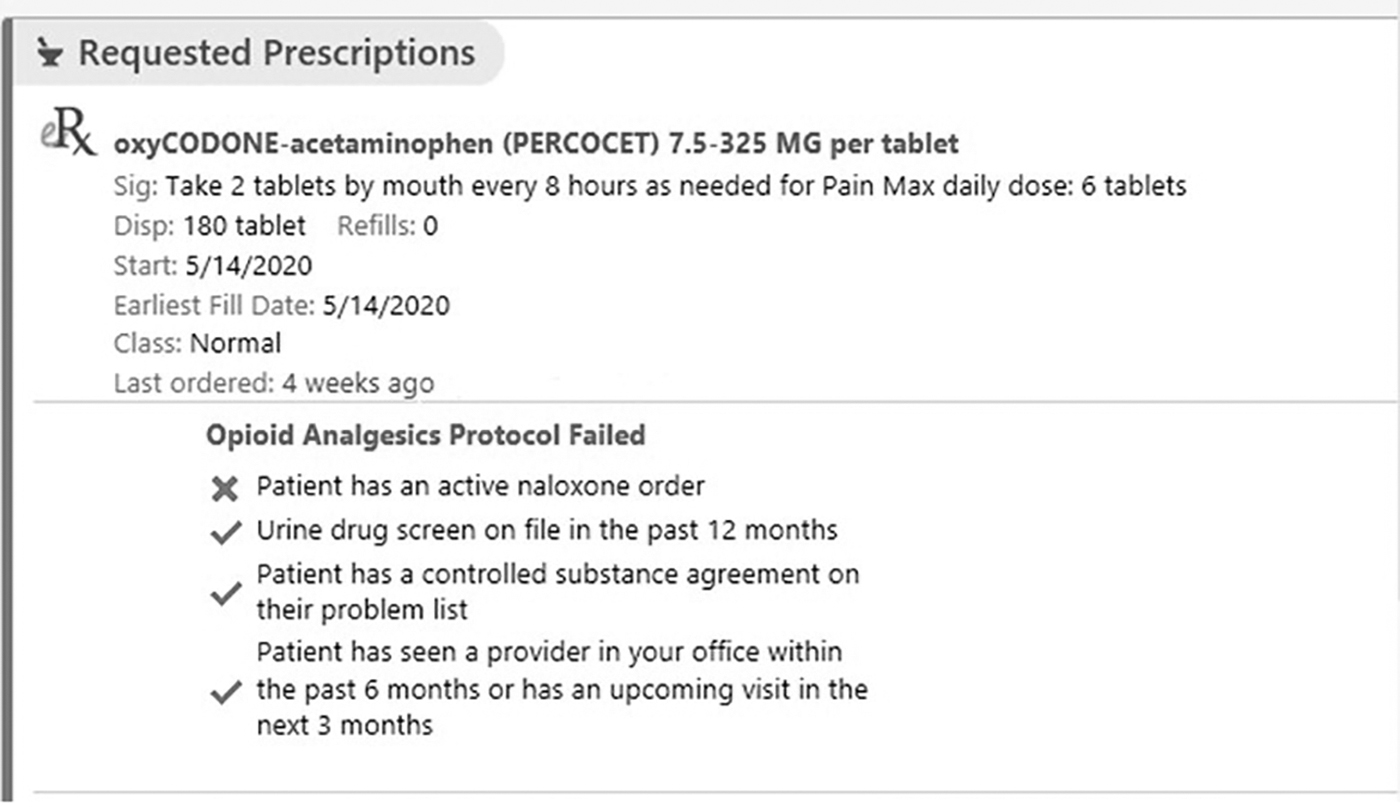
Point-of-prescribing alert.
Data collection
Data were available to individual physicians, APPs, and practice managers in real-time reports. Baseline data were collected in October 2018. Interim data for the entire network were collected in December 2020 and final network data were collected in December 2021.
Data analysis
Data analyses were primarily descriptive. The population base included adult patients on chronic opioid therapy, defined as those who were prescribed >90 days of an opioid from a primary care clinician in the prior 6 months for noncancer pain. Patients receiving opioids for substance use disorder were excluded from the analysis. Data are presented as the proportion of patients on a chronic opioid meeting each quality benchmark and were available at provider, practice, and network levels.
Institutional review board
This project was approved by the Human Studies Institutional Review Board.
Results
During the course of the intervention, the primary care network grew from 176,961 adult patients to 223,107 adult patients. Despite the growth in attributed adult patients, the absolute number of patients prescribed an opioid decreased through the course of the intervention (Fig. 4).

Growth of primary care network and prescribing of chronic opioids.
At baseline, 4848 patients were prescribed chronic opioid therapy (Table 1). Of these, ∼13% have a signed controlled substance agreement documented in the electronic health record, ∼26% were coprescribed a benzodiazepine, and 17% had a urine drug screen in the past year.
Patients on Chronic Opioids and Quality Measure Through Intervention
At the interim data analysis after the initial educational intervention and implementation of the best practices, the total number of patients prescribed chronic opioid therapy had decreased to 4176 patients. The proportion of patients on chronic opioids with controlled substance on file and recent urine drug screens had increased to 59% and 33%, respectively (P < 0.001, for both).
By the completion of the intervention, the total number of patients prescribed an opioid had decreased by >1700 despite the substantial growth in network size. The proportion of patients with signed controlled substance agreements and urine drug screens increased to 83% and 53%, respectively (P < 0.001). The number of patients coprescribed benzodiazepines decreased from 1261 at baseline to 834 in December 2021. Of the 154 patients who received services from the CASAC, 35% were from the rural primary care offices.
At baseline, <1% of prescribers were prescribing nasal naloxone; by December 2020, 75% of network providers had prescribed naloxone to 1 or more chronic opioid patients. The rate of naloxone prescribing continued to increase throughout the intervention, and at the conclusion, 100% of providers had ordered reversal kits.
Discussion
In 2017, the department of health and human services declared opioid dependence, misuse, and addiction a nationwide public health crisis. 18 Accordingly, practice recommendations have shifted from treating pain as the “fifth vital sign” to ensuring that the benefits of opioid use outweigh the risks to patient safety. 19 However, consistent adoption of national recommendations has been challenging. We found that the implementation of a novel 3-tier comprehensive opioid management program provided the structure necessary to improve adherence to opioid stewardship across a broad network primary care clinician. Overall, despite the expansion and growth of the network, the absolute number of patients prescribed an opioid significantly decreased through the course of the intervention.
The comprehensive opioid management program included 3 tiers that were critical to supporting clinicians and patients. The first tier focused on the establishment and implementation of best practices for prescribing opioids. These were guided by the CDC, but were customized by a quality committee composed of physicians and practice leaders within the primary care network. These best practices served as an agreed-upon foundation for aligning clinicians toward a common goal and resulted in significant improvements in adherence to CDC recommendations.
The second tier focused on the development of a weaning process to reduce or discontinue therapy when risks outweighed benefits. This phase was guided by opioid stewardship principles and supported by a clinical pharmacist team, opioid care managers, and pain specialists. Over the course of the intervention, the network grew by >46,000 new adult patients, many who presented on legacy regimens of chronic opioids. Despite the substantial increase in size, the number of patients on chronic regimens decreased by >1700 patients from baseline.
The third tier provided a structure of emotional support and advocacy for patients when opioid use disorders were identified and involved a CASAC and an opioid care management team. Ongoing support and evaluation of the patient were crucial for the success achieved in tapering. It is very common for opioids to mask underlying mental health disorders, such as anxiety, depression, and substance use disorders that may require additional assessments. The team found that providing this support was essential to not only support patients, but also to achieve “buy-in” from clinicians for the overall opioid stewardship program.
Interestingly, 35% of referrals to the embedded CASAC were from the rural primary care offices. These data are consistent with national trends indicating that rural residents have limited access to behavioral health services, MAT options, and a fear of stigma when seeking help. 20 –22 The approach of providing a “mobile” CASAC to support practices, including the rural clinicians, was important to the success of the intervention and validates the need to expand access to addiction treatment.
The key factors that contributed to the success of the intervention included aligning clinicians around a common set of internal guidelines and values, providing the structure and support necessary for clinicians to make changes, sharing real-time data to guide interventions toward defined goals, and developing a multidisciplinary collaborative approach to support both clinicians and patients in the process.
Although many of the components of this initiative have been previously studied, the 3-tiered approach was unique in its comprehensive nature and resulted in measurable and progressive improvements over 4 years. 12,23 –25 Other initiatives have similarly demonstrated benefits using electronic heath record notification to support prescribing. 26,27 Additional studies have found that educational interventions for opioid prescribing were associated with modest improvements in opioid prescribing. 12,24,28
Further studies have demonstrated the benefits of using standardized prescribing practices and patient-level dashboards to monitor patient risk and guideline adherence. 23 The team's intervention extends upon these earlier studies by implementing many of these initiatives in a coordinated multitier initiative and demonstrating their viability across a broad primary care network.
This initiative resulted in significant improvements, but had several limitations. First, this initiative was developed as an implementation project using a coordinated framework. As an implementation project, comparative practices were not tracked outside of the intervention sites. Second, the team was not able to reliably trend mean MMEs of opioids prescribed due to technical constraints. Third, this initiative took place at 44 practices spread across 7 counties, but all practices shared a common electronic health record and administrative structure, which may limit broader generalization.
Overall, the authors found that a comprehensive opioid stewardship program resulted in improved adherence to best practices, facilitated weaning of opioids, and provided the necessary support for patients with opioid use disorders. This 3-tiered approach drew upon published best practices and provided the necessary structure to support opioid prescribing while improving care for patients. Key components to success were aligning clinicians and teams around a common set of guidelines and values, providing the structure and support necessary for clinicians to make changes, sharing real-time data to guide interventions toward defined goals, and developing a multidisciplinary collaborative team.
Footnotes
Acknowledgments
The authors thank Patrick Seche, MS, CASAC, for his contributions and support of the CASAC team. The authors thank Therese Dale, RN, and Barb Myers, RN, for their role as opioid care managers and the Olsan Internal Medicine Group for piloting early initiatives. The authors also thank and acknowledge the ongoing efforts among their colleagues in Highland Family Medicine and Strong Internal Medicine.
Authors' Contributions
Dr. Fortuna contributed to conceptualization, supervision, funding acquisition, investigation, methodology, formal analysis, and writing. Dr. Venci contributed to conceptualization, funding acquisition, investigation, methodology, formal analysis, and writing. Dr. Johnson was involved in conceptualization, investigation, and writing. Mr. Clark carried out conceptualization, supervision, funding acquisition, methodology, administration, and writing. Ms. Stetzer carried out project administration, investigation, and writing.
Dr. Schlagman took care of investigation and writing. Ms. Vandermark took care of supervision, investigation, and writing. Dr. Nasra was involved in methodology and consultation. Dr. Martin-Stancil-El was involved in methodology and investigation. Dr. Judge was in charge of conceptualization, supervision, funding acquisition, methodology, and writing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project was funded by the Finger Lakes Performing Provider System Transformation Fund.