
Abstract

Lung cancer is a major public health concern as the leading cause of cancer death in the United States, underscoring the urgent need for progress with early detection strategies. 1 Centralized and decentralized lung cancer screening (LCS) programs have emerged as two approaches along a continuum of strategies for the organization and implementation of LCS. Although both aim to detect lung cancer at its earliest stages, they differ in their administration, resource requirements, and impact on screening outcomes. However, gaps in knowledge remain, including a consensus definition for centralized screening and identification of the specific component(s) of the centralized process that most strongly drives improvements in screening outcomes. This editorial identifies several defining characteristics of centralized and decentralized programs, with a specific focus on the evidence demonstrating the benefits of centralized structures.
Centralized LCS programs are well-coordinated systems offering screening services in specialized centers, typically leveraging patient or nurse navigation to facilitate LCS. 2 In most cases, primary care providers (PCPs) or outside clinicians refer potentially eligible individuals, and program personnel (including nurses and coordinators) carry out all downstream screening-associated functions, thereby relieving overburdened PCPs of additional tasks. 3 These programs follow clinical practice guidelines and protocols to define patient eligibility for screening, provide consistently high-quality shared decision-making and low-dose computed tomography (LDCT) scans, and determine the management of screening-detected findings 4 (Fig. 1). Centralized programs typically involve multidisciplinary teams comprised of physicians and advanced practice providers from subspecialties including Pulmonary Medicine, Interventional Pulmonology, Thoracic Surgery, Thoracic Radiology, and Interventional Radiology. By pooling resources and coordinating expertise in lung nodule management, these programs can efficiently screen and manage large cohorts of high-risk individuals. 2
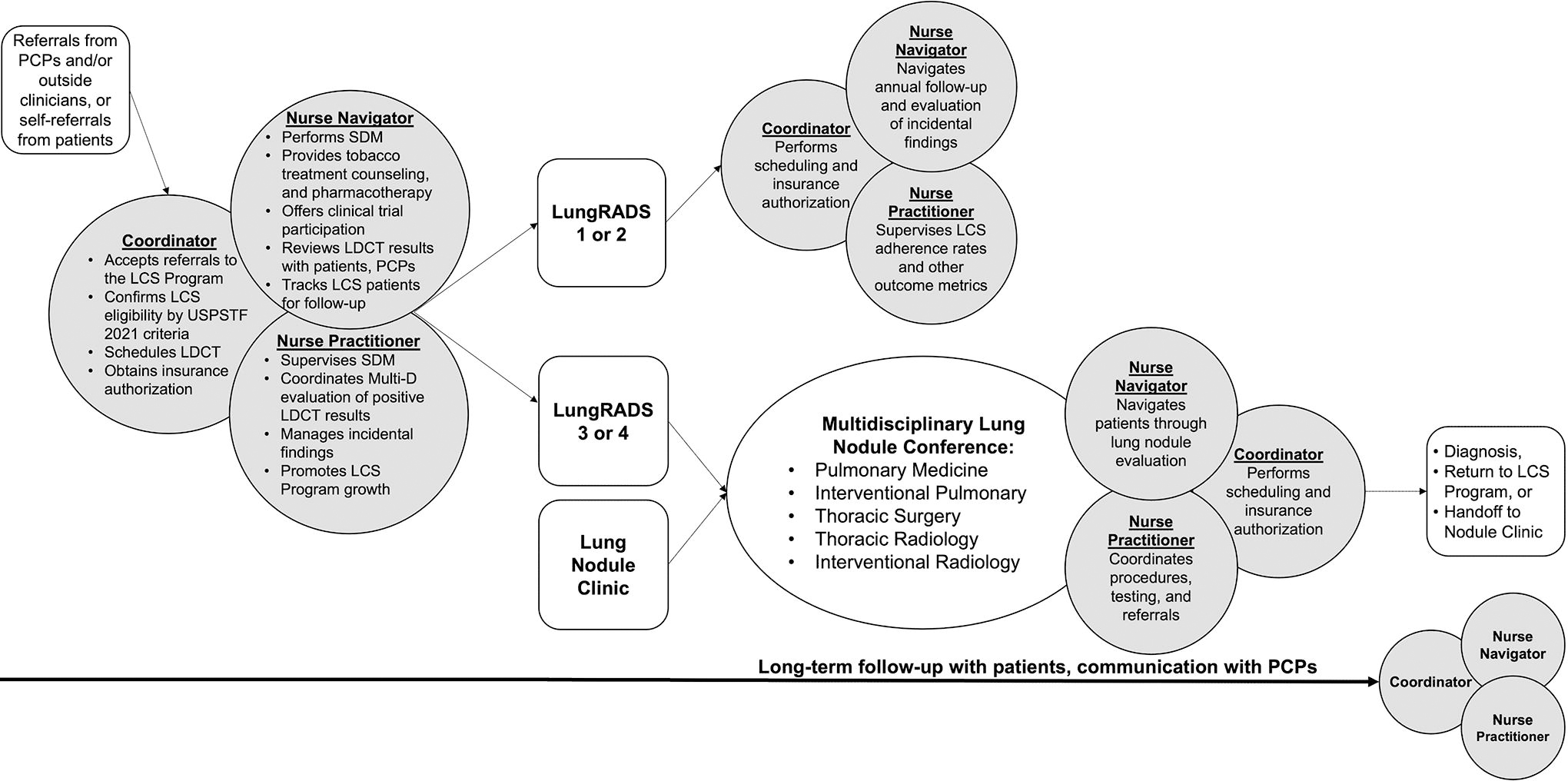
Centralized lung cancer screening program workflow at Thomas Jefferson University Hospital, Philadelphia, PA. CRNP, certified registered nurse practitioner; IP, inpatient; LDCT, low-dose computed tomography; SDM, shared decision-making; LCS, lung cancer screening; LungRADS, Lung CT screening reporting & data system; PCP, primary care provider; USPSTF, United States Preventative Services Taskforce.
One primary advantage of centralized programs is a standardized approach to providing high-quality LCS. This can help ensure that screening is appropriately offered to high-risk individuals who meet US Preventive Services Task Force criteria for eligibility and that patients return annually for continued screening, thereby optimizing the balance of benefits and harms of LCS. 2,5 In addition, robust staffing and navigation resources provided through a centralized program are critical for tracking patients, measuring screening outcomes, and maintaining communication with patients at critical steps throughout the screening process. Sakoda and colleagues showed that centralized programs can increase annual LCS adherence, therefore maximizing the known reduction in mortality that LCS provides. 6 Similarly, Kim and colleagues demonstrated in a multicenter cohort study that adherence to both annual LCS and recommended follow-up care was greater at centralized programs, particularly among Black individuals. 7 By concentrating efforts in dedicated centers, centralized programs can also leverage specialized management systems including registries and databases, skilled personnel, and multidisciplinary teams to provide comprehensive and evidence-based care. This approach has the potential to reduce variation in screening practices and facilitate accurate management of LCS results. Centralized programs also benefit from a centralized data infrastructure, enabling better tracking of screening outcomes and more timely workup of screen-detected abnormalities. 2
Despite many advantages, centralized programs require substantial investments in infrastructure, personnel training, and logistics, making their implementation and expansion challenging in resource-constrained settings. Therefore, centralized programs are found most often in academic medical centers, limiting their reach. Individuals from rural areas or regions with limited health care infrastructure may face difficulties accessing centralized centers.
In addition, while centralized programs have better outcomes with respect to patient adherence, it is unknown exactly which component(s) of centralized LCS drives this metric. Future research should investigate the impact of specific features of centralized LCS on adherence, such as program navigation, LCS provider-patient relationships, the multi-disciplinary approach, and well-coordinated follow-up and scheduling. Decentralized LCS providers could then incorporate the key driver(s) into their workflow to improve patient outcomes. 8 Centralized approaches may also be a mechanism to reduce racial disparities in screening. 7 In decentralized LCS, Black individuals with a negative baseline screen experienced a 27% decrease in annual screening adherence compared to their White counterparts, while there was no racial difference in adherence in centralized programs. 7 Black patients also have significantly greater lung cancer worries than White patients, while citing screening convenience and cost as very important factors much more frequently. Consideration of such factors in future research and LCS structure could be part of a more comprehensive approach to reducing racial disparities in LCS. 9
Conversely, decentralized LCS programs may allow greater access to screening across a broader network of health care facilities, including primary care clinics and community centers. In decentralized screening, PCPs screen eligible individuals directly, coordinating all steps of the LCS process. Decentralized LCS can increase access to early detection services for high-risk individuals who may face barriers in accessing centralized centers, such as those residing in rural areas or underserved urban locations. 8 This approach brings screening closer to local communities, promoting convenience, reducing travel distances, and potentially reducing health care disparities in access to care. Decentralized programs may also leverage existing health care infrastructure, minimizing the need for substantial additional investments.
However, decentralized programs may face challenges related to quality control and standardization of the LCS process. 10 It is also known that unnecessary LCS can carry significant harms, 3 and Smith and colleagues found that 90% of ineligible patients screened for lung cancer received LCS through decentralized programs. 10 In the context of a decentralized program, it is critical for PCPs to receive training to provide adequate counseling and shared decision-making. In addition, PCPs should have tools such as decision aids, information brochures, videos, and links to electronic resources. 6 PCPs must also have access to subspecialist experts who can manage screening-detected lung nodules. Such resources can help PCPs provide appropriate follow-up for not only suspicious lung nodules but also incidental findings, which are commonly identified in LDCT.
In summary, centralized and decentralized LCS programs represent two approaches to screening, each with benefits and challenges. Although centralized programs excel in providing standardized, comprehensive, and multidisciplinary care, decentralized programs allow for greater accessibility to screening in underserved areas. It is crucial to consider local patterns of care and target populations when deciding on the most appropriate screening strategy. A hybrid approach combining elements of centralized and decentralized programs may also be appropriate in some environments, optimizing resources and maximizing the potential benefits of LCS for diverse populations. 4 Such an approach often involves a centralized system for managing positive screening results while integrating decentralized screening services in local communities to enhance accessibility. Further research is needed to define clinically important screening outcomes by which LCS implementation strategies can be compared. Future research should also focus on examining secondary outcomes such as time to lung cancer diagnosis, tobacco treatment delivery and cessation rates, procedural complications, and appropriate follow-up of incidental findings, as well as patient-centered outcomes. 5 Ultimately a comprehensive LCS framework that maximizes early detection and reduces potential screening harms is needed to improve lung cancer mortality not only in the United States but also worldwide.
Footnotes
Authors’ Contributions
Jacob Martin led the original draft writing and investigation with supporting roles, while also equally contributing to the review and editing process. Gregory Kane equally conceptualized the project, provided supervision, and contributed to the review and editing of the writing. Christine Shusted contributed equally to the review and editing of the writing. Julie Barta equally conceptualized the project, led the investigation, provided supervision, led the visualization efforts, and contributed equally to the review and editing of the writing.
Author Disclosure Statement
J.A.B. reports research grants from the Prevent Cancer Foundation and the Genentech Health Equity Innovations Fund, and consulting fees for Delfi Diagnostics, Inc. paid to her institution, all outside the submitted work.
All other authors have no conflicts of interest to disclose.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.