
Abstract
In the United States, there are profound and persistent racial and ethnic disparities in pregnancy-related health, emphasizing the need to promote racial health equity through public policy. There is evidence that the Affordable Care Act (ACA) increased health insurance coverage, access to health care, and health care utilization, and may have affected some pregnancy-related health outcomes (eg, preterm delivery). It is unclear, however, whether these impacts on pregnancy-related outcomes were equitably distributed across race and ethnicity. Thus, the objective of this study was to fill that gap by summarizing the peer-reviewed evidence regarding the impact of the ACA on racial and ethnic disparities in pregnancy-related health outcomes. The authors conducted a scoping review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR), using broad search terms to identify relevant peer-reviewed literature in PubMed, Web of Science, and EconLit. The authors identified and reviewed n = 21 studies and found that the current literature suggests that the ACA and its components were differentially associated with contraception-related and fertility-related outcomes by race/ethnicity. Literature regarding pregnancy health, birth outcomes, and postpartum health, however, was sparse and mixed, making it difficult to draw conclusions regarding the impact on racial/ethnic disparities in these outcomes. To inform future health policy that reduces racial disparities, additional work is needed to clarify the impacts of contemporary health policy, like the ACA, on racial disparities in pregnancy health, birth outcomes, and postpartum health.
Introduction
In the United States, there are profound and persistent racial disparities in pregnancy-related outcomes. 1 –5 For example, compared with their non-Hispanic (NH) White counterparts, NH Black people who give birth are 1.6 times more likely to deliver babies preterm and are 3.2 times more likely to have a pregnancy-related death. 2,3 Similarly, American Indian/Alaska Native people who give birth are 1.3 times more likely to deliver babies preterm and are 2.3 times more likely to have a pregnancy-related death. 2,3 Importantly, racial disparities in pregnancy-related outcomes may be perpetuated across generations, 6 emphasizing the need for intentional efforts to reduce these disparities and promote health equity.
The passage of the Patient Protection and Affordable Care Act (ACA) had the potential to improve pregnancy-related health outcomes by reducing insurance-related barriers to health care before, during, and after pregnancy. Specifically, the ACA provided options for more affordable health insurance coverage through the expansion of Medicaid, the dependent coverage provision, and the opening and subsidization of the health insurance exchanges (ie, the Marketplaces). 7 The ACA also expanded the scope of health insurance by requiring coverage of preventive care, including FDA-approved female contraception, without patient cost sharing.
There is evidence the ACA decreased the proportion of women and birthing people without insurance, increased access to pregnancy-related care, and may have improved some perinatal health outcomes. 8 –11 It remains unclear, however, whether these effects were equitably distributed across race and ethnicity. Thus, the objective of this study was to conduct a scoping review of the peer-reviewed evidence to date regarding the impact of the ACA on racial/ethnic disparities in pregnancy-related outcomes. The authors entered this review in equipoise, hypothesizing that the ACA could have either (1) reduced disparities through use of income-based criteria for coverage or (2) not reduced (ie, maintained or even exacerbated) disparities in these outcomes, due to prevailing forces of structural racism.
A detailed rationale for these hypotheses is available in Supplementary Appendix A. This study builds on a previous systematic review that focused on the impact of the ACA Medicaid expansion on perinatal insurance, health care use, and health outcomes 8 by reviewing literature investigating additional ACA provisions (eg, the dependent coverage provision), including studies that focused on women or females of reproductive age irrespective of pregnancy status, and reviewing literature that investigated additional outcomes (ie, fertility-related outcomes).
Materials and Methods
Search and study selection
The authors conducted a review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). 12 They used the search strategy outlined in Supplementary Appendix Table B1 to search PubMed, Web of Science (WoS), and EconLit for peer-reviewed studies published in English between January 1, 2010, and December 31, 2022, that examined one of the following questions regarding the ACA or one of its provisions: (1) did the ACA impact a racial/ethnic disparity in a pregnancy-related outcome or (2) did the impact of the ACA on a pregnancy-related outcome differ by race/ethnicity? The latter includes studies that used statistical inference methods (ie, estimation or hypothesis testing) to evaluate whether the impact of the ACA differed between racial/ethnic groups, but it also includes studies that estimated the impact of the ACA stratified by race/ethnicity, which allows only for descriptive comparisons of the stratified point estimates. Although the authors' primary interest lies with understanding the answer to question (1), they also included question (2) because differences in the impact of the ACA by race/ethnicity hold implications for the impact on racial/ethnic disparities.
Within the scope of pregnancy-related health outcomes, the authors considered contraception-related outcomes (eg, contraception use or choice), fertility-related outcomes (eg, live birth rate, unintended pregnancy, interpregnancy interval), pregnancy health indicators (eg, prenatal care utilization, pregnancy complications), birth outcomes (eg, preterm birth [PTB], low birthweight [LBW]), and postpartum outcomes (eg, maternal mortality).
Importantly, the authors included contraception-related and fertility-related outcomes because they provide information regarding a potential mechanism of the ACA. Differential impacts on these outcomes by race/ethnicity would alter the composition of pregnancies and births, which may subsequently influence the distribution of pregnancy health indicators, birth outcomes, and postpartum outcomes. That is, the ACA could influence racial disparities in pregnancy health, birth outcomes, and postpartum outcomes through compositional changes in who becomes pregnant and gives birth. Critically, however, this would not be a success for population health because it does not improve the health of anyone getting pregnant or giving birth. Rather, it removes higher or lower risk pregnancies from the population. Moreover, whether impacts on contraception-related or fertility-related outcomes are “good” depends on whether these changes align with contraceptive preferences and fertility or pregnancy desires, which are often unmeasured. Thus, the authors only used results regarding contraception-related and fertility-related outcomes to contextualize findings regarding pregnancy health indicators, birth outcomes, and postpartum health outcomes.
After removing duplicate studies, the authorship team reviewed all titles and abstract to determine which studies would undergo full review. In this process, 2 authors independently reviewed each title and abstract. The Materials and Methods section was also reviewed before full-text review to capture studies that evaluated a relevant research question as a secondary objective or robustness check. Next, members of the authorship team reviewed the full text of all studies retained to make a final determination for inclusion. Disagreements were resolved through group discussion. Finally, 1 author (C.L.M.-B.) reviewed the reference lists of all included studies for additional relevant work.
Data extraction
The authors extracted the following information from each included article: publication year, author(s), data source, study setting and population, methods (study design, analytic strategy), exposure(s) and outcome(s), and associational measures reported (eg, prevalence ratio, prevalence difference). Where possible, the authors report confidence limits as a measure of estimate precision. If neither a confidence interval nor a standard error was provided in the original article, the authors provide the P-value.
An association is reported if it is statistically significant at the 5% significance level. Acknowledging the arbitrary nature of this threshold, this strategy was chosen to systematically determine whether there was sufficient evidence of an association. Where an association was investigated, but sufficient evidence was not found, the authors report that “there was no association.” If an association was statistically significant at the 5%–10% significance level, the authors report that the association was “marginally significant.”
Results
Search results and study characteristics
The authors' search identified 5691 records through PubMed, WoS, and EconLit, and 788 records through references. After removing duplicates, n = 1517 unique articles were screened and n = 21 articles were retained for full review (Fig. 1 and Supplementary Appendix Tables C1–C4). Supplementary Appendix Tables C2–C4 provide a detailed presentation of the data extracted from each reviewed article. To ease the reader's navigation of Supplementary Appendix Tables C2–C4, in-text references to study author(s) and publication year (as shown in Supplementary Appendix Table C1) are used in place of AMA-style references.
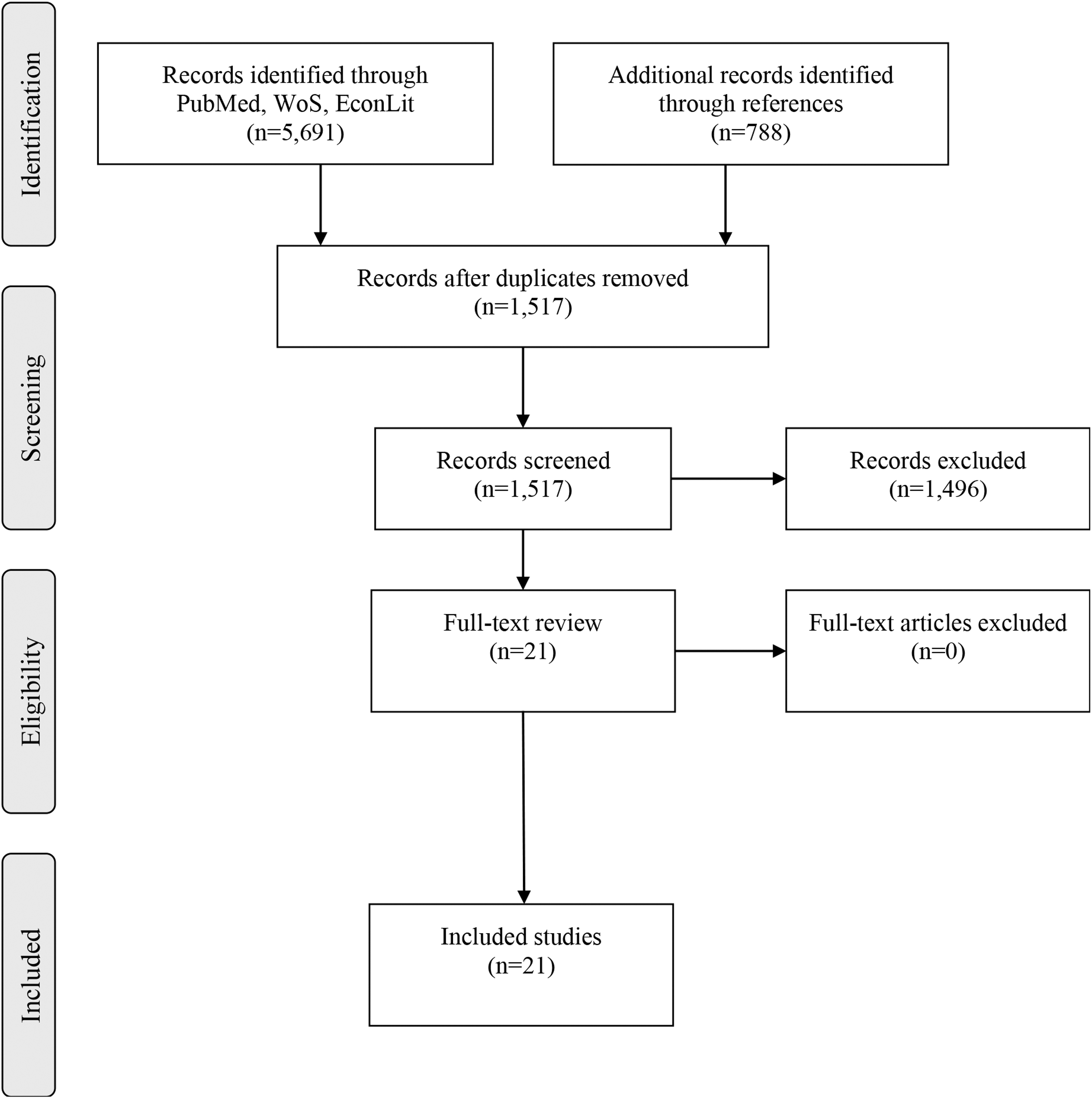
PRISMA flowchart.
Of the n = 21 reviewed articles, the majority (n = 12, 57%) evaluated the impact of Medicaid expansion (Table 1). The remaining articles evaluated the impact of the young adult-dependent coverage (YADC) provision (n = 4), the entire ACA (n = 2), the expansion of non-Medicaid subsidized insurance (n = 2), the opening of the Marketplace and the expansion of Medicaid (ie, the 2014 ACA insurance expansions) (n = 1), the contraceptive mandate (n = 1), or the Medicaid primary care rate increase (n = 1) (Table 1). Roughly 33% of the included studies focused on fertility-related outcomes (n = 7), whereas 29% focused on contraception-related outcomes (n = 6) or pregnancy health indicators (n = 6), 19% focused on postpartum outcomes (n = 4), and 14% focused on birth outcomes (n = 3) (Table 1).
Summary of Exposure–Outcome Combinations Investigated in Included Studies (n = 21)
Outcomes include contraception use or choice (n = 6), birth control counseling (n = 1), and checkup related to birth control (n = 1).
Outcomes include live birth rate (n = 1), birth in the past 12 months (n = 2), racial composition of live births (n = 2), unintended pregnancy (n = 1), and short interpregnancy interval or early postpartum pregnancy (n = 2).
Outcomes include prepregnancy diabetes (n = 1), prepregnancy hypertension (n = 1), prepregnancy smoking (n = 1), prenatal care initiated in the first trimester (n = 5), adequate prenatal care (n = 1), smoking during pregnancy (n = 2), gestational diabetes (n = 1), gestational hypertension (n = 1), infection during pregnancy (n = 1), anesthesia/neuraxial analgesia during labor (n = 2), and delivery by cesarean section (n = 1).
Outcomes include PTB (n = 3), VPTB (n = 1), gestational age (n = 1), LBW (n = 3), VLBW (n = 2), birthweight (n = 1), and NICU admission (n = 1).
Outcomes include severe maternal morbidity (n = 1), maternal mortality (n = 1), postpartum outpatient visits (n = 1), and postpartum checkup (n = 1).
This refers to Marketplace subsidies and other state-subsidized insurance plans that existed before the ACA.
ACA, Affordable Care Act; LBW, low birthweight; NICU, neonatal intensive care unit; PTB, preterm birth; VLBW, very low birthweight; VPTB, very preterm birth; YADC, young adult dependent coverage.
The remaining Results section and Discussion section are organized around these 5 outcome categories. Further, within these 5 outcome categories, results are organized by target population and exposure. By grouping results within target population, the authors highlight that the results of different studies may generalize to slightly different populations (eg, birthing people vs. low-income birthing people). Additional differences in study population are further presented in Supplementary Appendix Table C2.
All studies utilized a repeated cross-sectional design, and 52% of studies utilized birth certificate data (n = 11) (Table 2). Further, 62% (n = 13) of the included studies used a difference-in-differences (DD) approach, 24% (n = 5) used a pre/post analysis, 10% (n = 2) used an interrupted time series analysis, and 10% (n = 2) used a simulated eligibility analysis (Table 2). For reference, a brief description for each of these analytic strategies is provided in Supplementary Appendix Table C5.
Study Characteristics (n = 21)
Nine studies used NCHS natality files whereas 2 studies used birth certificate data from single states: (1) Oregon and (2) Arkansas.
All studies used a repeated cross-sectional design.
A point estimate was provided along with either a confidence interval, a standard error estimate, or a P-value.
HCUP, Healthcare Cost and Utilization Project; NCHS, National Center for Health Statistics; NH, non-Hispanic.
Nearly all included studies (n = 20) provided race- or ethnic-specific estimates of the association between exposure and outcome, but only 5 articles (24%) used statistical inference methods to estimate the difference in association between racial or ethnic groups. Across the reviewed studies, the number of included racial or ethnic groups ranged from 2 to 7. Studies most often included Hispanic (n = 17), NH Black (n = 16), and NH White (n = 16) racial or ethnic groups. Less often included were American Indian/Alaska Native groups (n = 3), Asian or Pacific Islander groups (n = 3), and Native Hawaiian or other Pacific Islander groups (n = 1). Occasionally studies included an aggregated group of “other” racial or ethnic identities (n = 5), but more often, people who did not identify with 1 of the included racial or ethnic groups were excluded (Table 2).
Contraception-related outcomes
Summary
Six studies considered contraception-related outcomes (Table 1). Across these studies, there was some suggestion that the impact of the 2014 insurance expansions, Medicaid expansion, and the YADC provision on contraception-related outcomes may have differed by race/ethnicity. 13 –15 This evidence is limited, however, to descriptive characterization because these studies did not use statistical inference methods to estimate the difference in impact between racial/ethnic groups. The 2 studies that did use statistical inference methods (to investigate the YADC provision) did not find statistically significant evidence of a difference in the association by race/ethnicity (Supplementary Appendix Table C4). 16,17
Contraception use or choice
Among females of reproductive age, the 2014 insurance expansions were associated with increased use of long-acting reversible contraceptives (LARCs) among Hispanic (15.5 percentage points [ppt]), NH Black (13.1 ppt), and NH White (13.8 ppt) females (Supplementary Appendix Table C3). 13 Further, this increase may be part of a shift in contraceptive choice, and this shift may have differed between groups (eg, a shift from non-LARC prescription contraceptives [−12.8 ppt] to LARCs [13.8 ppt] among NH White females vs. a shift from nonuse [−6.1 ppt], nonprescription contraceptives [−4.1 ppt], and non-LARC prescription contraceptives [−3.0 ppt] to LARCs [13.1 ppt] among NH Black females).
Among young adults aged 19–25 years, the YADC provision was associated with an increased use of prescription contraceptives among Hispanic females (13.5 ppt), but not NH Black or NH White females (Supplementary Appendix Table C3). 14 In addition, the ACA was not associated with dual-use contraception among young adult females aged 15–24 years (Hispanic, NH Black, or NH White), 17 and Medicaid expansion was not associated with the use of highly or moderately effective contraception among sexually active female adolescents (Asian, American Indian/Alaska Native, Black, Hispanic, NH Black, Native Hawaiian or other Pacific Islander, or NH White). 18
Postpartum contraception use
Among low-income birthing people (incomes ≤138% of the federal poverty level [FPL]), Medicaid expansion was associated with increased use of postpartum contraception among NH Black (6.9 ppt) and NH White individuals (4.1 ppt; this finding was marginally significant), but not among Hispanic individuals (Supplementary Appendix Table C3). 15 When broken down by type of contraceptive, findings further differed between groups. Among NH Black individuals, Medicaid expansion was associated with an increase in postpartum use of LARCs (10.4 ppt) and a decrease in postpartum use of short-acting contraceptives (−8.2 ppt) or sterilization (−5.0 ppt). Among NH White individuals, Medicaid expansion was associated with an increase in postpartum use of LARCs (6.2 ppt) and a decrease in postpartum use of nonprescription contraceptives (−5.7 ppt). No significant associations were found among Hispanic individuals.
Fertility-related outcomes
Summary
Seven studies evaluated fertility-related outcomes (Table 1). Across these studies, there was some evidence that the YADC provision differentially influenced live births, 19,20 and that Medicaid expansion differentially influenced both live births and interpregnancy interval, 21 –23 among different racial or ethnic groups. Moreover, findings regarding live births and interpregnancy interval differed between studies when the study population differed based on income and/or parity, suggesting these may be salient effect modifiers. This evidence is limited, however, to descriptive characterization because these studies did not use statistical inference methods to estimate the difference in the associations between racial/ethnic groups.
Live births and the racial/ethnic composition of live births
Among low-income females (incomes ≤138% of the FPL), Medicaid expansion was associated with a decreased probability of giving birth in the past 12 months among American Indian/Alaska Native (−2.8 ppt) and Hispanic females (−1.0 ppt), but not among Asian, NH Black, or NH White females (Supplementary Appendix Table C3). 21 Consistent with this, Medicaid expansion was also associated with a shift in the racial/ethnic composition of births to parous people of all income levels, with a 4 ppt reduction in the percentage of births to Hispanic individuals, but no significant change in other included groups (NH Black, NH Asian or Pacific Islander) (Supplementary Appendix Table C3). 22
Among nulliparous females, a 10 ppt increase in Medicaid eligibility was associated with increased birth rates among NH Black females aged 36–45 years (2.1%), NH White females aged 26–35 years (1.2%), and 20–25-year-old females who were identified as NH other (1.6%), but not among Hispanic females of any age group (Supplementary Appendix Table C3). 23 Increased eligibility for non-Medicaid subsidized insurance (NMSI; eg, Marketplace plans) was associated with similar increases in birth rates among nulliparous Hispanic females aged 26–35 years (1.3%) and 36–45 years (3.6%), nulliparous NH Black females aged 36–45 years (3.0%), and nulliparous NH White females aged 20–25 years (1.3%), 26–35 years (1.4%), and 36–45 years (2.4%). No association with NMSI eligibility and live birth rate was detected among nulliparous females who were identified as NH other. 23
Among young adults, the YADC provision was also associated with a shift in the racial composition of births, with a 1.4 ppt increase in the percentage of babies born to Black individuals and 1.5 ppt decrease in the percentage born to White individuals (Supplementary Appendix Table C3). 19 Further, the YADC provision was associated with a decreased probability of having a live birth in the past 12 months among NH White young adults (−1.1 ppt), but not among Hispanic or NH Black young adults (Supplementary Appendix Table C3). 20
Unintended pregnancy
Among sexually active females of reproductive age, there was no association between the ACA contraceptive mandate and unintended pregnancy among any racial/ethnic group considered (Hispanic, NH Black, NH White or other) (Supplementary Appendix Table C3). 24
Short interpregnancy interval
Among low-income birthing people (incomes ≤138% of the FPL), Medicaid expansion was associated with a decrease in the probability of having a pregnancy <6 months postpartum among NH Black individuals (−4.8 ppt) but not among Hispanic or NH White individuals (Supplementary Appendix Table C3). 15 Among parous birthing people of all income levels, however, Medicaid expansion was associated with an increased probability of having a pregnancy <12 months postpartum among Hispanic individuals (3.4 ppt) but not among people who identified as American Indian/Alaska Native, NH Asian or Pacific Islander, NH Black, NH White, or people identified as NH other (Supplementary Appendix Table C3). 22
Pregnancy health outcomes
Summary
Six studies evaluated pregnancy health indicators (Table 1). These studies suggested that some elements of the ACA may be differentially associated with pregnancy health indicators across racial/ethnic groups, but evidence is mixed. There is little evidence that Medicaid expansion or the YADC provision differentially affected the probability of initiating prenatal care in the first trimester (hereafter, “timely prenatal care”) by race/ethnicity. 16,25 –27
Evidence regarding pregnancy risk factors or complications was more mixed. Medicaid expansion was differentially associated with prepregnancy diabetes, with more benefit observed among the NH White group than among the Hispanic group. 25 Increased NMSI eligibility was differentially associated with gestational diabetes and smoking-related outcomes, but in opposite directions (regarding gestational diabetes, more benefit was observed among the Hispanic group than among the NH White group; regarding smoking-related outcomes, more benefit was observed among the NH White group than among the Hispanic or NH Black groups). 27
Finally, there was also mixed evidence regarding delivery-related care. Increased Medicaid eligibility was differentially associated with cesarean delivery (a larger increase was observed among the Hispanic group than among the NH White group), 27 but there was inconsistent evidence regarding the association between Medicaid expansion/eligibility and anesthesia use during labor (perhaps related to parity), 27,28 and there was no evidence that NMSI eligibility was differentially associated with either cesarean delivery or anesthesia use during labor among nulliparous females. 27
Prenatal care
The association between Medicaid expansion and timely prenatal care did not differ by race/ethnicity (Hispanic, NH Black, or NH White) (Supplementary Appendix Table C4). 25 Consistent with this, Medicaid expansion was also associated with an increased probability of timely prenatal care among both Hispanic (2.4 ppt) and NH (1.3 ppt) individuals, and an increased probability of receiving adequate prenatal care among both Hispanic (3.6 ppt) and non-Hispanic (2.6 ppt) individuals (Supplementary Appendix Table C3). 26
Among various subgroups of birthing people, results further suggested that the impact of ACA provisions on timely prenatal care did not differ by race/ethnicity. Among nulliparous females, neither the association between increased Medicaid eligibility and probability of timely prenatal care, nor the association between increased NMSI eligibility and probability of timely prenatal care, differed by race/ethnicity (Hispanic, NH Black, or NH White) (Supplementary Appendix Table C4). 27 Similarly, among young adults, the association between the YADC provision and timely prenatal care did not differ by race/ethnicity (Hispanic, NH Black, or NH White). 16 However, among Medicaid-covered birthing people, the ACA Medicaid primary care rate increase was associated with increased odds of timely prenatal care among NH Black individuals, but not among their Hispanic, NH White, or NH other counterparts (Supplementary Appendix Table C3). 29
Risk factors and complications during pregnancy
The association between Medicaid expansion and prepregnancy hypertension, cigarette use after the first trimester, or infection during pregnancy did not differ by race/ethnicity (Supplementary Appendix Table C4). 25 However, Medicaid expansion was more positively associated with prepregnancy diabetes (0.1 ppt) among Hispanic than among NH White birthing people, suggesting there may have been a slightly larger benefit among the NH White group (Supplementary Appendix Table C4). 25
Similarly, when limited to nulliparous females, the associations between Medicaid eligibility and gestational diabetes, gestational hypertension, prepregnancy smoking, and smoking in the third trimester did not differ by race/ethnicity (Supplementary Appendix Table C4). 27 There was, however, evidence among nulliparous females that increased NMSI eligibility had differential impacts by race/ethnicity, on outcomes of prepregnancy smoking, gestational diabetes, and third trimester smoking. 27 A 10 ppt increase in NMSI eligibility was associated with a larger decrease in prepregnancy smoking among NH White females (−0.60 ppt) than among Hispanic (−0.12 ppt) or NH Black (−0.12 ppt) females, and a larger decrease in third trimester smoking among NH White females (−0.38 ppt) than among Hispanic (−0.03 ppt) or NH Black (−0.09 ppt) females. However, a 10 ppt increase in NMSI eligibility was also associated with a larger decrease in gestational diabetes among Hispanic females (−0.19 ppt) than among NH White females (−0.04 ppt) (Supplementary Appendix Tables C3–C4). 27
Delivery-related care
One study found no evidence that the association between Medicaid expansion and anesthesia use during labor differed by race/ethnicity (Hispanic, NH Black, NH White) among birthing people. 28 When limited to nulliparous females, however, increased Medicaid eligibility was associated with differential impacts on delivery-related care by race/ethnicity, and increased NMSI eligibility was not. Specifically, a 10 ppt increase in Medicaid eligibility among nulliparous females was associated with a larger increase in anesthesia use during labor among Hispanic females (0.62 ppt) and NH Black females (0.19 ppt) than among NH White females (−0.23 ppt) (Supplementary Appendix Tables C3–C4). 27 Similarly, a 10 ppt increase in Medicaid eligibility among nulliparous females was associated with a larger increase in probability of cesarean delivery among Hispanic females (0.51 ppt) than among NH White females (0.11 ppt) (Supplementary Appendix Tables C3–C4). 27
Birth outcomes
Summary
Three studies considered birth outcomes (Table 1) and evidence regarding differential impacts of the ACA by race/ethnicity were mixed. Among nulliparous females, an increase in Medicaid eligibility was not associated with differential impacts on birth outcomes (LBW, PTB, neonatal intensive care unit [NICU] admission) by race/ethnicity, but an increase in NMSI eligibility was associated with differential impacts that were supportive of health equity (larger decreases in LBW, PTB, and NICU admission among Hispanic females than among NH White females). 27
When not limited to nulliparous females, however, there was both evidence that Medicaid expansion differentially affected birth outcomes in an equitable direction (decreasing LBW, very low birthweight [VLBW], PTB, and VPTB more among NH Black birthing people than among NH White birthing people), 25 and evidence that Medicaid expansion differentially affected birth outcomes in an inequitable direction (decreasing PTB and LBW among White birthing people but not among Black birthing people). 30
PTB, LBW, or NICU admission
Medicaid expansion was associated with a slightly larger decrease in LBW (−0.5 ppt), VLBW (−0.1 ppt), PTB (−0.4 ppt), and VPTB (−0.1 ppt) among babies born to NH Black individuals compared with those born to NH White individuals (Supplementary Appendix Table C4). 25 In contrast with these results, another study found evidence that Medicaid expansion was associated with a decrease in PTB (−2.5 ppt decennial decrease) and LBW (−0.3 ppt decennial decrease) among White birthing people but was not associated with either outcome among Black birthing people (Supplementary Appendix Table C3). 30 Interestingly, this analysis also found that Medicaid expansion was associated with a decrease in VLBW among both Black (−0.3 ppt decennial decrease) and White (−0.1 ppt decennial decrease) birthing people (Supplementary Appendix Table C3). 30
When limited to nulliparous females, however, increased Medicaid eligibility was not differentially associated with LBW, PTB, or NICU admission by race/ethnicity (Hispanic, NH Black, or NH White) (Supplementary Appendix Table C4). 27 In contrast, increased NMSI eligibility was differentially associated with LBW, PTB, and NICU admission among nulliparous females. Specifically, a 10 ppt increase in NMSI eligibility was associated with a larger decrease in LBW among Hispanic females than among NH White females (Hispanic: −0.06 ppt vs. NH White: 0.08 ppt). A 10 ppt increase in NMSI eligibility was also associated with a larger decrease in PTB among Hispanic females (−0.11 ppt) and females identified as NH other (−0.09 ppt) compared with NH White females (0.10 ppt), and a larger decrease in NICU admission among Hispanic females (−0.11 ppt) compared with NH White females (0.10 ppt) (Supplementary Appendix Tables C3–C4). 27
Postpartum outcomes
Summary
Four studies evaluated postpartum outcomes (Table 1). There was descriptive evidence that the association between Medicaid expansion and maternal mortality or severe maternal morbidity may have differed by race/ethnicity with a more beneficial association observed in racially minoritized groups, thereby promoting racial health equity. 31,32 There was little evidence, however, that the impact of Medicaid expansion or the YADC provision on postpartum health care visits differed by race/ethnicity. 16,33
Maternal mortality and severe maternal morbidity
Medicaid expansion was associated with a decrease in the maternal mortality ratio among Hispanic birthing people (−6.0 deaths/100,000 live births), NH Black birthing people (−16.3 deaths/100,000 live births), and NH White birthing people (−3.7 deaths/100,00 live births, although this was only marginally significant) (Supplementary Appendix Table C3). 31 Further, among low-income birthing people in New York, Medicaid expansion was associated with a decrease in severe maternal morbidity among people who did not identify as NH White (Supplementary Appendix Table C3). 32
Postpartum health care visits
Medicaid expansion was associated with an increase in the number of outpatient visits in the first 6 months postpartum among both NH Black (0.9 visits) and NH White (1.1 visits) birthing people (Supplementary Appendix Table C3). 33 Among young adult birthing people, however, the YADC provision was not associated with an increased probability of receiving a postpartum checkup among any racial/ethnic group considered (Hispanic, NH Black, NH White). 16
Discussion
Summary of findings
Through searching PubMed, WoS, and EconLit, the authors identified n = 21 peer-reviewed articles that investigated the impact of the ACA or 1 of its components on racial/ethnic disparities in a pregnancy-related outcome [ie, fertility-related outcomes (n = 7), contraception-related outcomes (n = 6), pregnancy health indicators (n = 6), postpartum outcomes (n = 4), or birth outcomes (n = 3)]. Most of these studies (n = 17) used quasi-experimental methods such as DD, interrupted time series, or simulated eligibility.
The current literature suggests that the ACA 2014 insurance expansions, Medicaid expansion, and YADC provision were differentially associated with contraception-related outcomes and fertility-related outcomes by race/ethnicity. Differential impacts on contraception-related or fertility-related outcomes could translate into differential impacts on pregnancy health, birth outcomes, and postpartum outcomes by creating compositional changes in who is giving birth. Despite this, the current literature is quite limited (ie, sparse and inconsistent) regarding differential impacts of the ACA on pregnancy health and birth outcomes. Further, few studies have considered differential impacts of the ACA on postpartum outcomes. Among those that have, there is some suggestion that Medicaid expansion differentially affected maternal mortality and severe maternal morbidity, in the direction of racial health equity.
Importantly, the reviewed literature was relatively sparse for each outcome, with variation in target population and study design across studies. Differences in target population and study design may alter the magnitude of the expected association (eg, Medicaid expansion would be expected to have a larger effect among individuals with income ≤138% of the FPL than among individuals of all income levels), thereby limiting readers' ability to directly compare estimates across studies. For example, only 2 studies evaluated the impact of Medicaid expansion on short interpregnancy interval, and the target population differed between these 2 studies (ie, 1 focused on low-income birthing people while the other focused on parous birthing people of all income levels). Additionally, differences in target population are particularly important when considering the complex ways in which population-level interventions such as policy intersect with existing institutions and structures to differentially impact different subpopulations, 34 –36 as highlighted in Hypotheses 1 and 2 (Supplementary Appendix A).
Given the sparsity and inconsistency of the current literature, this scoping review indicates a need for additional research that identifies the causal impact of the ACA and its components on racial/ethnic disparities in pregnancy health, birth outcomes, and postpartum outcomes. More broadly, this review highlights the need for research examining impacts of federal health policy (and other public policies) on health to explicitly examine whether policy impacts are equitable across sociodemographic subgroups (eg, race, ethnicity, socioeconomic status). This work will be critically important for guiding future policy efforts to reduce racial/ethnic disparities in pregnancy-related health.
Limitations of the reviewed literature
Across the reviewed articles, 2 major limitations were consistently observed. First, many racial/ethnic groups were either not included or rarely included in the reviewed studies. Increasing inclusivity can be difficult because the data collection process often prohibits it, or the sample size of a given group may be too small to allow for inclusion in statistical modeling, 37,38 but a comprehensive understanding of the ACA's impact on racial/ethnic disparities requires inclusivity. Thus, disaggregating race and ethnicity to the extent that existing data allow is crucial. Further, to support health disparities research moving forward, public health advocates and policymakers should promote improved data collection regarding race/ethnicity—particularly in population-based surveys and vital records. 39,40
Second, less than a quarter of reviewed articles (n = 5) used statistical inference methods to estimate the difference in the ACA's impact between racial/ethnic groups, and none of the articles operationalized a disparity measure as the outcome. Most reviewed articles reported estimates of the policy's impact within each included racial/ethnic group, thereby facilitating only descriptive comparisons between groups. This limits the reader's ability to evaluate whether the policy's impact differed between racial/ethnic groups, thereby limiting their ability to draw conclusions regarding the policy impact on racial disparities in these health outcomes.
Strengths of the reviewed literature
The existing literature is strengthened by its use of quasi-experimental methods (ie, DD, interrupted time series, simulated eligibility approaches). Notably, however, this literature could be further strengthened by incorporating more transparent and robust discussion of the assumptions required by these methods to identify causal effect estimates (eg, the parallel trend assumption in the DD approach). The reviewed literature was also strengthened by its common use of population-based survey data or vital records that reduce risk of selection bias by providing a representative sample and measurement error by using standard procedures and validated measures in data collection. Even with validated measures, however, there is still the possibility of differential measurement error between demographic subgroups. 41
Limitations and strengths of the current review
This review is strengthened by the fact that the authors searched PubMed, WoS, and EconLit for relevant literature. Although this strategy excludes gray (nonpeer-reviewed, scholarly) literature, it facilitates reproducibility. Further, the search terms used in this review encapsulated all elements of the ACA and were not limited by disparity-related terminology (eg, disparity vs. inequity vs. inequality). The search strategy was further strengthened by including a review of the methods section before full-text review to identify studies that may have examined a relevant research question as a secondary analysis.
Conclusions
In summary, this scoping review found that the current literature suggests the ACA and its components were differentially associated with contraception-related and fertility-related outcomes by race/ethnicity. Despite the potential for these compositional effects to translate into differential associations with pregnancy health and birth outcomes, the literature is quite mixed regarding these outcomes. Additional work—particularly intersectional research that considers race, socioeconomic status, geography, 42,43 and nativity 44 —is needed to clarify the impact of the ACA and its components on racial/ethnic disparities in pregnancy health, birth outcomes, and postpartum health.
More broadly, given the profound and persistent racial/ethnic disparities observed in pregnancy-related health, the impact of federal policy on these disparities should be considered both during policy writing and following policy enactment. Research that examines whether the health impacts of federal policy are equitable may provide policymakers with the information necessary to better assess whether a proposed policy is likely to promote or diminish health equity. To promote racial equity in health, policy that is not necessarily equal in its impact, but is equitable in its impact, is needed. 45,46
Footnotes
Acknowledgments
The authors thank Timothy Michling for his assistance in running queries in PubMed, and Abraham Wheeler for his expertise and guidance to the authors as they developed the search strategy for this review.
Authors' Contributions
Dr. MacCallum-Bridges contributed to conceptualization, methodology, investigation, analysis, writing—original draft, writing—review and editing, project administration, supervision, and funding acquisition; Dr. Gartner, Dr. Hettinger, and Dr. Zamani-Hank were involved in methodology, investigation, and writing—review and editing; Dr. Margerison (senior author) was in charge of conceptualization, methodology, investigation, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under Award Numbers F31HD103404 (PI: Dr. MacCallum-Bridges) and R01HD095951 and R01HD095951-02S1 (PI: Dr. Margerison). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Funding sources were not involved in (1) study design; (2) collection, analysis, and interpretation of data; (3) writing of the article; or (4) the decision to submit for publication.
Supplementary Material
Supplementary Appendix A
Supplementary Appendix Table B1
Supplementary Appendix Table C1
Supplementary Appendix Table C2
Supplementary Appendix Table C3
Supplementary Appendix Table C4
Supplementary Appendix Table C5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.