
Abstract
The US health care system has significant room for growth to achieve the Quintuple Aim. Reforming the relationship between payers and providers is pivotal to enhancing value-based care (VBC). The Payvider model, a joint approach to care and coverage rooted in vertical integration, is a potential solution. The authors aimed to investigate academic medical institutions adopting this model, termed Academic Payviders. All Association of American Medical Colleges (AAMC)-member allopathic medical schools were evaluated to identify programs meeting the inclusion criteria of offering both medical care and insurance coverage to patients via partnership with a payer or ownership of, or by, a payer. Twenty-five Academic Payvider systems were identified from 171 total AAMC-member programs. Most programs were founded after 2009 (n = 20), utilized a provider-dominant structural model (n = 17), and offered health plans to patients via Medicare Advantage (n = 23). Passage of the Affordable Care Act, recent trends in health care consolidation, and increased political and financial prioritization of social determinants of health (SDOH) may help to explain the rise of this care and coverage model. The Academic Payvider movement could advance academic medicine toward greater acceptance of VBC via innovations in medical education, resource stewardship in residency, and the establishment of innovative leadership positions at the administrative level.
Introduction
The Triple Aim laid the groundwork for the pursuit of value in health care by emphasizing 3 fundamental objectives: improved patient experience, enhanced outcomes, and reduced cost. 1 As health care systems evolved, the Quadruple Aim incorporated the crucial element of clinician well-being, followed by the Quintuple Aim, which introduced health equity, acknowledging the importance of equitable access and outcomes for all patients. 2 –4
Despite the evolution of these aims, the US health care system continues to grapple with critical shortcomings. Compared to peer countries, life expectancy remains 5% lower, and chronic disease burden 50% higher. 5 The exorbitant health care expenditure in the United States, amounting to 18.3% of gross domestic product, or $4.3 trillion annually ($13,000 per capita), raises concerns about the sustainability and efficiency of the system. 6 Physician burnout remains pervasive across specialties, contributing to medical and surgical errors while compromising patient safety. 7,8 Furthermore, a multitude of disparities in social determinants of health (SDOH) were further exacerbated by the COVID pandemic, posing a significant threat to individual and population health. 9,10
In light of these challenges, there is an undeniable need for reformation of the relationship between health care payers and providers. The current climate between these 2 entities has often been characterized by antagonism, with differing opinions toward the responsibility for the issues plaguing US health care. 11,12 A pivotal aspect of achieving value-based care (VBC) involves a shift toward alternative reimbursement models that prioritize outcomes over volume with shared accountability for risk. 13
One potential solution to align the interests of payers and providers is vertical integration, a strategy that overcomes the conventional obstacles of transferring control between parties. 14 Vertical integration in health care calls for the alignment of overarching goals, as well as the creation of a modified leadership structure to prevent conflicts of interest. Research has indicated that vertically integrated health systems have excelled in-patient experience, satisfaction, and overall health care perception. 14 The emerging concept of the Payvider, a model rooted in vertical integration and the Quintuple Aim, offers a promising approach. 15 This structure can take various forms, with the partnership model of shared ownership considered the most effective. 15
Key components of the Payvider model include its organizational structure, fewer protracted price-based negotiations, and new metrics for success and performance evaluation. 15 Potential risks, however, include perverse incentivization to provide less care and maximize financial gain. Overcoming these risks necessitates a positive organizational culture, technological innovation, and data sharing to inform decisions. 15 Furthermore, while the Payvider model may reduce antagonism between payers and providers, it may also lead to greater locoregional health care monopolization, which can harm consumers. 16
Amidst the evolving landscape of health care delivery, a notable trend has emerged: academic health systems offering health plans in a Payvider model. 17 This article seeks to investigate and shed light on the phenomenon of Academic Payviders, a term coined to describe academic health systems that provide health plans to patients—distinct from employer-sponsored plans. The research aims to elucidate the extent of this trend, its predominant structural models, and potential differentiating factors in comparison to non-Academic Payvider systems or traditional, nonaligned payer–provider systems. Additionally, this study seeks to analyze how Academic Payviders may influence adherence to the Quintuple Aim and drive a cultural shift toward VBC in academic medicine.
Methods
Inclusion criteria
The study compiled a list of all member schools affiliated with the Association of American Medical Colleges (AAMC) (n = 171). Medical schools in Canada, Puerto Rico, and the US Territories were excluded, narrowing the focus exclusively to allopathic medical (MD) programs in all 50 United States and the District of Columbia.
Search process
The primary teaching hospital or health system affiliated with each remaining medical school (n = 154) was identified by referencing clinical affiliations listed on the respective school's official website. Subsequent selection refinement entailed the exclusion of programs that did not meet the following working definition of an academic medical center (AMC): an institution comprising a university, a medical school, and an integrated primary teaching hospital or health system (n = 41).
After each AMC was identified, each hospital or health system's website was manually searched to identify if the AMC provided health insurance plans to the public, thereby categorizing the enterprise as an “Academic Payvider” (n = 25). The provision or administration of employer-sponsored or group health plans did not count toward plans offered to the public, and as such, organizations that only provided these types of plans were excluded (n = 88). A visual summary of the search criteria and exclusion process can be found in Figure 1.
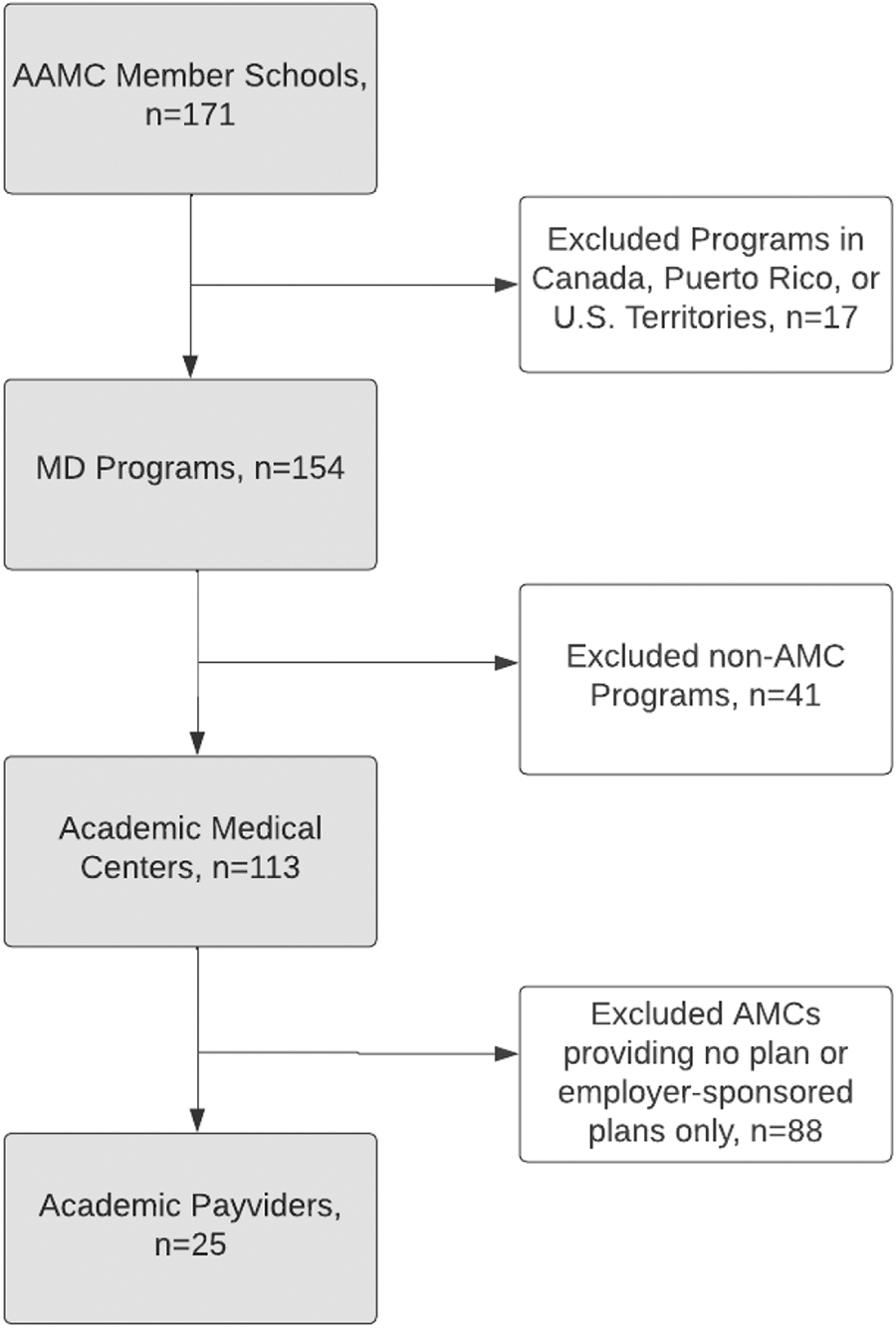
Search criteria and exclusion flowchart. AAMC, Association of American Medical Colleges; AMC, academic medical center.
Data analysis
Following the identification of Academic Payvider systems meeting criteria, data regarding the types of health insurance plans and member populations served were gathered from the respective health plan's enrollment website. The Payvider structure was classified into 3 models: provider-dominant, payer-dominant, or partnership, to understand the payer–provider relationship within each organization. 15 The entry of a provider into the health insurance market through the development or acquisition of a payer is known as a provider-dominant model. A payer-dominant model is 1 in which a payer enters the care delivery market by acquiring or developing a provider. The partnership model is 1 in which separate provider and payer entities partner to develop a Payvider. This data came from the Academic Payvider's website or supporting articles when primary sources were inadequate.
Results
Twenty-five Academic Payvider systems were identified. All were located in the contiguous United States and were concentrated along the East Coast and Central Northeastern regions (Table 1). There was a lack of programs found in the Midwest, West Coast, and Southeast. The density of Academic Payviders generally corresponds with trends in densities of US allopathic AMCs as listed by the AAMC. 18 The first Academic Payvider was established in 1995. Nineteen percent of Academic Payviders began offering plans between 1995 and 1998 (n = 5). Thirty-one percent started offering plans between 2009 and 2015 (n = 8), and 50% began 2017 or later (n = 12). The most common structural format was provider-dominant (n = 17), followed by partnership (n = 7), and payer-dominant (n = 1).
Index of All Academic Payvider Systems
BS&W, Baylor Scott & White; CHIP, Children's Health Insurance Program; DC, District of Columbia; EPO, Exclusive Provider Organization; HDHP, High-Deductible Health Plan; HMO, Health Maintenance Organization; HMO D-SNP, HMO Dual Eligible Special Needs Plan; HMO-POS, HMO Point of Service; LA, Los Angeles; MCO, Managed Care Organization; MVP; POS, Point of Service; PPO, Preferred Provider Organization; UMC, University Medical Center; UNC, University of North Carolina; UPMC, University of Pittsburgh Medical Center; VCU, Virginia Commonwealth University; WVU, West Virginia University.
Methods of coverage offered by Academic Payviders in 2023 were assessed to identify trends. The most common coverage offered included Health Maintenance Organization (n = 17) and Preferred Provider Organization (n = 15). No other method of coverage was offered by more than 5 Academic Payviders. The majority offered at least 2 or more coverage methods (n = 14). These offerings are likely to fluctuate in availability by year. Patient populations were also assessed based on the types of coverage for which they are eligible. The Medicare Advantage population was the most common group served by Academic Payviders via various Medicare Advantage plans (n = 23), followed by the Commercial (n = 12), Medicaid (n = 9), and Children's Health Insurance Program (n = 8) populations (Fig. 2). Additionally, all Academic Payviders that offered exclusively Medicare Advantage were established after 2008.

Populations served by Academic Payviders.
Discussion
The Academic Payvider movement
The authors identified rapid growth of Academic Payvider systems within the last 2 decades. This has been seen across several regions of the country, though such models remain concentrated in urban settings with higher population density and diversity. This trend may continue as policy and market forces encourage hospital systems to optimize financial stability and care quality.
Urban centers are likely to have increased competition; this pressure encourages systemic innovation. With increased racial diversity and low-income patients often requiring more provision of nonreimbursed services, there is often a greater focus on SDOH within these communities. 19 Additionally, there was an apparent lack of Academic Payvider implementation in the Southern United States, where there is less frequent state legislation to incentivize VBC. 20,21 As these models become more prevalent and their benefits and risks become more apparent, establishment of more systems across the country may occur.
The growth of Academic Payviders is stimulated by ongoing policy and market factors. Providers often have negative views of payers given regulatory burdens and administrative workload, often resulting in a confrontational or antagonistic relationship. 11,15 Additionally, many providers oppose VBC-associated elimination of fee-for-service (FFS) reimbursement without a model of stable salary-based income, and prefer that only bonuses be tied to outcomes. 11 AMCs have especially struggled to depart from a FFS system due to rigid clinical workflows and an absence of risk sharing between the health system, the providers it employs, and the payers in its network. 22 A potential solution rests in the Payvider model, which may promote greater sharing of risk and outcomes-based reward. 15 As competition and regulation rise, many provider systems have found that consolidation with insurers may control their revenue streams more consistently.
The Affordable Care Act and subsequent legislation have also created incentives and penalties for various quality metrics. For instance, hospitals were not reimbursed for treatment of near-term preventable, peri-hospitalization complications. 23 –25 Similarly, VBC was encouraged through incentivization of efficiency, waste reduction, and care coordination. 20,26,27 These factors make revenue less predictable for providers. Simultaneously, health systems have seen tightening budgets as reimbursements fall and inflation rises, only accelerated by the pandemic. As these pressures rise, hospital systems are seeking to synchronize cost and payment schema. The Academic Payvider model may allow greater insulation from losses caused by treating uninsured patients or addressing quality.
Ultimately, this shift in payment models can aid patients and providers alike. The patient experiences benefit from improved coordination and integration, reduced insurance hassles, and increased staff attention to ensuring optimal outcomes. Simultaneously, providers experience reduced administrative burden and burnout. For instance, much documentation, prior authorization, and disagreements with insurance controllers may be eliminated. More broadly, health equity may improve as Academic Payviders are incentivized to emphasize preventive and holistic care.
However, despite increases in efficiency and decreases in overhead expenses, consolidation (and subsequent monopolization) has produced uncontrolled increases in prices for consumers. As payers and providers integrate vertically and as hospitals integrate horizontally with individual physicians and care sites, there is increased incentive to refer patients internally and increase the volume of care provided to individual patients. 22 One study between 2007 and 2013 found that prices increased by 14.1% once systems acquired physician practices. 26 Nearly half of this increase was attributable to abuse of reimbursement regulations that allow “facility fees” for procedures performed by hospital-owned physician practices. 26 In turn, studies support the idea that providers, especially academic institutions, prioritize patients with commercial insurance, and commercial insurers subsequently transfer price increases to their members via higher premiums. 22,27 In terms of quality improvement, there has not been consistent evidence demonstrating improvement in cases of integration. 28
The academic cultural shift to value based care
For VBC to have a positive impact on the American health care system, there is a need for greater education and awareness among providers regarding its goals. There has historically been a lack of emphasis on VBC teaching at all levels of medical education. 29 –31 This is partly because of the significant variation in defining, measuring, and therefore teaching about value in health care. As all providers interact with academic systems during the most formative times of their training, implementing Academic Payvider schema at these levels may have positive downstream effects. Academic Payviders could foster a top–down approach to VBC education for medical students and resident physicians via integration of principles into existing curricula.
The most prominent efforts toward VBC education at different phases of medical training have come from the Choosing Wisely (CW) Campaign, which has produced positive results and provides a blueprint for VBC education through The STARS Program. 32 Many specialties have taken part in the CW campaign to produce evidence-based clinical guidelines that decrease wasteful utilization. 33,34 The inclusion of case-based learning and small group sessions can be an effective way to instill VBC concepts. 35 –37 When teaching students about the next best step in management, value metrics should be incorporated into the discussion.
The American College of Physicians' High Value Care curriculum helps train resident physicians to be good stewards of limited health care resources. 38 Other national initiatives from the Medicare Payment Advisory Commission and Accreditation Council for Graduate Medical Education provide additional guidance for teaching residents how to provide VBC. 39 This multipronged approach offers significant potential for reshaping the cultural landscape of academic medicine by fostering a value-conscious mindset from early phases of medical training.
At the faculty and administrative level, establishing a Chief Value Officer could be a practical step toward demonstrating a strong commitment to prioritizing value. This officer could foster a value-centric culture by leveraging health care data, utilizing clinical decision support, and initiating de-implementation interventions, which have been shown to reduce low-value care. 40 The growth of administrative positions including Vice Chair for Quality or Chief Population Health Officer, for example, certainly reflect the prioritization of these issues by the leadership of various payer and provider organizations. 41 These roles typically exist at both the departmental and enterprise levels to ensure a multitiered approach to quality and population health improvement. The authors hypothesize the development of value officers in Academic Payvider institutions could expand in a similar manner.
Integration of VBC principles into training and practice requires an emphasis on standardized value measurement strategies, administrative support, and national initiatives focused on normalizing the value officer position. Collectively, these strategies present a promising pathway to instill a top–down culture of VBC within Academic Payvider systems.
Strengths and limitations
This study is the first to introduce the Academic Payvider model in the context of the US health care landscape. Additionally, trends in structure, geographic distribution, member populations served, plans offered, and growth over time were also presented. To date, no peer-reviewed articles have been published about the Academic Payvider model. By focusing on the intersection of care and coverage within academic settings, this article addresses a relatively unexplored yet crucial aspect of health care reform.
However, several limitations remain. Twenty-five Academic Payviders were identified from 154 allopathic medical schools, representing a small sample by which to define and characterize. There is potential for selection bias as the study exclusively focuses on allopathic programs, and only those in the contiguous United States, Alaska, Hawaii, and the District of Columbia. This may not represent the entire spectrum of AMCs.
Information regarding populations served and plan types offered represent only a snapshot in time and may vary from year to year. In addition, the specific details about the size of health plans and their financial status are not publicly available, which makes it difficult to evaluate the financial well-being of these plans or analyze the connection between plan size and the patient population they serve. Many of the Academic Payviders were established after 2010, indicating that the model is relatively nascent. Therefore, the long-term impact and sustainability of these systems are not yet fully understood. Future research should investigate the specific governance structure and financial status of all systems in this model of care and coverage to determine their ability to drive greater adherence to the Quintuple Aim.
Conclusion
The Academic Payvider model has the potential to enhance the alignment of US health care with the Quintuple Aim. By integrating care and coverage, these systems are progressively influencing health care delivery. This strategic approach has the potential to enhance the patient experience while also tackling the issue of misaligned financial incentives between payers and providers. Academic Payviders stand at the unique intersection of health care delivery and education. By incorporating the principles of value-based care (VBC) into medical education, these institutions possess the capacity to foster a novel cohort of health care professionals who prioritize value in all aspects of practice. While the emergence of the Academic Payvider model is a direct response to the needs of stakeholders in the US health care landscape, its impact is still evolving.
Footnotes
Authors' Contributions
E.D.H.: Conceptualization, methodology, investigation, formal analysis, writing–original draft, project administration. Z.N.G.: Conceptualization, methodology, data curation, writing–original draft, project administration. Y.B.S.: Conceptualization, methodology, writing–original draft. A.S.K. and V.J.: Investigation, formal analysis, data curation, visualization, writing–original draft. D.B.N.: Conceptualization, methodology, writing–review and editing, supervision.
Author Disclosure Statement
All authors declare they have no conflicts of interest.
Funding Information
No funding was received for this article.