
Abstract
In the aftermath of the US withdrawal from Afghanistan, over 100,000 individuals were evacuated to the United States, primarily arriving through Philadelphia International Airport and Dulles International Airport under Operation Allies Welcome. In Philadelphia, evacuees were greeted at the airport by a medical triage unit (MTU) that was rapidly assembled to provide on-site medical care. The MTU triaged emergent medical complaints, handled minor complaints on-site to reduce impact on local health care systems, distributed patients who did require a higher level of care among area hospitals, and ensured appropriate follow-up care for individuals with ongoing needs. Although there are regional and federal entities whose purview is the establishment and coordination of such responses, these entities were not mobilized to respond immediately when planes began to arrive carrying the first wave of evacuees as this event was not a designated disaster. The MTU was a grassroots effort initiated by local health care providers in coordination with the local Medical Reserve Corps and Department of Public Health. This article presents a framework for similar operations, anticipating an ongoing need for planning for sudden arrivals of large numbers of displaced persons, particularly via air travel, in a time of increasing mass displacement events, as well as a rationale for establishing more robust networks of local medical professionals willing to respond in the case of an emergency and involving them in the emergency planning processes to ensure preexisting protocols are practical.
Background
In August 2021, the United States completed its strategic withdrawal from Afghanistan, evacuating over 100,000 men, women, and children from Kabul. From August 2021 to March 2022, 29,713 evacuees from Afghanistan were processed through Philadelphia International Airport (PHL) before being transported to various military bases for resettlement at sites throughout the United States. 1
A core group of locally based emergency medicine physicians, in coordination with the Philadelphia Department of Public Health (PDPH) and the Medical Reserve Corps (MRC), recruited and formed a multidisciplinary team of physicians, nurses, and advanced practice providers from several area hospitals and rapidly established a medical triage unit (MTU) on-site at PHL in the baggage claim of Terminal A to provide medical attention to evacuees. 2 Volunteer leadership organized themselves into a command structure according to National Response Framework principles, 3,4 with individuals assuming the roles of incident command, logistical support, and operations leads. PDPH served as a local convener for the medical response and provided administrative and logistical support, as well as acquisition of the majority of the supplies needed for the MTU. The MRC helped to ensure volunteers were appropriately licensed to practice in Pennsylvania and registered with the city, as the majority were not already MRC registered—nationally, there are only about 15,000 physicians registered with MRCs, comprising 7.5% of their total volunteer pool. 5 Spontaneous volunteers are a common occurrence in disaster management and were a feature of Operation Allies Welcome (OAW) as well, but most disaster responses are not structured to incorporate them effectively and safely. 6 Registration with the MRC provided necessary structure for the inclusion of medical providers.
Although the operation to absorb and resettle evacuees was led by the Department of Homeland Security (DHS) with involvement from numerous other federal agencies, including the Department of Defense, the Federal Emergency Management Agency (FEMA), the National Guard, and Health and Human Services (HHS), the arrival of the evacuees was not a designated disaster, limiting the medical resources that were invoked to address it, and did not include a plan for on-site medical care. Medical resources at the federal level were focused on providing emergency health insurance coverage 7 and providing care at the military bases serving as temporary homes for evacuees, as well as ensuring that individuals were able to complete required medical exams and receive necessary vaccines to continue their visa applications. 8 Although these are critical functions in the care of refugees, they did not address acute needs at the point of entry or the prevention of overburdening of local health care systems.
The Department of Health and Human Services (HHS) Administration for Strategic Preparedness and Response’s (ASPR) Hospital Preparedness Plan (HPP) provides resources and funding for cooperative agreements between hospitals responding to large-scale disasters, particularly through the development of health care coalitions (HCCs), which are essentially mutual aid agreements between hospitals and other local health care entities (e.g., public health departments, EMS providers) to ensure that resources are available to each participating entity in the event of a disaster. 9,10 The COVID-19 pandemic highlighted significant weaknesses in these collaborative agreements and their practical utility in the event of a sudden need for resource deployment 11 as they are not structured or empowered to effectively engage local health care workers. 12 –14 In this case, ASPR and FEMA and the areas’ HCC were involved in OAW, particularly in the care of hospitalized patients, but did not take lead roles in the MTU as OAW was not designated as a disaster event.
Seventeen months into the COVID-19 pandemic and amid historic emergency department waiting room volumes and long boarding times at hospitals across the country and within Philadelphia, the MTU strategy for triaging, evaluating, and treating arrivals on-site was critical to avoid further stress on existing health care infrastructure, an issue that hindered the successful processing of evacuees at Dulles International Airport and that may have ultimately contributed to suspension of operations at Dulles. 15 The MTU provided efficient and trauma informed care on-site in order to mitigate impact on the local health system, quickly identify and communicate information on communicable diseases of public health concern, and facilitate safe transitions in care when indicated.
Since OAW concluded, the conflict in Ukraine has led to 4 million refugees fleeing the country, with flights bringing large numbers of refugees to international airports, 16 many of which have little warning of their arrival and no plan for the triage and care of arriving migrants, leading to prolonged lengths of stay in makeshift, unsafe housing situations on-site. 17 The Council of Europe has previously acknowledged the need for comprehensive planning for reception of refugees arriving by air, but no definitive or standardized protocol exists for providing medical care on-site. 18
The authors have therefore outlined their own approach to medical evaluation of evacuees on-site at a commercial airport during OAW as a framework for similar operations in the future. The success of the MTU outlined in this article highlights the critical need for involvement of local health care providers and systems leaders in the planning process for unconventional response needs at the local, regional, and federal level and for better coordination between the governmental agencies responsible for disaster response and the individuals tasked with caring for patients on the front line. These types of responses are becoming more frequent and preparing for them well has never been more urgent. The DHS Office of Health Security has taken the lead in providing more structure to these types of considerations for better future coordination.
Purpose
This operational framework outlines the processes related to the triage, transfer, and continuation of care for refugees arriving by air and is based on operations conducted during OAW. Given the structural similarities between many international airports and customs and immigration processes, this framework is applicable to future deployments for reception of refugees arriving by air in unpredictable medical condition. A MTU operating at an international airport must also account for the difficulties specific to the operating site, specifically coordination with existing airport medical resources and ensuring the security of the site as it continues to operate as a commercial airport.
The primary goals of the MTU were to: Ensure any patients with emergent issues were appropriately triaged and sent to local hospitals for further evaluation and management. Identify patients requiring specific follow-up and ensure appropriate onward placement aligned with their medical needs as they were routed through the resettlement process. Reduce the impact on local health care systems by managing minor, nonemergent complaints onsite, initiating more complex evaluations to reduce patient time off-site, and serving as a centralized command and transfer center to equitably distribute patients to local hospitals depending on capacity and facilitate their eventual return to the resettlement process. Ensure patients on chronic medications for high-risk conditions had adequate near-term supplies of needed medications. Ensure appropriate isolation of patients with infectious diseases of public health concern, including measles, mumps, tuberculosis, diarrheal illnesses, COVID-19, and other communicable diseases. Ensure that the care provided was culturally appropriate and trauma informed, making efforts to ensure that medical care did not further traumatize an already highly vulnerable population.
To achieve these goals, the authors have outlined the following framework for medical triage and assessment of large numbers of displaced persons during processing through an international airport.
Pre-Event Planning
Any municipality with a major receiving airport may at some point be called upon to receive a large number of refugees. In the case of OAW, the Philadelphia Department of Public Health was notified approximately 48 hours prior to the first arrivals, providing an extremely short window to stand up operations and recruit volunteers. This window of time was used to accomplish a number of tasks that could have been prepared before the onset of operations but, in this case, were accomplished in the 48 hours given before the first evacuees arrived (Table 1).
Pre-event Planning Before Event Occurrence or Notification
These pre-event tasks could be managed by the relevant emergency operations infrastructure and the health department, working in partnership with physician leaders and local health systems who are willing to assist in case of an emergency. Preemptively establishing these relationships and protocols may save valuable time and prevent confusion during an emergency.
When activated to respond, the focus of all involved parties can then pivot rapidly to establishing the appropriate medical command structure to lead the medical response and meet the specific needs of the arriving population (Table 2). The operation to receive and resettle Afghan evacuees was complex and involved numerous governmental and nongovernmental organizations. With so many parties involved, it was critical to have clear operational chains of command established, with a single point of command for the MTU. Designating a medical command team of several individuals who could rotate shifts, rather than a single individual, helped to ensure a core team leader was always available to direct the medical effort for consistency and sustainability. All members of this team met regularly with other leaders of the overall response effort to ensure communication between partners.
Pre-event Planning for a Specific or Known Refugee Arrival Event
Clinical Care Delivery
The MTU served several critical functions during OWA. Medical operations were guided by best practices regarding medical care of refugees
19
and focused primarily on: Appropriate identification of evacuees experiencing a medical emergency and requiring transport to a hospital for a higher level of care. Evaluation and resolution of minor medical issues that did not require hospital level care or specific follow-up. Identification of individuals requiring ongoing outpatient care or specific follow-up. Identification of individuals with infectious diseases of public health concern requiring immediate isolation and further management planning.
On-site operations
Staffing and organization
The medical commander was the main point of contact and a member of the medical command team was available 24/7 for coordination and questions for medical staff, as well as to rapidly manage and initiate new protocols for unanticipated events. This dedicated core team was responsible for coordinating with incident command and the other agencies participating in the response, including DHS as the overall OAW response lead, Transportation and Security Administration (TSA) as the OAW Philadelphia site leader, PDPH as the on-site medical response leader in coordination with the MRC, and other partners including the Department of Defense, Department of State, FEMA, and government contractors providing translation services.
Every shift had a designated medical lead physician. This individual provided rapid just-in-time training and orientation to medical staff at the start of each shift, organized and directed volunteers during the shift, and communicated any emergencies or needs to the medical command phone. The lead physician was also responsible for the initial triage of any patient arriving in the medical triage area, in order to direct the patient to an appropriately specialized clinician to address their chief complaint. The lead physician coordinated hospital transfers in conjunction with operations staff. Warm handoff was given at the end of each shift to the oncoming lead physician with particular attention to current hospital transfers and any changes to protocol necessary during the previous shift.
Medical care was primarily provided by volunteer physicians recruited from and representing a broad cross section of the health care systems of Philadelphia. A smaller number were recruited from nongovernmental organizations. Physician volunteers were selected based on specialty, with priority given to adult providers with training in a generalist specialty (e.g., emergency medicine, internal medicine, and family medicine) to maximize their ability to evaluate patients for a variety of complaints, and pediatric providers with a similar ability to evaluate a broad range of pediatric illnesses (e.g., pediatric emergency medicine, general pediatrics, and family medicine). Prior studies have shown that the majority of individuals arriving in a mass refugee event suffer from respiratory, dental, skin, and gastrointestinal illnesses, with a significant number having experienced trauma; medical providers on hand were preferentially those trained to handle this broad range of conditions. 20,21 OB-GYN trained providers were also highly valuable in this setting as pregnant women made up a significant proportion of evacuees, but were never the only adult providers available. Emergency medicine and family medicine providers are the ideal candidates to draw volunteers from given their diverse skill sets and ability to care for individuals across all ages and genders.
Translators were available for all medical evaluations as many evacuees did not speak English as a primary language, and patient outcomes are improved when medical care is provided in their preferred language, even if they speak English as a second language. 22 Translation services may be provided by governmental partners, contractors, or remotely via a phone translator service; for OAW a contractor provided the majority of medical translators after an initial period in which the team relied on the large numbers of volunteer interpreters from the local community.
Logistics
The layout of the medical triage area was arranged to accomplish several key goals: Initial triage by the medical team lead and direction of patients to an appropriate available medical provider for evaluation Smooth patient flow through the medical triage area and onward to the next step in processing Allow for family groups to remain together throughout the medical evaluation process Isolation of patients with potentially communicable diseases Privacy for physical exams, diagnostic testing, and procedures when needed
The medical command team coordinated with airport staff to identify an appropriate area with sufficient space for an MTU and to acquire necessary supplies to set up the area. Baggage claims are ideal for this purpose and were used during OAW (Fig. 1).
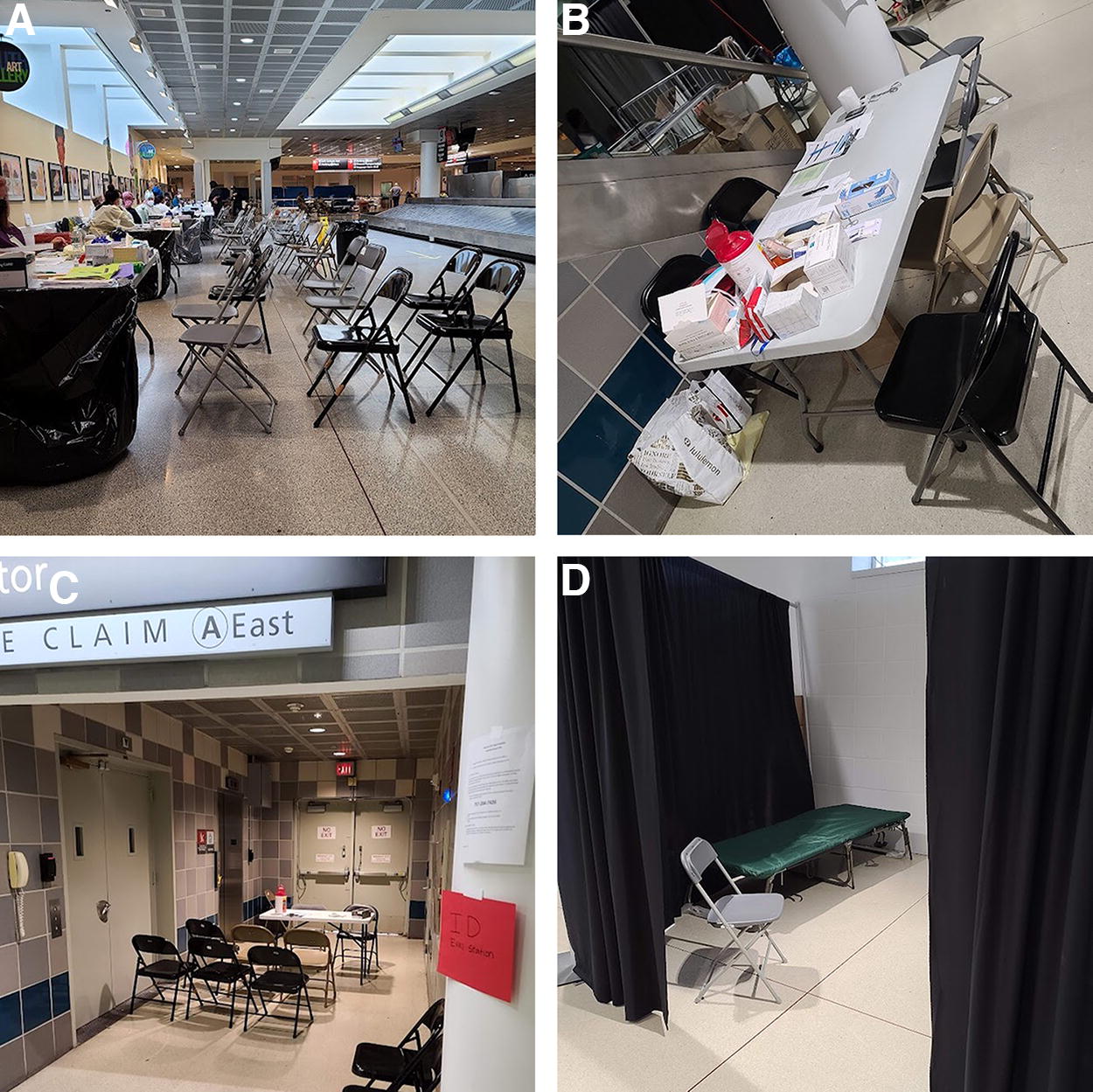
Medical triage area, Baggage Claim A, Philadelphia International Airport (PHL). Images demonstrating the layout of the medical triage area at PHL.

MTU map. Process map outlining the basic flow of patients through the medical triage area.
Logistical support to troubleshoot MRC enrollment, arrange for the purchase and transportation of needed supplies and medications, and meet other needs to support the medical team was provided by local health department staff who volunteered for this assignment.
Equipment (Table 3) was brought in to facilitate basic physical exams. These exams were focused on the chief complaint of the presenting patients. Vital signs and diagnostic testing were done as indicated to evaluate the presenting issues. The MTU could also perform basic diagnostics and minor procedures to reduce the need for hospital transfers for nonemergent issues.
Supplies
OAW Color-Coded Wristbands for Individuals Requiring Specific Follow-up Care
OAW, Operation Allies Welcome.
Medications were available in a small onsite medical dispensary, including medications to treat minor ailments, as well as commonly used outpatient medications to provide to refugees who may arrive without adequate supplies of their home medications. Medications for the onsite formulary during OAW were selected based on the likelihood of encountering a particular medical condition (e.g., common pediatric rashes and febrile illnesses) as well as the likelihood of rapid decompensation if a patient did not have access to a medication (e.g., common diabetes and antiepileptic medications) as chronic noncommunicable diseases account for a significant morbidity burden in refugee populations. 23 Overall, 1363 prescriptions were dispensed on-site during OAW. The majority were for over-thecounter analgesics, antacids, prenatal vitamins, and antibiotics for common mild infections (e.g., amoxicillin). If a patient urgently required medications not available onsite (e.g., blood thinners and cardiac medications), a prescription was called in by the evaluating provider to a local pharmacy and a volunteer was dispatched to obtain the medication and provide it to the patient before they left the airport. Emergency medical insurance was provided by HHS.
Clinical Care and Patient Flow
Patient identification
The processing of patients through the MTU (Fig. 2) began prior to any arrivals, with a review of medical assessments done at the point of origin. Any available records were transported with the patient. If a medical evaluation at the point of origin identified any particular medical concerns, this information was communicated to the medical and operations team leaders daily to ensure appropriate resources were prepared to greet the patient on arrival. This information was also communicated to customs and immigration personnel to ensure patients requiring urgent medical attention went through expedited processing.
On arrival at the airport, all evacuees went through customs and immigration. This process took a variable amount of time depending on the evacuee’s immigration status and what documents they possessed. Processing times through customs during OAW ranged from 1 hour to over 24 hours. Because of this prolonged time period, there were several medical emergencies within the secured area. Given security concerns, coordination with Customs and Border Patrol (CBP) and TSA agents and paramedics was required to ensure prompt care of any evacuees experiencing a medical emergency during customs. Existing airport emergency medical service units, who possessed all needed security clearances to enter the secure area, conducted an initial evaluation and determined if more care was needed. If such a determination was made, the evacuee could be brought to the MTU accompanied by a CBP agent for medical assessment and stabilization. If the patient was subsequently cleared, they could return to customs; if it was determined that the patient required transfer to a local hospital, the patient and their family were accompanied to the hospital by a CBP agent until they were stabilized and returned to the airport for further processing.
If no preidentified medical issue or en route emergency existed, evacuees were processed through customs and immigration. On completion of this process, they were offered the opportunity to see a physician and were asked screening questions related to infectious diseases of public health concern. This evaluation primarily focused on COVID-19 but was ultimately expanded to include infectious diarrheal illnesses and measles after several cases were identified at points of origin. 24 Any patients screening positive were tested and then brought to an isolated area of the MTU for evaluation. In addition, infants under 30 days old and expectant mothers at >36 weeks gestational age were brought to the medical triage area for a brief assessment, regardless of whether there was a specific medical complaint, as these populations are at high risk for the development of complications related to prolonged travel.
MTU process
All patients seeking or sent for medical evaluation were brought to the MTU with their entire family group. Triage was performed by the medical team lead, who conducted a brief visual assessment, gathered information on patient age and chief complaint, and routed the patient to an appropriate provider based on the patient’s complaint, the provider’s specialty, expected diagnostic or therapeutic resources needed, and patient preferences regarding the gender of the provider to ensure culturally conscious care. 25 If a same-gender provider was not available when a patient requested one, the medical team lead arranged for a same-gender chaperone to be present for the exam to increase patient comfort. The family remained together during the entire evaluation unless the patient required a diagnostic test or procedure, in which case they were briefly brought to a separate screened area while their family waited at the provider’s table. Families were kept together as much as possible to avoid retraumatizing a vulnerable group of individuals who have every reason to fear separation from their family members.
Providers made every effort to use available resources to address patient concerns onsite, including managing minor illnesses or injuries, performing minor care procedures, and dispensing common prescription medications if available. Point-of-care ultrasound (POCUS) examinations were performed by either emergency medicine or OB/GYN trained providers using a Butterfly iQ or Philips Lumify handheld ultrasound device. Common indications included abdominal pain, pregnancy-related concerns (e.g., pain or bleeding in early pregnancy or confirmation of gestational age to determine appropriate follow-up care), shortness of breath, leg swelling, and skin and soft tissue infections. These studies allowed providers onsite to rule out emergent pathologies such as ectopic pregnancy or deep venous thrombosis and to diagnose conditions treatable onsite such as skin abscesses, preventing unnecessary hospital transfers. 26 Images were stored on the ultrasound device, and the results of the study were recorded in the patient’s chart. POCUS trained physicians reviewed images to ensure the correct diagnoses and care were given to the patient.
Provider assessments included follow-up planning for ongoing care. Any patient requiring specific follow-up was flagged with a color-coded wrist band and sticker (Table 4) and the specialty and urgency of that follow-up were documented in the patient’s chart, which traveled with them. These follow-up decisions impacted which base the evacuee could be transferred to for further processing, as not all bases had access to specialized medical care. Identifying and flagging patients requiring close follow-up ensured that they and their family were placed in a location where they could continue to receive appropriate medical care in an outpatient setting. At the end of each shift, warm handoff was given to medical staff at each destination point to ensure receiving medical staff were aware of incoming patients with specific needs.
This process of flagging individuals for necessary follow-up also included individuals who did not seek medical care from the MTU. Infants <30 days of age, pregnant women at >24 weeks gestational age, or individuals with a significant mobility impairment were identified by staff after customs, and their documents flagged with a color-coded indicator to assist with appropriate placement (Table 3).
Once patients were cleared by the health care provider evaluating them, they continued through the process at the airport until they had a destination site designated and transportation was available. Some evacuees had prolonged lengths of stay on site at the airport as they awaited transport to an appropriate resettlement facility or other location. The MTU was at times called upon to provide ongoing care for these individuals as well. Operations staff responsible for the needs of those still at the airport, including food, water, and sleeping arrangements, could bring individuals to the medical team lead for assessment.
Off-site operations
If a patient presents with an urgent medical issue that could not be appropriately managed onsite or wait for outpatient follow-up, the evaluating provider alerted the medical team lead who coordinated a hospital transfer.
For unstable patients, emergency medical services (EMS) was called to assess the patient and immediately transport them to the nearest emergency department. If the patient was stable, then the medical team lead could work with operations staff to initiate the transfer process. The medical team lead would select an appropriate facility based on their knowledge of the local medical environment, accounting for capacity and any specialty services that may be needed, and would call the transfer center for the facility receiving the patient, taking care to load balance among area hospitals to avoid overburdening any facility. They provided warm handoff to the receiving physician and also communicated with hospital staff any special considerations to ensure culturally aware care of the patient and their families. This at times included negotiations with hospital administrators to allow larger numbers of visitors than is typical to avoid separating families and other similar accommodations. The medical team lead ensured that transportation was available for the families of patients regardless of whether the patient themselves was transported by ambulance or by other means. Stable patients were sometimes transported by operations staff if there was no need for an ambulance, and their families were brought with them. Meticulous documentation of each individual traveling to the hospital with the patient was kept by the medical team lead to ensure families were kept together and returned to processing once the patient was discharged from the hospital. Interpreters accompanied all patients sent to the hospital.
To facilitate returning patients and family members to the airport, all local hospital transfer centers were provided with the contact information for the medical team lead phone, and the medical team lead would inform the treating physician at the receiving hospital that a call to the medical team lead was necessary when the patient was being prepared for discharge. Once they received a call that the patient was being discharged, the medical team lead worked with operations staff to arrange for transport of all individuals either back to the airport if additional processing was needed or onward to an appropriate site with access to any necessary follow-up care. Any new medical information or follow-up care needs resulting from the hospital visit were communicated to the receiving destination during the daily warm handoff call to ensure ongoing care of the patient.
Documentation
Individual patient charts completed by each provider were copied, with one copy being sent with the patient and another being kept securely by the medical team. In addition to these charts, the medical team lead provided a daily summary to the operations command team including total number of patients seen, hospital transports and returns, any patients still admitted to area hospitals awaiting discharge, and the number of patients designated for specific sites.
Discussion
OAW serves as an example of a highly successful onsite medical triage operation during a mass evacuation event. The MTU was able to efficiently and thoroughly evaluate a total of 1598 patients while limiting hospital transfers to only 85 individuals and mitigate the impact of a large influx of evacuees on a local health care system already stretched beyond its limit by the ongoing COVID-19 pandemic.
The MTU was rapidly initiated by PDPH engaging local physician leaders with a background in refugee health and global disaster response. PDPH assumed the responsibility of logistical and operational support, and the MRC provided registration and organization of volunteers; however, an onsite MTU was not initiated, organized, or established by any federal agency, despite the existence of the HPP and local HCCs and Federal Coordinating Centers (FCCs) that could in theory have provided many of the services provided by the MTU if this event was a designated disaster. Instead, the MTU was locally organized, managed, and supported by PDPH in coordination with DHS, TSA, and other federal partners. This event highlights a gap in the HCC/FCC model of disaster preparedness and response considerations and the dependence of operations like this on local health care providers who are generally not involved in the planning and preparation for emergency responses, which is currently being further evaluated by DHS with federal and local partners.
The nature of mass migration and refugee crises is that there is often very little time to prepare and predict complications that may impact operations. Sharing this approach is intended both as a rationale for higher level involvement of local frontline health care workers in the planning and preparation for nondisaster rapid response needs, as well as a guide for municipalities to create their own response plans for mass migration events, which are expected to occur more and more often as climate change and global political unrest force displacement of large groups. We can anticipate that in any mass displaced person event, there will be people who become separated from life sustaining medications and others who are injured or become ill in transit. Providing timely, culturally sensitive care on site at arrival points can avoid complications and prevent overloading of local health care systems.
Footnotes
Acknowledgments
This paper is dedicated to the men, women, and children of the Kabul Airlift, and to those who were left behind. The authors would like to thank the many individuals who volunteered their time and extraordinary efforts to the medical triage unit.
Authors’ Contributions
E.R.K.: Writing—original draft (lead), writing—reviewing and editing (lead), editing (lead), project administration, and visualization. M.S.: Editing, project administration, supervision, and visualization (lead). C.B.: Editing, project administration, supervision, and resources (lead). S. Myers: Editing, project administration, and supervision. S. Mohammadie: Writing—original draft. N.R.: Editing and project administration. P.H.: Project administration (lead), editing, and supervision (lead).
Author Disclosure Statement
The authors have no competing interests or personal financial interests to disclose.
Funding Information
This work was not funded by any grants. Some administrative staff were paid in part by the PDPH for their time. The remainder of the work was unfunded and undertaken by volunteers.