
Abstract
Asthma is the most common chronic disease in children, disproportionately affects families with lower incomes, and is a leading reason for acute care visits and hospitalizations. This retrospective cohort study used the Massachusetts All Payer Claims Database (2014–2018) to examine differences in acute care utilization and quality of care for asthma between Medicaid- and privately insured children in Massachusetts. Outcomes included acute care use (emergency department [ED] or hospitalization), ED visits with asthma, routine asthma visits, and filled prescriptions for asthma medications. Multivariable logistic regression was used to account for differences in demographics, ZIP codes, health status, and asthma severity. Overall, 10.0% of Medicaid-insured children and 5.6% of privately insured were classified as having asthma. Among 317,596 child-year observations for children with asthma, 64.4% were insured by Medicaid. Medicaid-insured children had higher rates of any acute care use (50.4% vs. 30.0%) and ED visits with an asthma diagnosis (27.2% vs. 13.3%) compared to privately insured children. Only 65.4% of Medicaid enrollees had at least one routine asthma visit compared to 74.3% of privately insured children. Most children received at least one asthma medication (88.6% Medicaid vs. 83.3% privately insured), but a higher percentage of Medicaid-insured children received at least one rescue medication (84.0% vs. 73.7%), and a lower percentage of Medicaid-insured (46.1% vs. 49.2%) received a controller medication. These results suggest that opportunities for improvement in childhood asthma persist, particularly for children insured by Medicaid.
Introduction
Asthma is the most common chronic disease of childhood and a leading cause of preventable and costly emergency department (ED) visits, hospitalizations, school absences, and lost parental workdays. 1 –3 Although effective strategies exist for reducing asthma symptoms, nearly half of children with asthma have poorly controlled disease, suggesting that some of the acute care utilization experienced by children with asthma can be attributed to suboptimal management in the ambulatory setting. 3 Asthma is more prevalent and more likely to be poorly controlled among children in lower income, Black, and Puerto Rican populations compared to children in higher income and White populations. Poorly controlled asthma results in higher ED visit and hospitalization rates. 4 Children in these populations are also more likely to be insured by Medicaid than by private insurers 5 and to have worse access to health care.
Prior studies comparing asthma utilization and outcomes based on insurance type found lower medication adherence, higher rates of poorly controlled asthma, higher ED and hospital utilization rates, and differences in the number of outpatient visits for Medicaid-insured compared to privately insured children with asthma. 6 –9 However, these studies relied on survey data collected between 1991 and 1996 or claims data from 2005 to 2007 and from 2006 to 2014. These studies were conducted before passage of the Affordable Care Act, which required routine care such as preventive services (including well-child visits and vaccinations) be covered without cost sharing, which may have impacted asthma care and outcomes. 10,11 Additionally, the comparisons of studies conducted from 2005 to 2007 did not compare children with different insurance types in the same states, meaning results may be biased by children's exposure to different clinical care environments. 8
Numerous interventions to address asthma disparities 4,12 and changes in health care delivery have taken place nationally and at the state level since these previous studies were conducted, but Massachusetts has not, to the authors' knowledge, adopted any asthma-specific policy changes either during or since the current study's time frame. These changes include those related to the Affordable Care Act 13 and increased use of pediatric quality metrics by private insurers and Medicaid. For example, a 2014 rule change expanded the type of clinicians that can be reimbursed for providing preventive services to Medicaid/CHIP enrollees, allowing state Medicaid programs to reimburse for asthma-related interventions in nonclinical settings. 14 Expansion of indications for newer asthma controller medications since prior studies were conducted may also have differentially affected Medicaid and privately insured populations.
A better understanding of differences in recent patterns of health care utilization among children with asthma can inform targeted strategies to improve care, particularly with frequently changing clinical guidelines. 11 This study aimed to compare patterns of nonambulatory setting acute care, ambulatory care, and medication utilization for Medicaid versus privately insured children with asthma in Massachusetts. The authors hypothesized that Medicaid-insured children with asthma would have higher rates of acute care utilization and lower quality of outpatient care (measured by lower rates of routine care use), higher rates of rescue medications, and lower use of controller medications.
Methods
Data and analytic sample
Children with asthma were identified using the Massachusetts All Payer Claims Database (MA APCD) (v8.0, 2014–2018), obtained from the Massachusetts Center for Health Information and Analysis. 15 The MA APCD includes health insurance enrollment and claims data for private insurers and Medicaid (including fee-for-service and managed care). 15 The sample included children with asthma aged 2–17 years in 2015–2018, and 2014 data were also used to identify children with persistent asthma as detailed below.
Based on prior studies, the authors considered a child to have asthma if they met at least one of the following criteria in that year: (1) 1 or more hospital visits (including inpatient, ED, and observation stays) with a principal or secondary diagnosis of asthma, 16,17 (2) 2 or more ambulatory care visits with a principal or secondary diagnosis of asthma, 18 or (3) at least one ambulatory care visit with a principal or secondary asthma diagnosis and at least one asthma medication. 18,19 Supplementary Appendix Tables S1 and S2 include a complete list of International Classification of Diseases, Ninth Revision (ICD-9) and ICD-10 codes and asthma medications. Briefly, asthma medications included rescue medications (short-acting β2-agonists) and controller medications (long-acting β2-agonist, inhaled corticosteroid, methylxanthines, mast-cell stabilizers, or combinations). 20 Children with diagnoses of emphysema, chronic obstructive pulmonary disease, and cystic fibrosis in any year were excluded from the analysis. 16,21 Observations of children with less than 6 months of health insurance enrollment or residence in the calendar year and those not residing in Massachusetts for at least 6 months during the calendar year were also excluded from that child-year. Those with multiple insurance types in a year (ie, both Medicaid and private) were assigned to the modal type by number of months. Those with missing or erroneous data for age and/or sex were excluded, while those without a ZIP code were assigned to a “missing” ZIP code category.
Measures
The primary outcome variables are indicators of acute and routine care for asthma. Specifically, any acute care use (ED visit, hospitalization, or hospital observation visit), ED visits and hospitalizations (both “any” and counts for each), any routine visit for asthma, any asthma medication, and rescue medication and controller medications (both “any” and numbers for each) were examined. For rescue and controller medication use, both numbers of filled prescriptions for each (eg, 1 inhaler = 1 fill) and the number of days' prescribed use as a measure of care quality were measured.
For asthma-specific acute care utilization measures, only ED or hospital utilization with an asthma code as the principal diagnosis code were counted. Revenue codes, place of service codes, and CPT codes were used to recognize various kinds of utilization. A routine visit for asthma was defined as a well-child visit with a principal or secondary asthma diagnosis, or an evaluation and management visit on the same day as a well-child visit.
The key explanatory variable is an indicator of whether the child is enrolled in Medicaid (including Children's Health Insurance Program) versus private insurance. Child demographics included age (2–4, 5–11, and 12–17 years) 22 and child sex (male or female). Child health status (other than asthma) was captured with binary indicators available in Centers for Medicare and Medicaid Services Hierarchical Condition Category software. 23,24 Persistent asthma during a year was defined using the HEDIS metric; it includes children in the asthma cohort who were enrolled for 2 continuous years and also met at least one of the following criteria in the year of interest and the year prior: (1) at least one inpatient visit with a principal asthma diagnosis, (2) at least one ED visit with a principal asthma diagnosis, (3) at least 4 ambulatory care or hospital observation visits on different dates of services with any asthma diagnosis and at least 2 medication fills on different dates for asthma medications, or (4) at least 4 medication fills on different dates for asthma medications. 18,25
Statistical analysis
Descriptive statistics on characteristics of the analytic sample were calculated, and statistical comparisons between those with Medicaid versus private insurance using chi-squared tests for binary and categorical variables and t-tests for continuous variables were conducted. The authors then examined differences in utilization of asthma-related care between these groups and estimated unadjusted logistic regression models. Results are presented as average marginal effects for the difference in predicted probabilities.
The authors used a multistep process to examine the influence of different risk factors, after accounting for other specific factors. The authors estimated multivariable logistic regression models controlling for sets of child and community-level factors. Adjustment for child demographics, including age and sex, fixed effects for calendar year, and 3-digit patient ZIP code to account for unobserved community characteristics was performed. Indicators for other diseases were then added to the model, since comorbidities may influence care utilization, and again, after also including an indicator for persistent asthma. For each model and outcome, the average marginal effects for the difference between Medicaid and private insurance are reported.
In modeling numbers of acute care visits and numbers of medications among those with any, the authors used multivariable Poisson regression analysis. Again, the indicator for Medicaid versus private insurance is the exposure of interest, and the multistep process to account for the explanatory variables described above was conducted. Results are reported as incidence rate ratios, which are interpreted as, for example, the percent change in the outcome associated with Medicaid (vs. private) insurance.
Criteria for being classified as having asthma included a single ED visit or hospitalization for asthma, meaning that acute care utilization may be higher in this group; the reason this was used as the primary analytic sample is because this group is less likely to be misclassified or have asthma as a “rule-out” diagnosis. The authors conducted a sensitivity analysis using the sample of all children with a principal or secondary diagnosis of asthma on any claim during the year, with similar inclusion criteria based on insurance enrollment and Massachusetts residence.
Standard errors in all logistic models were clustered at the 3-digit patient ZIP code level. Robust standard errors were used for Poisson models. The delta method was used to estimate standard errors of marginal effects. An alpha of 0.05 is considered significant. Statistical analyses are conducted in SAS 9.1 (SAS Corporation, Cary, NC, USA) and Stata-MP 16.0 (StataCorp, College Station, TX, USA).
Results
Asthma was identified in 10.0% of otherwise-eligible observations in Medicaid versus 5.6% private insurance, leading to a study population with 317,596 child-year observations (Supplementary Fig. S1), attributed to 171,416 unique children. Of these, 64.4% were insured by Medicaid, 43.2% were female, 49.2% were in the 5–11-year age category, and 18.0% have persistent asthma. Children with Medicaid were significantly younger, more likely to be female, more likely to have persistent asthma, and have higher rates of comorbid conditions than those with private insurance.
Acute care utilization was common, with 50.4% of Medicaid-insured children and 30.0% of privately insured children having at least one all-cause ED visit or hospitalization during the year (Table 2). Risk modeling modestly reduced but did not eliminate the gap in acute care utilization between Medicaid- and privately insured children. In both unadjusted and regression-adjusted analyses Medicaid-insured children were twice as likely to have ED visits with either a principal or other diagnosis of asthma than privately insured children (unadjusted rates: 27.2% for Medicaid vs. 13.3% for private; adjusted difference of 12.0 percentage points [P < 0.01; 95% confidence interval; CI 10.8–13.2]). Hospitalization differences for the overall sample are much smaller and children with Medicaid were not significantly more likely to be hospitalized for asthma (principal diagnosis) than children with private insurance. Among those children with acute care utilization, Medicaid-insured children had 8% [95% CI 7–9] more ED visits and 2% [95% CI 0–5] more hospitalizations with a principal asthma diagnosis than privately insured children.
Descriptive Statistics of Children with Asthma in Massachusetts All Payer Claims Database (2015–2018)
P-values are calculated using chi-squared tests. Observations are at the child-year level. Data from 2014 were used to calculate persistent asthma. Only the 5 most common hierarchical condition categories are displayed in the table.
SD, standard deviation.
Utilization Patterns of Children with Asthma in Massachusetts All Payer Claims Database (2015–2018)
Observations are child-years for children with asthma as defined in the Methods section.
Negative values indicate rates for privately insured children are higher, positive values mean rates for Medicaid-insured children are higher. For binary variables, average marginal effects are displayed as described in the Methods section. For continuous variables, incidence rate ratios are show. Numbers higher than 1 indicate rates for Medicaid insured children are higher.
Any acute care use includes ED, hospitalization, or observation stay. Data from 2014 were used to calculate persistent asthma for those in 2015.
ED, emergency department.
P < 0.01, * P < 0.05.
Routine asthma visits were more common for privately insured children (unadjusted rates of 74.3% private vs. 65.4% Medicaid; risk adjusted difference of −8.5 percentage points [P < 0.01; 95% CI −9.8 to −7.3pp]). Medicaid-insured children were more likely to have any asthma medication (unadjusted rates of 88.6% Medicaid vs. 83.3% private; risk adjusted difference of 5.1 percentage points, P < 0.01; 95% CI 4.1–6.2) and to have at least one rescue medication but were less likely to have any controller medication. These differences in medication usage persist in the number of filled prescriptions for rescue medication among those with at least one prescription; Medicaid-insured children had 7% [95% CI 5–9] more medication fills and 7% [95% CI 5–10] more days' supply of prescriptions for rescue medications compared to privately insured children. Similarly, for those with at least one prescription for a controller medication (more common for privately insured children), Medicaid-insured children had 11% fewer [95% CI −13 to −9] filled medications and 17% fewer [95% CI −20% to −14%] days' supply than privately insured children, both statistically significant differences. When patterns of medication usage were examined, many children, including those with Medicaid or private insurance, received 15–30 days of rescue medication (Fig. 1A) and 30 days of controller medication (Fig. 1B); 31.7% received greater than 30 days of controller medication in a year (32.6% for private vs. 31.2% for Medicaid), and 17.4% had greater than 90 days of controller medication in a year (18.6% for private vs. 16.7% for Medicaid).
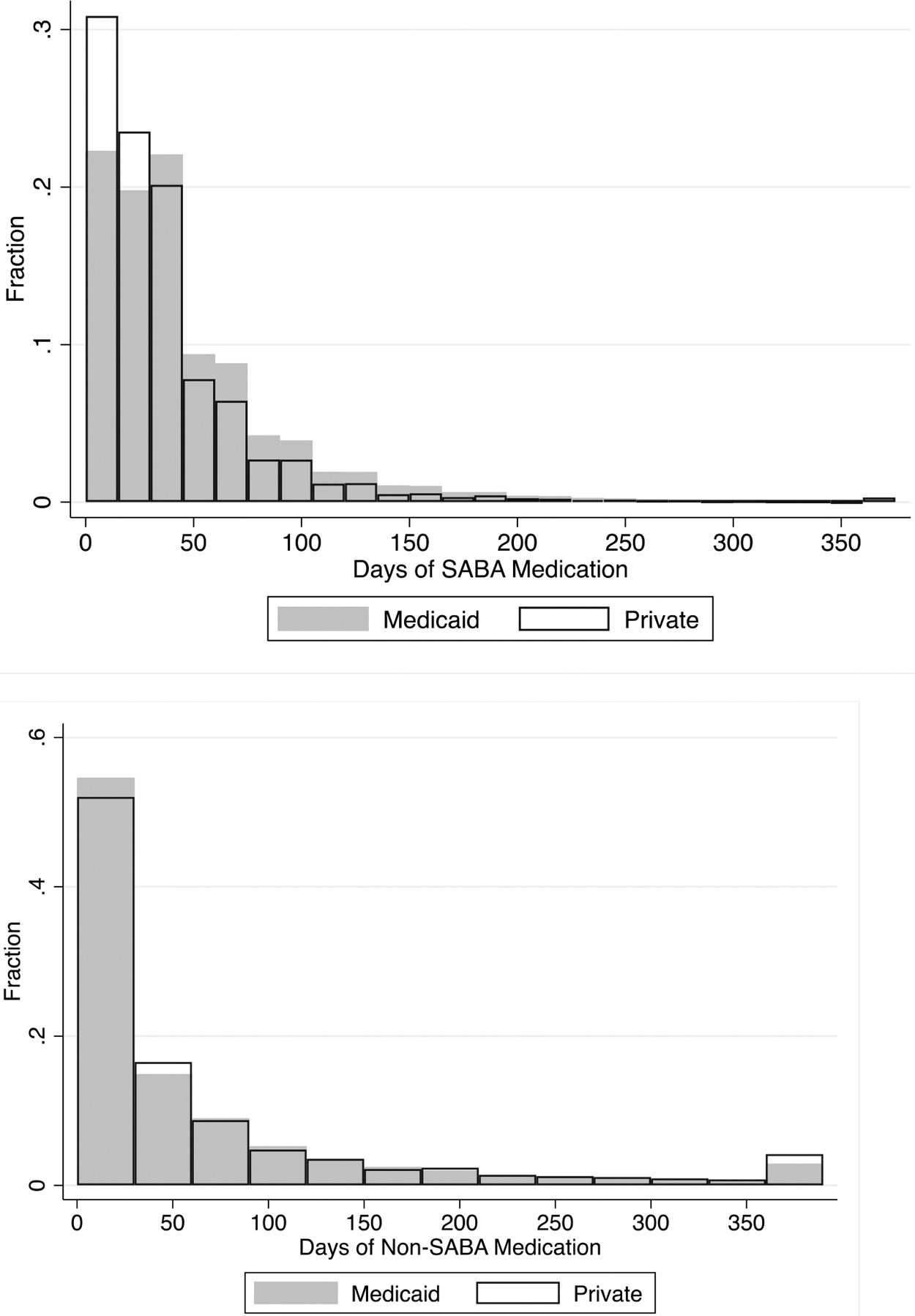
Distribution of asthma medications for children with asthma.
In the sensitivity analysis that extended the primary analysis to all children with any diagnosis code indicating asthma on any claim during the year (Table 3), very similar differences in acute care utilization were found, although the overall use and difference in use for visits with asthma is slightly less. Similar patterns in routine asthma visits (ie, higher for privately insured children), any asthma medication (ie, higher for Medicaid insured children), and rescue medication (ie, higher for Medicaid-insured children, both any use and number of fills and days' supply) were found. Different from the main asthma cohort, slightly more Medicaid-insured children had any controller medication compared to privately insured, although the higher number of fills and days' supply for privately insured children persisted as in the asthma cohort.
Utilization Patterns of Children with Any Asthma Diagnosis Code in Massachusetts All Payer Claims Database (2015–2018)
Observations are “child years,” including all children with any diagnosis code indicating asthma in the calendar year. ** P < 0.01, * P < 0.05.
Negative values indicate rates for privately insured children are higher, positive values mean rates for Medicaid insured children are higher. For binary variables, average marginal effects are displayed as described in the Methods section. For continuous variables, incidence rate ratios are shown. Numbers higher than 1 indicate rates for Medicaid-insured children are higher.
Any acute care use includes ED, hospitalization, or observation stay. Data from 2014 were used to calculate persistent asthma for those in 2015.
Discussion
This study found higher rates of acute care utilization—particularly for ED care—for Medicaid-insured versus privately insured children with asthma that were not explained by differences in demographics, health status, and asthma severity. These findings suggest that there are likely modifiable factors preventing optimal disease management. Differences in routine outpatient visits and asthma medication prescribing patterns were identified, but the relatively small magnitude of the differences suggests that they likely contribute to the disparities but do not fully explain them.
The findings of higher acute care utilization for Medicaid-insured children with asthma are consistent with studies that made similar comparisons using data from 7 to nearly 20 years before the data used in the current study. 6 –8,26,27 The consistency of the current study's findings—including lower use of routine asthma visits and controller medications—with those over the last 2 decades suggests that interventions to ensure access to high-quality asthma care for Medicaid-insured children are falling short of their goals. There are many likely reasons for this failure, including potentially modifiable factors such as inadequate dissemination and uptake of evidenced-based asthma interventions, inconsistent access to primary care, and exposure to environmental factors at home and in the community that can be difficult to remediate.
The authors found fewer routine asthma visits for Medicaid-insured children than for those with private insurance. A recent review reported a lack of adequate access to primary care can lead to increased asthma severity and poor asthma treatment adherence in Medicaid-insured children. 26 Although their data could not clarify why Medicaid-insured children have fewer routine visits for asthma, social determinants of health, such as poverty-associated chronic stress, 27,28 limited transportation, neighborhood safety, and limited access to providers who accept large numbers of Medicaid-insured children likely contribute. It is only recently that value-based care payment systems have incorporated incentives for assessing and addressing social determinants of health into contracted expectations of health care organizations in which Medicaid-insured children receive care. It will be critically important to evaluate whether such programs reduce acute health care utilization for Medicaid-insured children with asthma while also probing more deeply on why such gaps in acute care have persisted for so long.
Treatment of asthma exacerbations in acute care settings is costly for state Medicaid programs 14 ; policies that aim to improve asthma control and reduce acute care utilization for exacerbations when they do occur by substituting appropriate outpatient care, including mitigating environmental triggers, could reduce the burden of disease and reduce cost. 14 Although performance on quality measures has long been used as an incentive to stimulate innovative approaches to complex chronic disease management, 29 there is limited evidence linking common asthma quality measures focused on process, such as those developed through AHRQ's Pediatric Quality Measurement Program (PQMP) 30 and the Center for Disease Control and Prevention's EXHALE program, 31 to patient outcomes. Insurers and health systems are increasingly considering quality measures that aim to address factors known to influence health disparities, such as racism, trust, and social determinants of health. Although these constructs can be more difficult to measure, inclusion of such measures and refocusing on outcome measures that are more meaningful to patients and parents may help to address persistent asthma inequities and disparities.
This study's strengths and limitations should be considered when interpreting its findings. First, this is a single state study; however, Massachusetts has similar Medicaid eligibility limits for children, 32 higher asthma rates than many states, high rates of uncontrolled asthma, and similar racial, ethnic and socioeconomic asthma disparities in quality of care and outcomes. 33 Second, state Medicaid programs vary in factors such as eligibility requirements, provider reimbursement levels, and quality of care. Although Massachusetts's eligibility criteria are similar to many states’, 34 associations between insurance status and utilization and outcomes for children with asthma may differ across states. Third, the definition the authors used for persistent asthma requires children to be observed for 2 consecutive years and may understate the rates of persistent asthma. The persistent asthma measure is constructed using acute care utilization as one of the criteria, which could be an indicator of underuse of controller medications, poor inhaler technique, exposure to cigarette smoke or other irritants or allergens in the home, or poor quality of care rather than asthma severity. Fourth, due to a change in reporting requirements in 2016, self-insured employers are not required to report to the MA APCD, meaning that Medicaid-insured children are overreported in the dataset. 35 Fifth, race and ethnicity are not available in the MA APCD, meaning the study team could not account for known racial and ethnic disparities in asthma prevalence, care, and outcomes. Issues with poor quality race and ethnicity data in claims data are well established, and particularly for many states' Medicaid data. 36,37 The poor quality limits the potential for using large state or national claims data sets to fully isolate the role of race, ethnicity, and racism in health disparities. Sixth, other variables within and external to the health system, such as the patient-perspective factors in the Levesque access-to-health care framework, 38 likely contribute to differences in health care utilization. However, assessing these factors was beyond the scope of this study.
This study suggests that despite prior efforts to address socioeconomic disparities in asthma prevalence, quality of care, and outcomes, these disparities persist. Future studies should evaluate the effects of newer approaches to organizing and financing care, such as accountable care organizations, on quality of care, outcomes, and disparities for childhood chronic diseases such as asthma. This is a consideration of novel approaches to improve quality of care for children with asthma and insurance-associated disparities in preventable acute health care utilization for children with asthma.
Footnotes
Acknowledgments
The authors thank Erin DeCou, Valerie Evans, Suepriya Adhikari, and Michael Cooper (University of Massachusetts Amherst) for research assistance.
Authors' Contributions
Dr. Goff and Dr. Geissler conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr. Lindenauer, Dr. Krishnan, and Dr. Ash contributed to study design and critically reviewed and revised the manuscript. Dr. Shieh carried out the initial analyses, and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute or the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the National Heart, Lung, and Blood Institute [Grant No. R01 HL149875]. Dr. Ash received funding from the University of Massachusetts Center for Clinical and Translational Science-Biostatistics, Epidemiology & Research Design Component (BERD) (2UL1 TR001453-05A1). The funding source was not involved in study design or collection, analysis, and interpretation of data, writing, or in the decision to submit the article for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Appendix Table S1
Supplementary Appendix Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.