
Abstract
Hip and knee replacement have been marked by racial and ethnic disparities in both utilization and postoperative adverse events among Medicare beneficiaries, but limited knowledge exists regarding racial and ethnic differences in joint replacement care among Medicaid beneficiaries. To close this gap, this study used Medicaid claims in 2018 and described racial and ethnic differences in the utilization and postoperative adverse events of elective joint replacements among Medicaid beneficiaries. Among the 2,260,272 Medicaid beneficiaries, 5987 had an elective joint replacement in 2018. Asian (0.05%, 95% confidence interval [CI]: 0.03%–0.07%) and Hispanic beneficiaries (0.12%, 95% CI: 0.07%–0.18%) received joint replacements less frequently than American Indian and Alaska Native (0.41%, 95% CI: 0.27%–0.55%), Black (0.33%, 95% CI: 0.19%–0.48%), and White (0.37%, 95% CI: 0.25%–0.50%) beneficiaries. Black patients demonstrated the highest probability of 90-day emergency department visits (34.8%, 95% CI: 32.7%–37.0%) among all racial and ethnic groups and a higher probability of 90-day readmission (8.0%, 95% CI: 6.9%–9.0%) than Asian (3.4%, 95% CI: 0.7%–6.0%) and Hispanic patients (4.4%, 95% CI: 3.4%–5.3%). These findings indicate evident disparities in postoperative adverse events across racial and ethnic groups, with Black patients demonstrating the highest probability of 90-day emergency department visits. This study represents an initial exploration of the racial and ethnic differences in joint replacement care among Medicaid beneficiaries and lay the groundwork for further investigation into contributing factors of the observed disparities.
Introduction
Hip and knee replacements can enhance the quality of life for individuals grappling with severe osteoarthritis. However, in the United States, the surgery has been marked by stark racial and ethnic disparities in both its utilization and postoperative adverse events. Specifically, Black individuals are ∼30%–60% less likely to receive elective joint replacement compared with their White counterparts. 1 –4 This disparity extends into postoperative adverse events as well. Black patients face a higher likelihood of experiencing complications, which, in turn, leads to increased rates of emergency department visits and hospital readmissions within 90 days of the joint replacement surgery. 5,6 In addition, Black patients tend to experience more limited functional improvements during their postsurgery recovery period. 2,7
However, most prior research on racial and ethnic disparities in joint replacement care has focused on older adults aged 65 years or older enrolled in traditional Medicare. There is a relative lack of evidence regarding joint replacement care utilization and postoperative adverse events among Medicaid-only beneficiaries, particularly regarding variations across racial and ethnic groups. This knowledge gap is important because Medicaid beneficiaries, who often face socioeconomic disadvantages, also face challenges in accessing care, and even if they access care, they may still face difficulties in receiving high-quality care. 8,9 Furthermore, the fastest growing age group for joint replacement surgeries comprises individuals aged 45–64 years, 10,11 with 15% of adults in this age bracket enrolled in Medicaid in 2020. 12 In addition, the issues of racial and ethnic disparities are particularly pertinent to Medicaid beneficiaries, given that more than half (61%) of Medicaid beneficiaries identified themselves as Asian, Black, Hispanic, and other non-White racial or ethnic groups in 2018. 13
To bridge this gap in the literature, this study analyzed nationwide Medicaid claims data from 2018 to describe the utilization and postoperative adverse events of elective joint replacement among Medicaid beneficiaries by their racial and ethnic groups. In addition, the study stratified joint replacement utilization and postoperative adverse events by neighborhood income mix within each racial and ethnic group. This allowed authors to explore potential outcome variations within each racial and ethnic group, as individual socioeconomic status differences could introduce significant heterogeneity in outcomes.
This study marks an essential initial exploration of racial and ethnic disparities in the utilization and postoperative adverse events of elective joint replacement among Medicaid beneficiaries, laying the groundwork for future investigations into factors that contribute to disparities.
Materials and Methods
Data source
This study used the 2018 Transformed Medicaid Statistical Information System Analytic Files (TAF) to describe (1) the utilization of elective joint replacement among Medicaid enrollees and (2) the postoperative adverse events of Medicaid joint replacement patients. 14 TAF includes detailed enrollment and claims information from inpatient, residential, and outpatient settings for Medicaid beneficiaries enrolled in either fee-for-service or managed care plans.
Study population
The authors initially identified 88,619,609 Medicaid beneficiaries in the 2018 TAF dataset. Among them, only individuals between the ages 45 and 64 were included. Medical conditions that require joint replacement (eg, severe arthritis) are more common in people aged 45 years and older, 15,16 and joint replacement among people aged 65 years or older is likely to be covered by Medicare. Authors also limited the study population to those enrolled in Medicaid for at least 11 months in the year 2018 to reliably capture their utilization of joint replacement and postoperative adverse events, as well as to those enrolled in Medicaid for at least 11 months in each of the years 2016 and 2017 to assess each person's comorbidities at the beginning of 2018. In addition, the sample excluded beneficiaries from 3 states with TAF data quality problems, from 28 states with >10% missing race and ethnicity data, and beneficiaries categorized as Hawaiian/Pacific Islander, multiracial, or unknown race/ethnicity to avoid small sample sizes that would violate reporting guidelines.
The final sample included 2,260,272 Medicaid beneficiaries in 19 states (Alaska, California, Delaware, Idaho, Illinois, Maine, Montana, North Carolina, North Dakota, Nebraska, New Hampshire, New Mexico, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Virginia, and Washington), including 5987 beneficiaries who received joint replacements in 2018. See eFigure 1 in Supplementary Data S1 for further details about sample selection.
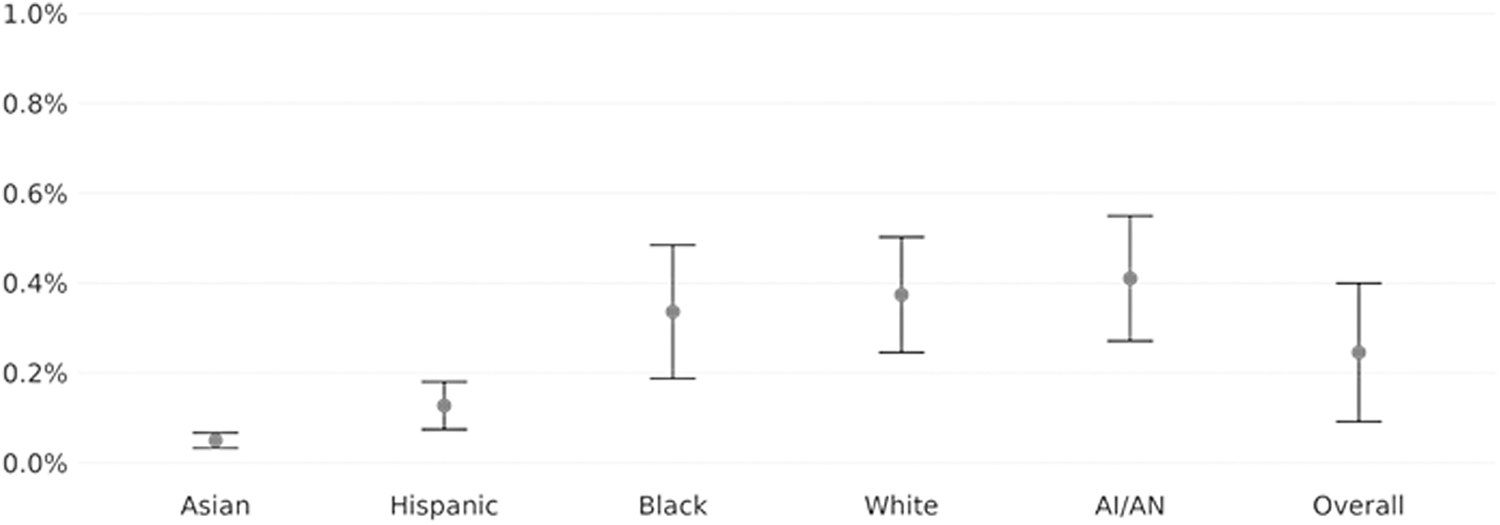
Elective joint replacement utilization among Medicaid beneficiaries by racial and ethnic groups in 2018, adjusted for sex and age. A vertical bar with whiskers is 95% CI of each estimate. AI/AN, American Indian/Alaska Native; CI, confidence interval.
Dependent variables
Dependent variables included (1) the utilization of elective joint replacements, (2) any 90-day all-cause emergency department visit, and (3) any 90-day all-cause readmission. The authors assessed the first dependent variable among all Medicaid beneficiaries, and the second and third dependent variables among beneficiaries who underwent elective joint replacements. To identify elective hip and knee replacements, the study used current procedural terminology (CPT) and International Classification of Diseases-10 codes from the Inpatient and Other Services TAF files (see eTable 1 in Supplementary Data S1). Authors used the 2016 Health Care Effectiveness Data and Information Set's Emergency Department Utilization measure, 17 which utilizes CPT codes, revenue codes, and place-of-service codes to identify emergency department visits, and used bill type codes to identify readmissions within 90 days after the joint replacement surgery (eTable 1 in Supplementary Data S1).
Characteristics of Medicaid Joint Replacement Patients by Their Racial and Ethnic Groups
Some cells coarsened to comply with reporting rules for small cell sizes. Type of bill codes, revenue center codes, and place of service codes were used to identify surgical settings. A weighted Charlson Comorbidity Index score was calculated using 2011 weights developed by Quan et al. 24 Claims from 2016 and 2017 were used to identify diagnoses of arthritis and obesity using the Chronic Conditions Warehouse 30 Chronic Conditions Algorithms. 40 To obtain measures of rurality, TAF data was linked by zip code to the 2010 Rural-Urban Commuting Area codes from the US Department of Agriculture.
AI/AN, American Indian/Alaska Native; SD, standard deviation; TAF, Transformed Medicaid Statistical Information System Analytic Files.
Race and ethnicity
The study used a race and ethnicity variable from the TAF that was constructed based on the most recent self-reported data available from the calendar year and the 2 preceding years. 18 This variable classified beneficiaries as Hispanic if they self-reported their ethnicity as Hispanic, regardless of their reported race. For all other cases, beneficiaries were categorized based on their reported race. To ensure adherence to reporting guidelines, the study excluded beneficiaries who were categorized as Hawaiians/Pacific Islanders, multiracial individuals, or those with unknown race/ethnicity, leaving the 5 categories: American Indian and Alaska Native, Asian, Black, Hispanic, and White.
Analysis
To describe the utilization of elective joint replacements, 90-day all-cause emergency department visits, and 90-day all-cause readmissions across racial and ethnic groups, authors estimated logistic regressions that accounted for race and ethnicity groups, as well as the beneficiary's age and sex. The model accounted only for age and sex in addition to race and ethnic categories because the differences in other individual factors (including health conditions) could be driven in part by structural racism and different life experiences lived by each racial and ethnic group. Authors wanted to capture racial and ethnic differences in the utilization and postoperative adverse events of joint replacement driven by such factors. Standard errors were clustered using the Huber-White method at the state level to account for repeated observations within each state. The adjusted marginal probabilities of each outcome were then calculated across 5 race and ethnicity groups, with the delta method to calculate standard errors.
Authors also described the utilization and postoperative adverse events of elective joint replacement within each beneficiary's race and ethnicity group in combination with the income mix of their residential zip code. To assess the neighborhood income mix, the study used the Index of Concentration in the Extremes (ICE) 19 –23 for income disparity, 21 which ranges from −1 to 1 (eSection 1 in Supplementary Data S1). Lower values of the ICE measure indicate zip codes primarily inhabited by low-income households earning <$25,000 annually, whereas higher values indicate zip codes predominantly inhabited by high-income households earning at least $100,000 annually. Middle range ICE values correspond to a more balanced mix of income. Authors categorized all zip codes into 3 groups based on the ICE measure values: [−1, −0.34), [−0.34, 0.34), and [0.34, 1].
Authors conducted separate sets of logistic regressions that included interaction terms between race and ethnicity groups and the 3 groups of zip codes based on ICE measures, while also adjusting for age and sex. Authors then calculated the adjusted marginal probability of each dependent variable for each of the 3 zip code groups within each race and ethnicity groups.
Three sensitivity analyses were conducted. First, authors expanded the study sample to those residing in 34 states with 0%–20% missing rates in the race/ethnicity data (instead of 19 states with 0%–10% missing rates) to increase the geographical scope of the study analyses. Second, authors adjusted for a wide set of covariates (rurality, Medicaid eligibility group including disabled adults, Medicaid expansion adults, other adults, pregnant women, or youth, 2-year weighted Charlson comorbidity index, 24 and history of arthritis or obesity) in addition to age and sex, and repeated the main analyses. Third, authors conducted a separate analysis for hip replacement and knee replacement.
All statistical tests were 2-sided, and statistical significance was set at a P-value <0.05. All analyses were conducted using R version 4.2.3. Institutional review board approval for this study was received from Oregon Health & Science University.
Results
In 2018, a total of 5987 Medicaid beneficiaries underwent joint replacement surgeries, representing 0.26% of all Medicaid beneficiaries between the ages of 45 and 65 years. These joint replacement patients had distinct characteristics within their racial and ethnic groups (Table 1). In particular, Asian patients were the oldest (with an average age of 58.6 years old compared with a maximum of 57.1 for other groups) and had the fewest comorbidities (as indicated by a mean Charlson comorbidity index score of 0.8, compared with a minimum of 1.1 in other groups; 16.7% had obesity, compared with at least 23.2% in other groups; and 80.8% had arthritis, compared with at least 82.7% in other groups). In addition, Asian patients were most likely to receive a surgery in outpatient settings (15.0%, compared with maximum 11.1% for other groups).
In contrast, American Indian/Alaska Native and Black joint replacement patients were least likely to receive a surgery in outpatient settings (8.6% and 8.1%, respectively, compared with at least 11.1% for all other groups). Black joint replacement patients had the highest Charlson comorbidity index score (1.6, compared to a maximum of 1.4 in other groups) and were notably less likely to live in the west region (19.9%, compared with 38.2% for White patients and at least 65.6% for all other racial/ethnic groups).
When adjusting for age and sex, authors observed variations in joint replacement utilization among different racial and ethnic groups. Asian beneficiaries had the lowest likelihood of receiving joint replacements (0.05%, 95% confidence interval [CI]: 0.03%–0.07%), followed by Hispanic beneficiaries (0.12%, 95% CI: 0.07%–0.18%) (Fig. 1). In contrast, joint replacement utilization was more prevalent among other groups, with no statistically significant differences among American Indian and Alaska Native (0.41%, 95% CI: 0.27%–0.55%), Black (0.33%, 95% CI: 0.19%–0.48%), and White (0.37%, 95% CI: 0.25%–0.50%) Medicaid beneficiaries.
After adjusting for age and sex, Black joint replacement patients had a higher probability of a 90-day emergency department visit (34.8%, 95% CI: 32.7%–37.0%), compared with White (27.8%, 95% CI: 26.0%–29.7%), Hispanic (25.6%, 95% CI: 22.7%–28.5%), and Asian patients (20.0%, 95% CI: 17.5%–22.5%) (Fig. 2). Black joint replacement patients had a higher probability of 90-day hospital readmission (8.0%, 95% CI: 6.9%–9.0%), compared with Hispanic (4.4%, 95% CI: 3.4%–5.3%) and Asian patients (3.4%, 95% CI: 0.7%–6.0%), but the difference was not statistically significant when compared with American Indian/Alaska Native (7.9%, 95% CI: 4.5%–11.3%) and White patients (6.6%, 95% CI: 5.6%–7.6%). Within each racial and ethnic group, the utilization and postoperative adverse events did not vary by neighborhood income mix (Figs. 3 and 4).

Prevalence of 90-day ED visits and 90-day hospital readmissions among Medicaid joint replacement patients by racial and ethnic groups in 2018, adjusted for sex and age. Horizontal bars with whiskers indicate 95% CIs. AI/AN, American Indian/Alaska Native; CI, confidence interval; ED, emergency department.
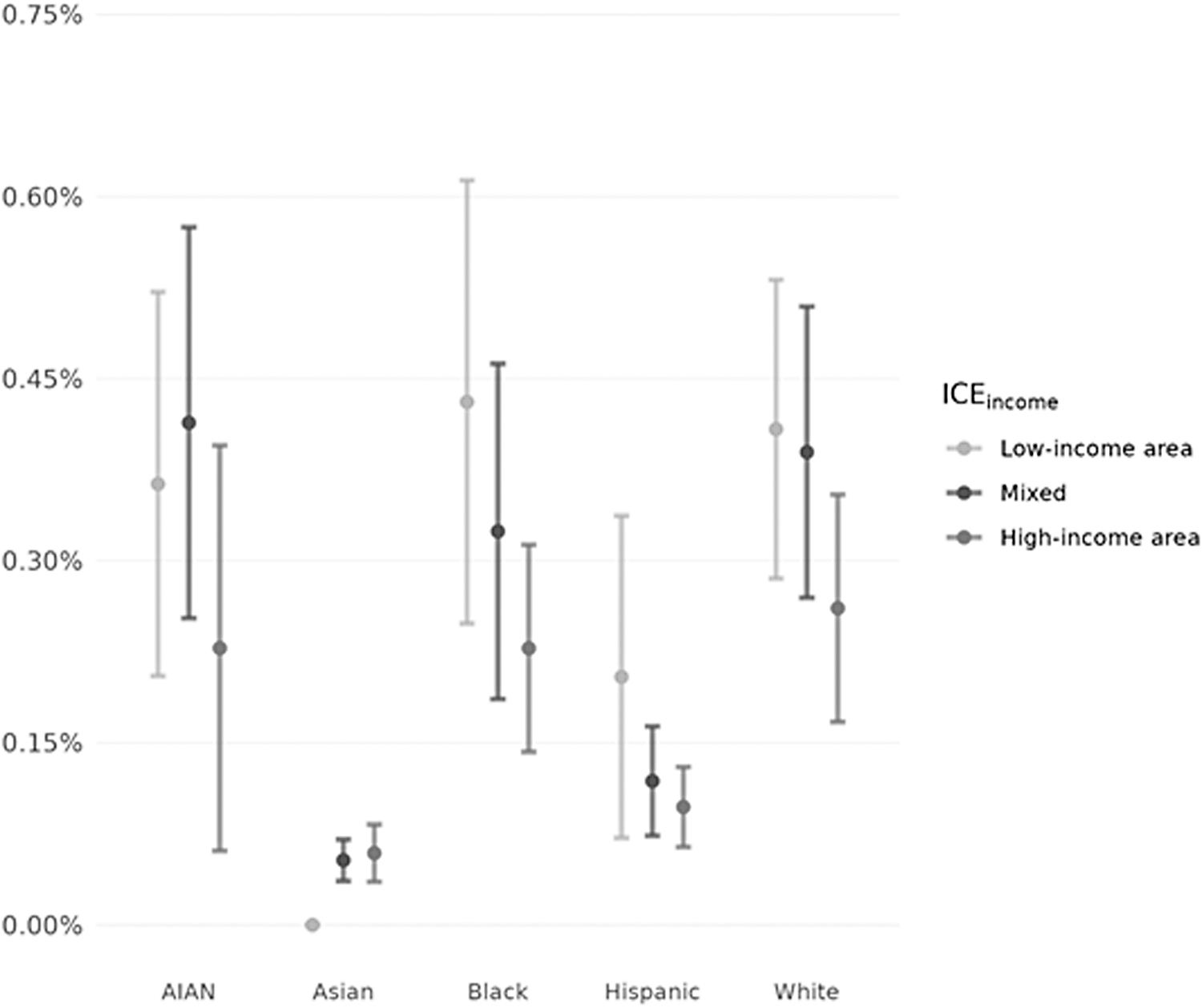
Elective joint replacement utilization among Medicaid beneficiaries by racial and ethnic groups and neighborhood income mix in 2018, adjusted for sex and age. Vertical bars with whiskers are 95% CIs. ICEincome is 3 groups of zip codes based on the ICE measures. Lower values of ICEincome indicate zip codes primarily inhabited by low-income households earning <$25,000 annually. In comparison, higher values indicate zip codes predominantly inhabited by high-income households earning at least $100,000 annually, with middle values corresponding to more balanced mixes of income. The CI for Asian beneficiaries living in low-income–dominated zip codes is not visible because none of the Asian beneficiaries living in low-income–dominated zip codes had a joint replacement and the CI was very narrow (0%–0.00002%). AI/AN, American Indian/Alaska Native; CI, confidence interval; ICE, Index of Concentration in the Extremes.
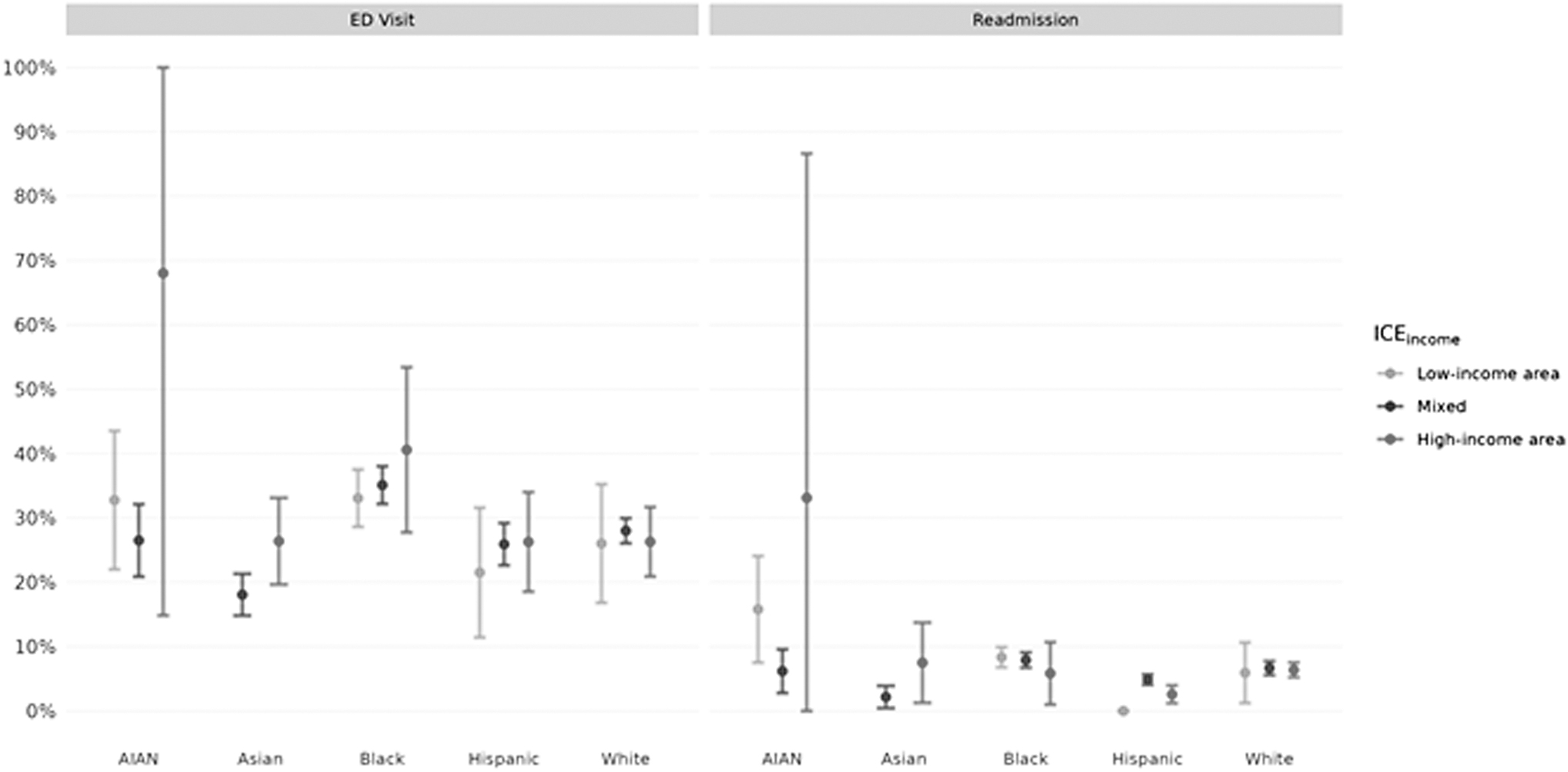
Prevalence of 90-day ED visits and 90-day hospital readmissions among Medicaid joint replacement patients by racial and ethnic groups and neighborhood income mix in 2018, adjusted for sex and age. Vertical bars with whiskers are 95% CIs. ICEincome is 3 groups of zip codes based on the ICE measures. Lower values of ICEincome indicate zip codes primarily inhabited by low-income households earning <$25,000 annually. In comparison, higher values indicate zip codes predominantly inhabited by high-income households earning at least $100,000 annually, with middle values corresponding to more balanced mixes of income. None of the Asian joint replacement patients resided in low-income–dominated zip codes, and therefore, estimates of ED visits and hospital readmissions were not presented for them. The CI for readmissions among Hispanic patients living in low-income–dominated zip codes is not visible because none of those patients had readmissions, and the CI was very narrow (0%–0.00001%). AI/AN, American Indian/Alaska Native; CI, confidence interval; ED, emergency department; ICE, Index of Concentration in the Extremes.
The results of the sensitivity analyses were similar to findings from the main analyses with one exception: the rate of emergency department visits did not differ across racial and ethnic groups when the sample was limited to hip replacement patients (eFigures 2–7 in Supplementary Data S1).
Discussion
Using 2018 nationwide Medicaid claims data, this study described the utilization and postoperative adverse events of elective joint replacements among Medicaid beneficiaries across racial and ethnic groups. The analysis yielded 3 findings: First, Asian and Hispanic beneficiaries received joint replacements less frequently than American Indian and Alaska Native, Black, and White beneficiaries, but the latter 3 groups showed similar utilization rates. Second, there were evident disparities in postoperative adverse events across racial and ethnic groups, with Black patients demonstrating the highest probability of 90-day emergency department visits. Third, within racial and ethnic groups, utilization and postoperative adverse events of elective joint replacement showed no significant variation by neighborhood income mix.
This study's analysis builds on previous studies that have consistently found a higher prevalence of 90-day emergency department visits and readmissions among Medicaid joint replacement patients than those with Medicare and commercial insurances. 25 –29 For example, using the 2013–2017 institutional database at a tertiary referral center, Plate et al found 21% and 10% of joint replacement patients with Medicaid coverage had 90-day emergency department visits and readmissions, respectively, which was higher than people with Medicare or other insurance coverage. 25 Another study using the 2013 nationwide readmission database found 10.0% of Medicaid joint replacement patients had 90-day readmissions, again higher than 7.4% among non-Medicaid patients. 26 As far as authors are aware, no studies have assessed utilization of elective joint replacement among Medicaid beneficiaries or racial and ethnic disparities in the utilization and postoperative adverse events of joint replacement among Medicaid beneficiaries.
In this study, elective joint replacement utilization did not significantly differ across American Indian/Alaska Natives, White, and Black beneficiaries. This finding is inconsistent with the consistent pattern found among older adults with Medicare coverage. In the Medicare population, racial and ethnic minority groups, particularly Black individuals, typically receive joint replacements at significantly lower rates than White individuals, and this disparity has persisted despite national efforts to mitigate it. 1 Although understanding the driving factors behind this stark disparity among Medicare beneficiaries remains a challenge, past studies suggest that a lack of trust in the health care system among racial and ethnic minorities often leads to reluctance to undergo joint replacement. 30,31 Given this, the current study finding that elective joint replacement utilization among Black Medicaid beneficiaries did not significantly differ from White beneficiaries is an encouraging outcome.
However, it is worth noting that the overall utilization of elective joint replacements among Medicaid enrollees was relatively rare. Specifically, only 2.6 of every 1000 Medicaid beneficiaries received an elective joint replacement, substantially lower than in previous studies for Medicare beneficiaries aged 65 years or older (13–15 of 1000 beneficiaries). 1,4 This may be because fewer Medicaid beneficiaries in the study sample required an elective joint replacement because of their younger age. Alternatively, this discrepancy may suggest that Medicaid beneficiaries, regardless of racial and ethnic group, face barriers to accessing elective joint replacement procedures. Supporting this assumption, a previous study conducted with a small sample in South Florida reported that only 14% Medicaid beneficiaries were offered an appointment for an elective joint surgery when contacting an orthopedic surgeon's office compared with 100% of beneficiaries with commercial insurance. Furthermore, those who were offered an appointment had to wait twice as long for their surgery compared with individuals with other insurance types. 32 Further research is needed to delve deeper into these factors.
This study found that postoperative adverse events were most common among Black joint replacement patients. Specifically, ∼35% of Black patients visited the emergency department within 90 days of surgery. This rate was also much higher than corresponding rates reported in previous studies, which typically range from 10% to 20%. 33 –35 This alarming discrepancy, predominantly observed in knee replacement patients, raises significant concerns, highlighting the need to understand underlying causes. One important factor may be the specific hospitals that Black replacement patients have access to for surgery. A previous study has shown that racial and ethnic minorities, including Black patients, often face barriers in accessing high-volume hospitals, 36 where a higher volume of joint replacement surgeries typically translates to fewer postoperative adverse events. 37 The type of postacute care Black patients receive may also matter.
The use of institutional postacute care after joint replacement surgeries is associated with increased postoperative adverse events, 38 and studies have reported that Black joint replacement patients are much more likely to be discharged to institutional postacute care as opposed to home to recover. It is possible that social determinants of health (SDOH), such as socioeconomic status or social support, may inform the decision of discharge location, in turn influencing postoperative adverse events. To ensure equitable care, future studies are needed to assess the reasons behind why Black joint replacement patients experience such elevated rates of postoperative adverse events, including SDOH that may determine access to high-quality care.
This study found that the utilization and postoperative adverse events of elective joint replacement did not vary by neighborhood income mix within each racial and ethnic group. This suggests that individual socioeconomic status differences within these groups measured by where people lived may not be contributing to heterogeneity in joint replacement care. This finding was surprising because prior studies have reported that residents in areas mainly resided by low-income households often experience more disparities, such as higher rates of infant mortality, 39 preterm birth, 19 fatal and nonfatal assaults, 21 compared with those in other areas. This unexpected finding may be because Medicaid beneficiaries shared similar socioeconomic status, regardless of the neighborhoods they resided in. It is also important to note that the 95% CIs were quite wide for some outcomes, which implies that authors may not be able to rule out meaningful differences among beneficiaries residing in areas with different income mixes.
This study has limitations. First, the study only included 19 states owing to data quality, limiting the generalizability of the study findings. However, the overall results remained consistent in the sensitivity analysis where the state exclusion criteria were relaxed to include 34 states with up to 20% missing race and ethnicity data. Second, the study used claims data and could not measure key factors related to quality of care, such as waiting time for surgery, functional improvements, or patient satisfaction. Third, the racial and ethnic differences that authors observed in utilization and postoperative adverse events of elective joint replacement may be owing to differences in underlying health conditions. Nevertheless, the sensitivity analyses in which authors accounted for some aspects of underlying health yielded similar results. Fourth, the study data are from 2018, predating the COVID-19 pandemic, and racial and ethnic differences in utilization and postoperative adverse events of joint replacement may have evolved during and after the pandemic.
In summary, Asian and Hispanic beneficiaries received joint replacements less frequently than American Indian and Alaska Native, Black, and White beneficiaries, with the latter 3 groups showing similar utilization rates. Furthermore, there were evident disparities in postoperative adverse events across racial and ethnic groups, with Black patients demonstrating the highest probability of 90-day emergency department visits. This finding underscores the pressing need for an in-depth investigation into the contributing factors, including SDOH, behind these disparities.
In conclusion, this study represents an initial exploration of the racial and ethnic disparities in joint replacement care among Medicaid beneficiaries, paving the way for further research aimed at understanding the underlying factors responsible for these disparities.
Footnotes
Authors' Contributions
Dr. Kim: conceptualization, methodology, writing—original draft, writing—review and editing, visualization, supervision, project administration, funding acquisition. Mr. Hart: conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, visualization. Dr. Senders: conceptualization, methodology, formal analysis, writing—review and editing, visualization. Dr. Schabel: conceptualization, methodology, writing—review and editing, visualization. Dr. Ibrahim: conceptualization, methodology, writing—review and editing, visualization, supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Agency for Healthcare Research and Quality (R01HS026457). The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.